
Abstract
Goals:
To assess the long-term results of transoral incisionless fundoplication (TIF 2).
Background:
TIF with the EsophyX2 is an accepted procedure to treat gastroesophageal reflux disease (GERD). Long-term data have been limited. We report clinical outcomes of 151 patients followed up to 9 years.
Study:
A single institution prospective registry of patients undergoing TIF 2 between 11/2008 and 7/2015. Outcomes were assessed by complications, re-interventions, and a mixed effect model of clinical response over time.
Results:
A total of 151 patients (87 women), mean age 62 years (30–91), mean body mass index (BMI) 26.6 (20–36.1), 93% on daily proton pump inhibitor (PPI), underwent TIF 2 without hiatal hernia repair; 131 of the 151 patients (86%) were available for follow-up at a median of 4.92 years (0.7–9.7 years). Of 120 patients ⩾5 years post-TIF, 62 (51%) were followed for a median 6.8 years. Median GERD-health-related quality of life (HRQL) scores decreased from 21 (interquartile range (IQR) 9.5–30) off PPI and 14 (4–24) on PPI at baseline to 4 (2–8) at 4.92 years and remained at 5 (2–9) in the 62 patients 5–9 years post-TIF. Sixty-four per cent had successful (>50%) reductions in GERD-HRQL scores at 4.92 years and 68% of patients followed ⩾5 years. Median regurgitation decreased from 15 (8–20) off PPI and 11 (5–20) on PPI at baseline to 0 (0–4) at 4.92 years, remaining at 1 (0–3) in 62 patients 5–9 years post-TIF. Mixed model analyses confirmed significant and stable improvements in GERD-HRQL and regurgitation scores at all annual follow-up time points after TIF. Daily PPI use decreased from 93% to 32% at 4.92, and 22% at ⩾5 years post-TIF. Revision to laparoscopic fundoplication in 33(22%) showed comparable outcomes. Two patients recovered uneventfully after laparoscopic surgery for localized perforation.
Conclusions:
TIF 2 provides durable relief of GERD symptoms at up to 9 years with 69–80% of patients having a successful outcome by symptom response and PPI use.
Introduction
Gastroesophageal reflux disease (GERD) treatment modalities are changing. Although proton pump inhibitor (PPI) has been the primary treatment modality, increasing recognition of PPI limitations – especially in regard to incomplete symptom control and potential long-term side effects associated with chronic PPI usage – helps define a need for other approaches to treat GERD. 1 As the necessary precondition for GERD is a defect in the mechanisms for controlling the reflux of gastric contents into the esophagus (variously called the lower esophageal sphincter or gastroesophageal valve or antireflux barrier), mechanical solutions to this defect are generally considered the most effective method of addressing GERD, albeit accompanied by potentially greater risks than PPI therapy. 2 Laparoscopic Nissen fundoplication has historically been the most common procedure; however, the side effect profile of gas bloat, diarrhea, and dysphagia have reduced its popularity and leaves an opportunity for other interventions.3,4 Novel techniques to restore the antireflux barrier have sought to balance minimal invasiveness, efficacy with safety and minimal side effects.
Transoral incisionless fundoplication (TIF) in the latest iteration, TIF 2.0, has shown promise in providing reasonably effective control of GERD symptoms with a minimal side effect profile Although appropriately termed a ‘fundoplication’, TIF does not create the supra-physiological flap valve of a Nissen procedure; gas bloat and dysphagia have been very uncommon side effects of TIF. Short-term success at alleviating heartburn and regurgitative symptoms has been reported in 60–80% range in multiple series.5–7 Long-term studies have confirmed the same results; however, on a relatively small number of patients.8,9
We report follow-up of up to 9 years on a consecutive series of 151 patients undergoing TIF by a single procedural team between 11/2008 and 7/2015, using the EsophyX2 device (Endogastric Solutions, Inc., Redmond, WA, USA) using a variation of a technique (called TIF 2.0), details of which we have previously described. 10
Materials and methods
Study population
A total of 151 patients with objectively documented GERD underwent primary TIF (without hiatal hernia repair) at a single institution between November 2008 and July 2015. Patients provided written informed consent. When written informed consent could not be obtained, patients provided verbal consent which was documented.
All patients were enrolled in a prospective, Western Institutional Review Board (WIRB) approved registry (study no. 1185349) and data were maintained in a secure Microsoft Access database. Baseline demographics included age, gender, body mass index (BMI), use of PPI, and preoperative objective studies. Baseline GERD-specific health-related quality of life (HRQL) surveys, and a regurgitation-specific questionnaire used in other TIF studies were obtained with patients on and/or off PPI. The GERD-HRQL consists of 10 questions (six regarding heartburn, two on dysphagia, one on abdominal bloating, and one regarding medication use), scored 0 (no symptoms) to 5 (incapacitating to do daily activities), range 0–50. The regurgitation-specific questionnaire uses the same GERD-HRQL scoring system with the six questions specific to heartburn in the GERD-HRQL replacing ‘heartburn’ with ‘regurgitation’, range 0–30. A decrease of >50% in a score results in the intervention being considered successful. 11 Detailed operative and postoperative data were collected. Routine follow-up using the same surveys was initially performed for 2 years after the procedure. Beginning in 2018, with institutional review board (IRB) approval, patients were again contacted and asked to complete the same quality of life surveys, as well as questions regarding postoperative interventions.
Study design and endpoints
Clinical response assessed by GERD-HRQL and regurgitation scores used in prior TIF studies, use of PPI, perioperative complications, and need for re-intervention were primary outcome measures.
Preoperative evaluation
Patients underwent preoperative upper gastrointestinal endoscopy to assess both axial height of hernia and transverse hiatal dimensions, as well as for the presence of esophagitis or Barrett’s esophagus. Ambulatory reflux testing either by 48-h telemetry capsule pH testing off PPI, or 24-h transnasal impedance/pH testing (off PPI in the majority of patients) was performed to document excess esophageal acid exposure. An abnormal percentage time with pH <4 in 24 h of >5.2% total, >6.1% upright, >2% supine, a DeMeester score >14.72, or >53 reflux episodes per 24 h were considered objectively diagnostic of GERD. High resolution impedance manometry was performed in the majority of patients and in any patient reporting preoperative dysphagia or chest pain.
Inclusion/exclusion criteria
Inclusion criteria included patients ⩾18 years of age who were able to provide informed consent and consented to TIF, and who had objective documentation of GERD. Exclusion criteria included axial hernia height >2 cm, Los Angeles classification C or D esophagitis, Barrett’s esophagus defined as visible columnar lined (⩾1 cm) esophagus demonstrating intestinal metaplasia on biopsy.
Treatment
TIF was performed under general anesthesia with complete muscle relaxation in the main operating room (95%) or endoscopy suite (5%). We have previously described the technique, 12 complete upper endoscopy re-evaluated for appropriateness for TIF procedure. No patients in this report underwent concomitant hiatal hernia repair.
Flexible endoscopy was performed to confirm appropriate patient selection and to measure the distance to the diaphragmatic hiatus. Esophageal bougienage to 56 Fr was performed, the EsophyX2 device placed over the endoscope and passed into the stomach under direct visualization. The endoscope was brought back proximal to the tissue mold until the tissue mold could be retroflexed under direct vision. The procedure was then performed with both tissue mold and flexible endoscope in retroflexion. A ‘roll’ technique was employed: using a combination of caudal retraction with the helical retractor, gastric desufflation and rotational movement of the tissue mold, the fundus of the stomach was partially rotated around the distal esophagus. Closure of the tissue mold with the invaginator on was followed by external advancement of the device (to which the esophagus was adherent by suction) to reduce the hernia and ensure that fastener deployment would be below the hiatus. The fundus was then plicated to the distal esophagus and fixed in place with multiple 6.5 mm H-shaped polypropylene fasteners. The roll technique with a single engagement of the helix retractor at the 12 o’clock position on the lesser curvature was repeated in multiple locations to create an internal fundoplication of approximately 270° circumference. The device was then removed under direct vision, and subsequent endoscopy performed to confirm hernia reduction, evaluate degree and length of fundoplication, and evaluate any potential complications.
Anterior-posterior (A-P) and transverse dimensions of the hiatus were recorded as well as fastener deployment at four locations: anterior (12:00–01:00), mid-anterior (02:00–03:00), greater curve (04:00–06:00), and posterior (10:00–11:00), Figure 1.

Clock-face definitions and hiatal dimensions.
Fastener deployment was recorded by position. With the lesser curve considered 12:00 as in Figure 1. Anterior deployment was between 12:00 and 01:00, mid-anterior between 02:00 and 03:00, Posterior between 09:00 and 11:00, and greater curve from 04:00 to 07:00. The number of fasteners deployed by location is illustrated in Figure 2. The resulting height of fasteners above the squamo-columnar junction (lip of valve), by location, is illustrated in Figure 3.

Number of fasteners deployed by location.

Height of fasteners above squamo-columnar junction by location (cm).
Final retroflex inspection after the device was removed estimated the degree of wrap between the onset of the plication folds, Figures 4 and 5.

Determination of degree wrap at completion of transoral incisionless fundoplication (TIF).

Degree wrap at completion of transoral incisionless fundoplication (TIF).
Patients were discharged when they achieved adequate pain and nausea control and tolerated a liquid diet.
Patient categorization
Patients who underwent revision to laparoscopic fundoplication due to failure of TIF to control GERD are reported for comparison.
Statistical methods
Data were reported as mean (standard deviation) or median with range or interquartile range (IQR) as appropriate. Data were analyzed using t tests for continuous data and Fisher’s exact test for categorical data. A mixed effect model was used to assess the changes in treatment effect on quality of life measures (GERD-HRQL and regurgitation scores) in terms of testing mean differences, a p-value less than 0.05 was considered statistically significant. All mixed models were fitted in SAS software version 9.4 (SAS Institute, Inc., Cary, NC, USA). All other analyses were performed using XLSTAT and JMP software.
Results
Patient demographics and procedures performed
One hundred and fifty-one patients (87 women, median age 62 years (range 30–91), median BMI 26.6 (range 20–36.1), underwent TIF during the study period.
The average duration of symptoms prior to TIF was 11.3 years (range 0.15–24.2). Daily PPI use prior to TIF was reported by 93% (140/151) of patients with 30% having taken 80 mg/day. Seventy-eight per cent of patients reported moderate to severe ongoing GERD symptoms preoperatively despite PPI therapy.
Eighty-eight per cent (132/151) underwent baseline ambulatory pH testing; 97% (128/132) of those tested demonstrated abnormal esophageal reflux, Table 1.
Baseline ambulatory reflux testing in 132 patients, median (range).

PPI, proton pump inhibitor.
Baseline manometry performed on 101 patients demonstrated normal esophageal body peristalsis (distal esophageal amplitude >35 mmHg with >70% of swallows peristaltic) in 91 (91%).
Baseline (sedated with spontaneous respiration) and intraoperative (general anesthesia with positive pressure ventilation) endoscopy findings were available for 120 of the 151 TIF patients. As hernia height is dynamic, hernia axial dimensions were categorized by range, Table 2.
Available endoscopic axial hernia height ranges preoperatively (sedated) and intraoperatively (general anesthesia, positive pressure ventilation).

Two patients with preoperative >2 cm reducible hernia underwent transoral incisionless fundoplication due to patient request (protocol deviation).
Three patients at surgery were found to have axial hernias of 3 cm (2) and 4 cm (1). These patients were early in our experience and currently would not have a completed procedure.
Positive pressure ventilation, as would be expected, was associated with a decrease in the axial hernia dimensions.
Preoperatively a Hill grade 1 valve (lip of valve tight around endoscope on retroflexion) was present in one patient, a Hill grade 2 (lip of valve loose around endoscope and moves or opens with respiration) in 118/120 (98%) of patients, and a Hill grade 3 (ridge is effaced and hiatus is patulous) in one patient. Intraoperative Hill grade was not recorded.
Operative procedures
Median operative time for TIF was 55 min (range 25–124). Mean estimated blood loss was 3.6 cc (range 0–100 cc).
Intraoperative hiatal dimensions are recorded in Table 3.
Intra-operative hiatal dimensions, percentage of patients.

Axial hernia height was ⩽2.0 cm in these patients.
Three patients at surgery were found to have axial hernias of 3 cm (2) and 4 cm (1). These patients were early in our experience and currently would not have a completed procedure.
A-P, anterior-posterior.
A-P and transverse dimensions frequently exceeded the axial hernia height recorded intraoperatively or even preoperatively.
The median number of fasteners deployed was 20 (range 12–40, IQR 20–26).
Hill grade 1 was seen at completion of TIF in 98% (105/107) patients, with a Hill grade 2 in one patient and Hill grade 3 in one patient.
Postoperative course
The majority of patients were discharged within 24 h. Five patients had prolonged retching/vomiting requiring more than 8 h of intravenous antiemetics.
Adverse events
An immediate postoperative esophagram demonstrating leak in one patient with suspected esophageal perforation led to prompt laparoscopic evaluation, suture repair of the perforation, laparoscopic anterior fundoplication to cover the repair, and an uneventful postoperative course.
One patient with postoperative vomiting who demonstrated an elevated white blood cell count on postoperative day 1 with a negative computed tomography (CT) scan was treated with antibiotics and recovered uneventfully. One patient presented 7 days postoperatively with chest pain; CT scan was consistent with a mediastinal abscess confirmed by esophagram. Laparoscopic transhiatal drainage of the mediastinal abscess, takedown of the TIF, repair of esophagus, and laparoscopic fundoplication resulted in an uneventful recovery. One patient with interstitial lung disease was hospitalized for 5 days for hypoxemia, and one patient developed a prolonged ileus requiring 3 days hospitalization.
Laparoscopic revision
Thirty-three (22%) of TIF patients underwent laparoscopic revisional surgery at a median of 14.7 months after surgery (3–86). All revisions were accomplished without perioperative complication; details have previously been reported. 13 Long-term quality of life outcomes were equivalent to those patients who did not undergo reoperation.
Quality of life results
Clinical follow-up was obtained in 131 (87%) of 151 total patients at a range 0.7–9.7 years (median 4.92 years, IQR 3–6.8). Five years or greater follow-up was obtained on 51% (62) of the 120 total patients 5 years or more out from surgery (median follow-up 6.8 years, range 5–9.7 years). The median GERD-HRQL scores decreased from 21 (IQR 9.5–30) off PPI and 14 (4–24) on PPI at baseline to 4 (2–8) at 4.92 years, and remained 5 (2–9) in the 62 patients 5 to 9 years post-TIF. Successful (>50%) reductions in GERD-HRQL scores were seen in 64% at 4.92 years and 68% of patients followed for ⩾5years. Median regurgitation decreased from 15 (8–20) off PPI and 11 (5–20) on PPI at baseline to 0 (0–4) at 4.92 years, and remained 1 (0–3) in 62 patients 5 to 9 years post-TIF. GERD-HRQL and regurgitation scores at baseline and by year post-TIF are shown in Figure 6.

GERD-HRQL and regurgitation scores at baseline and by year post-TIF. Numbers of patients with available data are noted below.
Table 4 shows the results of mixed model analyses for the GERD-HRQL score at different time points. This analysis shows a significant improvement in the GERD-HRQL score at different time points when compared to the preoperative baseline values.
Mixed model for GERD-HRQL score by time point.

GERD-HRQL, gastroesophageal reflux disease-specific health-related quality of life.
Table 5 shows the results of pairwise comparison of GERD-HRQL for each two consecutive years. All of the comparisons resulted in no significant difference in GERD-HRQL score at time points from 1 year to 9 years, indicating that the favorable outcome after TIF did not change over time.
Pairwise comparison based on the GERD-HRQL score mixed model.

GERD-HRQL, gastroesophageal reflux disease-specific health-related quality of life.
The results of similar comparisons for the regurgitation score are shown in Tables 6 and 7. These analyses show a significant improvement in regurgitation score at each time point from 1 to 9 years when compared to preoperative baseline values using a mixed model (Table 6).
Mixed model for regurgitation score by time point.

Pairwise comparison based on the regurgitation score mixed model.

Similarly, all of the pairwise comparisons with the exception of one comparison (5 years versus 4 years) resulted in no significant difference in regurgitation score (Table 7), indicating that the improvement in regurgitation following the procedure does not change over time.
Over 70% of patients reported a >50% improvement in quality of life as measured by the GERD-HRQL score at all time points through 8 years of follow-up, Figure 7.

Percentage of patients with >50% improvement in GERD-HRQL by year post-TIF.
Daily PPI use was reported in 93% of patients preoperatively; throughout follow-up approximately 70% of patients remained free of the daily use of PPIs, Figure 8.

Percentage of patients free of daily PPIs by year post-TIF. Number within bars represent total number of patients reporting by year.
GERD-HRQL scores were similar between patients who continued to take PPI therapy (median 6, IQR 3–16) and those who were off PPI therapy (median 2, IQR 0–7, p = 0.09) at 4.92 years’ follow-up.
Dysphagia
Dysphagia assessed by GERD-HRQL (scored 0–10) decreased from a median of 2 (IQR 0–4) preoperatively to a median of 0 (0–2) at a median 4.92 years’ follow-up (p < 0.0001).
Bloating, vomiting, belching
As in other studies of TIF, abdominal bloating or distention as measured by GERD-HRQL (scored 0–5) decreased after TIF at 4.92 years’ median follow-up, in this case from a median of 2 (IQR 0–4) to 1 (IQR 0–2), p < 0.001.
Ability to vomit was preserved in 95% (42/44) of patients who reported a need to vomit, and ability to belch in 90% (57/63) at 4.92 years’ median follow-up.
Discussion
TIF using the EsophyX2 device has demonstrated an subjective and objective improvement in GERD in multiple single-arm and randomized controlled trials. Criticism remains, however, regarding its long-term durability as the majority of studies have been short term. Long-term studies to date are favorable in relatively small cohorts of patients.
This study analyzed prospectively collected data on a cohort of 151 patients who underwent TIF with the EsophyX2 device between November 2008 and July 2015. We report the median follow-up on 131 of these patients of 4.92 years with 5 years or greater on 62 of 120 patients 5 or more years out from surgery. GERD-HRQL and regurgitation scores improved significantly from baseline and remained stable through 9 years of follow-up. The results of our mixed model showed significant improvement in both GERD-HRQL and regurgitation scores at different follow-up time points. In addition, the mixed effect model confirmed no changes in the effect of TIF on these quality of life measures over time. At a median of 4.92 years’ follow-up, ⩾50% reduction in GERD-HRQL and regurgitation scores were seen in 64% and 76% of patients, respectively. Approximately 70% of patients remained free of daily PPI use through the 9 years of follow-up and were symptom free. As these patients were cared for in a foregut surgery practice, 22% of patients failing TIF wished to undergo revisional laparoscopic fundoplication and did so safely without detriment to their long-term outcomes.
One may argue that a limitation of our study is incomplete follow-up on all patients that may result in selection bias in this longitudinal dataset. However, we used a mixed effect model to analyze the data to address the potential selective drop-out. This method of analysis copes with missing data points while still accounting for variability within and across study participants. Another potential limitation of the study is the lack of long-term objective outcome data, specifically with regard to esophageal acid exposure. However, prior studies of antireflux procedures have shown little if any correlation between symptomatic improvement and postoperative pH changes. 14
Techniques involving the EsophyX2 device have evolved over time and the TIF 2.0 technique described by Hoppo et al. 15 and modified by Bell and Cadiere 10 have been widely adopted. This current study adds to the reports regarding the modified TIF 2.0 technique. What is not often appreciated in descriptions of the TIF 2.0 technique is the degree to which the fundus is physically rotated around the distal esophagus, something that can only be seen with simultaneous laparoscopy, as illustrated in Figure 9. We believe the device and technique modifications since 2011 will increase the overall success of the TIF procedure by enabling more reproducible fastener deployment and a greater degree of anterior rotation.
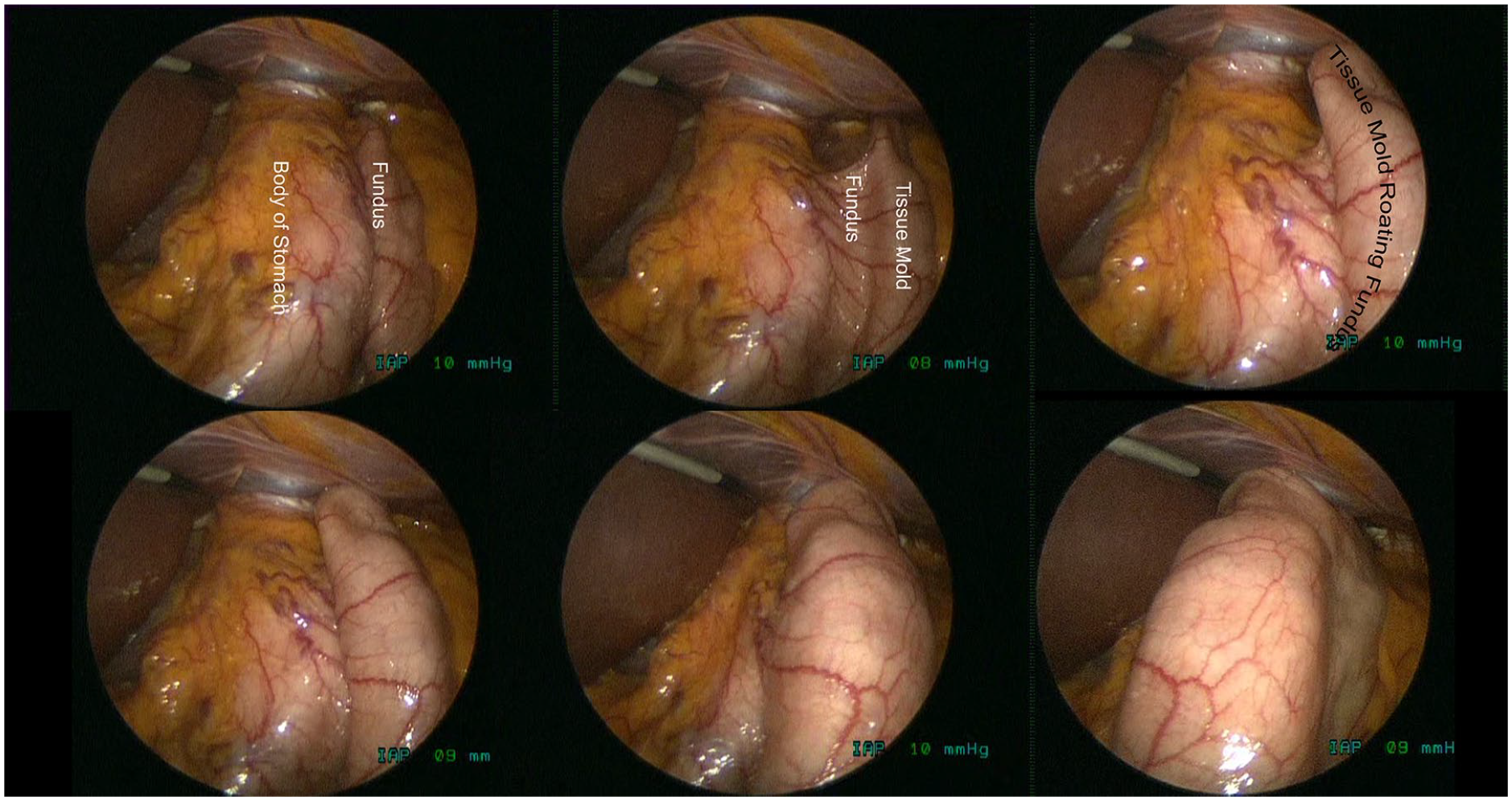
Laparoscopic sequential view of anterior rotation of EsophyX tissue mold, beginning with fundus lateral to stomach (top left) to fundus anterior to stomach (bottom right).
Despite previously published long-term follow-up with the TIF procedure, concern about the durability of TIF persists.16,17
Trad et al. reported resolution of regurgitation in 86% and freedom from daily PPI use in 66% of 44 patients at 5 years post-TIF, with three patients undergoing reoperation. 9 Chimukangara et al. reported on 23 of 57 patients in whom follow-up was obtained at a median of 8 years: GERD-HRQL decreased from 24 to 10, 27% stopped daily PPI use, and 21% underwent laparoscopic revisional surgery. 18 Testoni et al. followed 50 TIF patients for up to 10 years: GERD-HRQL scores decreased from a median of 45–10 at 5 years and remained stable at 10 years, and 73–91% of 41–14 patients followed at 5–10 years, respectively, had stopped or halved their PPI dosing. Seven patients (14%) underwent subsequent laparoscopic revisional surgery. 8
We undertook the current study based on the above studies, as we had stopped routine follow-up on our TIF patients and had seen a drop off in our TIF volume. The findings were, honestly, more positive than we expected. In particular, that 75% of patients reported excellent GERD-related quality of life, and that almost three-quarters did not require any PPIs was impressive.
Conclusions
Long-term outcomes of 151 patients undergoing modified TIF 2.0 with the EsophyX2 device demonstrate durability of the procedure out to 9 years. GERD-HRQL and regurgitation scores improved following TIF and remained stable, and at a median of 4.92 years 69–80% of patients had a successful outcome by symptom response and PPI use.
Footnotes
Author contributions
The authors had sole authority for, and received no remuneration for data analysis, interpretation, or writing of the manuscript.
Conflict of interest statement
Research support for data collection provided by EndoGastric Solutions, Inc., Redmond, WA, USA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.