
Abstract
Background:
The incidence of Clostridioides difficile infection (CDI) is increasing in the general population. Data on the epidemiology of CDI in peripartum women – a highly vulnerable patient population – is scarce. The objective of this study was to report the incidence of CDI in peripartum women.
Methods:
A single-center retrospective cohort study was conducted in peripartum women from 1997 to 2017. Peripartum CDI was defined as definite CDI (watery diarrhea for >24 h with positive stool assay) during pregnancy, or within 6 weeks postpartum. Incidence was reported per 100,000 pregnancies and time trends in incidence were analyzed using Poisson regression. Analyses were done separately for time trends before and after 2007, when CDI testing strategy changed to polymerase chain reaction.
Results:
From 1997 to 2017, 80 patients with peripartum CDI (47 during pregnancy, 33 postpartum) out of 125,683 pregnancies (0.064%) were identified. Incidence of CDI increased 3.4 fold (95% confidence interval 1.5–7.4, p = 0.005) over the 21 year period. Time trends were evident after (p = 0.054), but not before 2007 (p = 0.97).
Conclusion:
Incidence of CDI in peripartum women increased over the 21 year study period. The rise in incidence is concerning, and calls for heightened surveillance for CDI in this highly vulnerable population.
Introduction
The incidence of Clostridioides difficile infection (CDI) is increasing in the United States (US), though it is stable or decreasing in different regions in Europe.1–5 Young adults, including peripartum women, have previously been thought to be at low risk for CDI. Recent studies in the US using national datasets have demonstrated an increasing incidence of peripartum CDI.6,7 These studies have used data from inpatients only, and have data up to 2013. With the increasing incidence of CDI in the general population and a rise in community-acquired cases, we aimed to provide comprehensive and updated data on peripartum CDI. The objective of this study was to assess the incidence and risk factors of peripartum CDI in a single-center cohort.
Methods
Study population
All pregnant women at the Mayo Clinic from 1997 to 2017 (population used to calculate incidence), who did not deny research authorization for access to medical records, were eligible for inclusion. Cases were identified using CDI diagnostic codes and confirmed by reviewing the medical records. Peripartum CDI was defined as: watery diarrhea for >24 h with positive stool assay [toxin enzyme immunoassay (EIA) or polymerase chain reaction (PCR)] during pregnancy, or within 6 weeks postpartum. The first CDI episode during pregnancy was included. Risk factors for CDI within the prior 90 days were recorded. Mode of acquisition of CDI was defined according to recently published guidelines by the Infectious Diseases Society of America and Society for Healthcare Epidemiology of America. 8 CDI was categorized as healthcare facility-onset (HO) if it occurred >3 days after hospital admission, community-onset healthcare facility-associated (CO) if within 4 weeks of discharge, community-associated (CA) if there was no inpatient stay within 12 weeks, indeterminate if hospital discharge was within 4–12 weeks, and unknown if data were inadequate to classify. Healthcare-associated (HA) CDI included both HO- and CO-CDI.
Statistical analysis
Incidence was reported per 100,000 pregnancies and time trends were determined using Poisson regression. Incidence and time trends were analyzed for peripartum CDI, and for CDI during pregnancy or postpartum separately. Analyses of trends in incidence of CDI before and after 2007 (when testing was switched from EIA to PCR) were performed as PCR has higher sensitivity and could lead to increased detection. Fisher’s exact test was used to compare antibiotic exposure in patients with vaginal versus cesarean delivery (among postpartum CDI cases). Statistical analyses were performed using JMP Pro 14.1.0 and SAS version 9.4. Two-tailed p-value < 0.05 was considered statistically significant.
Results
From 1997 to 2017, 80 cases of peripartum CDI (47 during pregnancy, 33 postpartum) out of 125,683 pregnancies (0.064%) were identified; median age was 27 years (range 20–41); 90% were Caucasian. Six patients (8%) had history of prior CDI. Timing of CDI during pregnancy and risk factors for CDI is outlined in Table 1.
Description of cases with peripartum Clostridioides difficile infection.

Data presented as number (%) and as percentage of patients with available information.
CA, community associated; CDI, Clostridioides difficile infection; CO, community onset healthcare facility associated; HA, healthcare associated; HO, hospital onset.
Outpatient/emergency room visits (83%) and antibiotics (70%) were the most common risk factors within the 90 days prior to the CDI episode. Overall, 48 (61%) patients had prior hospitalization as a risk factor for CDI. Amongst these, 27 (56%) patients had a pregnancy-related hospitalization: for delivery of child in 25 patients, preterm labor in 1 and endometritis in 1 patient. Amongst patients with CDI in the postpartum period, 15 (48%) patients had a vaginal delivery, 16 (52%) patients had a cesarean delivery and 2 patients did not have data on mode of delivery. The proportion of patients exposed to antibiotics was similar in those who had vaginal and cesarean delivery [11 (73%) versus 13 (81%), respectively; p = 0.68]. The majority of cases (47%) were HA, while 30% were CA. Overall, 15% patients (n = 12) had CDI within the immediate peri-partum period (within 7 days of delivery).
Over the 21 year study period, incidence of peripartum CDI increased 3.4 fold [95% confidence interval (CI) 1.5–7.4, p = 0.005]. Prior to 2007, there was no significant increase in CDI over time [incidence rate ratio (IRR) = 1.00, 95% CI: 0.84–1.18, p = 0.97]; post-2007, there was an increase of 7% a year (IRR = 1.07, 95% CI 1.00–1.16, p = 0.05), which contributed to the overall trend (Table 2, Figure 1). There was no statistically significant increase in incidence when CDI during pregnancy and postpartum were analyzed separately (Table 2), likely due to smaller sample size.
Trends in incidence of peripartum CDI from 1997 to 2017 a .

Data shown as IRR per year.
p < 0.0; **p < 0.10.
CDI, Clostridioides difficile infection; CI, confidence interval; IRR, incidence rate ratios.
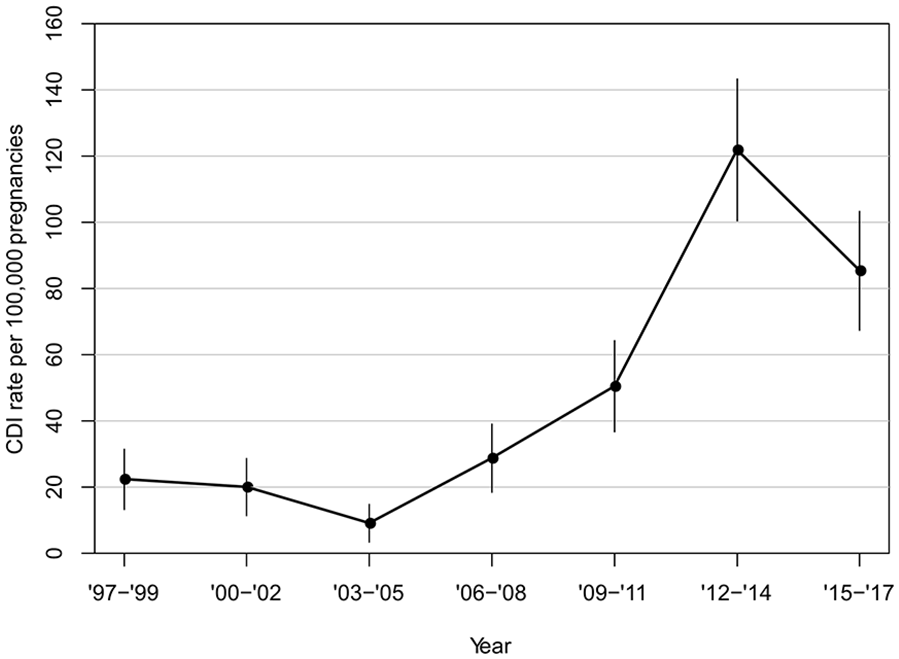
Incidence of peripartum CDI from 1997 to 2017.
Discussion
In this large single-center retrospective cohort study, we demonstrate increasing incidence of CDI in peripartum women over a 21 year period from 1997 to 2017. Majority of the CDI cases were HA, though a large proportion was CA. Health-care exposure and exposure to systemic antibiotics were the most common risk factors.
The increasing CDI incidence in our population is similar to that reported previously in the general population in the US, and higher than previously reported in peripartum women.1,6,7,9 Two studies using the Nationwide Inpatient Sample database reported a two-fold increase in peripartum CDI during the study period (1998–2006 in the study by Kuntz et al., and 1999–2013 in the study by Ruiter-Ligeti et al.).6,7 Both studies included only patients hospitalized for delivery who develop CDI, thus excluding outpatients and any CDI that may have occurred earlier in pregnancy or later in the postpartum period. In contrast, we included data from both inpatients and outpatients, and CDI occurring any time during pregnancy and in the postpartum period.
One factor to consider while interpreting results from our study is the change in C. difficile diagnostic modality from EIA to PCR during the study period. Change in testing methodology would lead to a rise in incidence in the immediate period following the change, which would plateau thereafter. In our study, the increase in incidence was seen only after 2007 (when testing methodology changed); however, the consistent rise in incidence seen for several years post-2007 indicates a real increase in incidence and cannot be explained by change in testing strategy alone.
We found the most common risk factor for CDI in peripartum women to be healthcare exposure, followed by systemic antibiotics. Since maternal antibiotic exposure has been associated with childhood asthma and peripartum CDI can be associated with morbidity, judicious use of antibiotics is important. 10 Antibiotic exposure was similar in patients with vaginal and cesarean delivery (within the subset of patients with postpartum CDI), though we did not specifically collect information on antibiotic exposure in the immediate peri-partum period. Healthcare exposure is common in peripartum women due to the need for close monitoring. Results from our study highlight the need for further research into whether peripartum women with CDI have more frequent healthcare contact than their non-CDI counterparts, which would have important implications for clinical practice. Interestingly, though deliveries are often associated with traditional CDI risk factors (hospital admission, antibiotic use, surgery), we found that most women had CDI earlier during the pregnancy. Several reasons could account for this: first, most studies to date have focused on pregnant women hospitalized for delivery; thus, information on CDI and CDI-related risk factors earlier in pregnancy or in the postpartum period are largely unknown. Second, antibiotic use, the strongest risk factor for CDI, is highly prevalent in pregnancy. Approximately one in four pregnant women receives antibiotics, accounting for 80% of all prescriptions during pregnancy. 11 Third, pregnant women have frequent healthcare contact for antenatal care or complications from pregnancy, which may place them at risk for CDI. Lastly, CA CDI (1/3rd of our cases) is often not associated with traditional risk factors for CDI, suggesting that other factors may drive the community transmission of the infection. 12
Our study is one of the few reporting data on the incidence of CDI in peripartum women. Strengths of the study are inclusion of cases throughout pregnancy and regardless of hospitalization status, thus enabling assessment of both HA and CA CDI. Our study also provides the most updated data on incidence, with data up to 2017. Confirmation of eligibility of cases via manual chart review also strengthens our results. Limitations of our study include referral bias and diagnostic detection bias due to a change to PCR in 2007, which could partly explain a shift in incidence but not account for the increase seen thereafter. Other limitations are the inclusion of modest number of cases from a single center, which may not be representative of the broader US population.
To conclude, the incidence of peripartum CDI is rising. Increased awareness and surveillance efforts for CDI are warranted in this highly vulnerable population. Pregnant women presenting with diarrhea with risk factors should be tested for CDI.
Footnotes
Acknowledgements
We thank Kristin Mara, Biostatistician for her help with performing statistics and data analyses. Part of this study was presented at Digestive Disease Week (DDW) held at San Diego from 18–21 May 2019.
Author contributions
SS: design of study, data abstraction, statistical analysis, interpretation of data, manuscript writing. RP: data abstraction, manuscript writing. RNT: interpretation of data, intellectual input in drafting the article, approval of manuscript. DSP: interpretation of data, intellectual input in drafting the article, approval of manuscript. SK: design of study, data abstraction, interpretation of data, drafting, revising and approving the manuscript. All authors have approved the final draft of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.