
Abstract
Background and aims:
The role of small bowel neoplasia (SBN) screening in asymptomatic patients with Lynch syndrome (LS) is uncertain. The aim of our study was to assess the effectiveness of screening by capsule endoscopy (CE) in these patients.
Methods:
This study was an observational, analytical, and retrospective single-center study within the PRED-IdF network. All consecutive asymptomatic patients older than 35 years-old with confirmed LS and no personal history of SBN who started the screening from 2010–2015 were included. The baseline screening and 24 months follow-up were performed by CE. The CE diagnostic yield (positive tumor or polyp) and accuracy, using the follow-up as gold standard, were evaluated.
Results:
A total of 150 patients underwent the SBN screening program and 135 (52.7 ± 11.2 years-old, 37.8% male) met the inclusion criteria. The baseline CE diagnostic yield was 4.4% (3 polyps, 3 tumors) and the proximal small bowel was the most common location (n = 4, 66.7%). In total, 87 patients underwent follow-up and the diagnostic yield was 4.6%.
Four patients were considered positive at follow-up (2 adenomas, 2 adenocarcinomas). The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of CE were 60%, 100%, 100%, 96.9%, and 97%, respectively.
Conclusions:
CE is an accurate procedure for baseline screening of SBN in LS patients and may be efficient for follow-up procedures. However, the optimal starting age of screening and intervals of follow-up must be clarified.
Introduction
Lynch syndrome (LS), also known as the hereditary non-polyposis colorectal cancer, is an autosomal dominant inherited disorder caused by a pathogenic variant in one of the mismatch repair genes (path_MMR), mostly path_MLH1, path_MSH2 and path_MSH6. This disease is characterized by a very high risk of early-onset colorectal and endometrial cancer and an increased risk of other neoplasms, including cancers of the stomach, ovary, urinary tract, and small bowel.1,2 Recently, several studies have evaluated the life-time risk of small bowel neoplasia (SBN) in LS patients, which is estimated to be around 4–5%.3,4 Although the SBN risk increases with age, LS patients may develop early adenocarcinoma usually located in the duodenum and jejunum.5,6
Currently, SBN screening by capsule endoscopy (CE) or radiological examinations in LS is not recommended, 7 however, prospective studies in the literature analyzing the usefulness of CE in these patients are lacking. Indeed, CE8,9 and magnetic resonance enteroclysis (MRE) 10 have shown to have a high diagnostic yield in the diagnosis of sporadic small bowel (SB) tumors. Similarly, the diagnostic yield of CE in LS has been assessed in two prospective studies with different outcomes. Saurin et al. 11 described an 8.6% SBN rate in 35 asymptomatic patients with LS who underwent CE, thus concluding that this technique could be better than Computed Tomography enteroclysis. Conversely, Haanstra et al. 6 reported a 1.5% SBN rate (200 asymptomatic patients), and all the lesions were located in the duodenum and within reach of conventional gastroduodenoscopy. In a follow-up study, the same group reported an SBN rate of 0% (155 patients) at 2 years, thus suggesting that small bowel screening by CE should not be warranted in asymptomatic LS patients. 12 In addition, the optimal interval time of surveillance after a baseline screening CE and the usefulness of this technique in the long term are uncertain. In this study, we aimed to evaluate, within our dedicated tertiary care center, the effectiveness of a dedicated SBN screening program by CE in asymptomatic patients with LS.
Patients and methods
Patients
This is an observational, analytical, and retrospective study performed in one center of the PRED-IdF network. All consecutive asymptomatic patients older than 35 years-old with genetically confirmed LS followed at our center were sent for SBN screening between January 2010 and December 2015. Baseline and demographic characteristics including family history of SBN and path_MMR were collected. Patients with suspected SB or obscure gastrointestinal bleeding, suspected intestinal obstruction, previous diagnosis of SB tumor, or previous SB surgery were excluded.
The SBN screening program
The PRED-IdF network is a French dedicated regional network for counselling and follow-up of patients with genetic predispositions to gastrointestinal cancers, coordinated by the Georges Pompidou European Hospital.
The baseline SBN screening was performed by CE (Pillcam SB2, Pillcam SB3, Medtronic Inc, Dublin, Ireland) in all cases. A 1.5L polyethylene glycol preparation was given the night before CE. The patients had fasted for 8 h and were allowed to drink water 2 h after the CE ingestion. Laxatives and prokinetic agents were not used. A positive diagnostic yield was retained in patients with SB polyps or tumors, while those presenting with other SB lesions (vascular lesions, ulcers, diverticula) or a normal examination were considered a negative result. CE-related adverse events were noted. All procedures were read by expert endoscopists (ES, GR) with a background of more than 2000 CE procedures.
Follow-up
According to the PRED-IdF guidelines, patients were offered either CE or MRE follow-up procedures within 12–24 months in case of normal baseline findings and every 2 years thereafter. The choice between both modalities was made in accordance with patient preference. To ensure the homogeneity in the follow-up of our population, we only considered the first CE follow-up procedure.
In case of suspected SBN, double balloon enteroscopy (DBE) (Fujifilm Inc., Saitama, Japan) was performed under general anesthesia to obtain histological confirmation. Subsequently, endoscopic or surgical removal of the neoplastic lesions was decided based on patient and lesion characteristics.
Ethics
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. Written informed consent was obtained from all patients entering the PRED-IdF network, for both prospective and retrospective data analysis. The research proposal was reviewed and approved 7 September 2019 by the local ethics committee, the CERAPHP.5 (registration number of the committee: 00011928).
Statistical analysis
Categorical variables were compared using the χ2 test or Fisher’s test. Normally distributed continuous variables were presented as the mean standard deviation and analyzed by Student’s t-test. Non-normally distributed variables were expressed with the median and the range, and were analyzed by the Mann–Whitney U test. Preliminary sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for CE baseline diagnosis. Per-patient and per-procedure approaches were also considered. The gold standard for SBN screening was a composite criterion. A positive screening was retained when a histopathological confirmation of adenoma or adenocarcinoma, or the presence of an SBN (polyp or tumor) were achieved in follow-up examinations during a maximum period of 24 months following baseline CE. A negative result was retained in patients with a minimum of 12 months uneventful follow-up after baseline CE procedure. Per-procedure CE analysis was also carried out. p-values < 0.05 were considered statistically significant. SPSS version 24 was used (IBM, SPSS Inc., IL, USA).
Results
Patients
A total of 150 patients underwent the SBN screening program. Out of those, 15 were excluded as follows: obscure gastrointestinal bleeding (n = 8), SB obstruction (n = 3), and previous SB surgery (n = 4). Finally, 135 (52.7 ± 11.2 years-old, 37.8% male) patients were included in the data analysis. The LS pathogenic variants were path_MSH2 (n = 59, 43.7%), path_MLH1 (n = 52, 38.5%), path_MSH6 (n = 20, 14.8%), path_PMS2 (n = 3, 2.2%), and path_EPCAM (n = 1, 0.7%). There was a personal history of colorectal cancer in 30.4% of cases and a family history of SB cancer (SBC) in 25 patients (18.5%).
CE diagnostic yield
CE reached the caecum in 132 cases (97.8%) and the SB preparation was considered adequate in all but one procedure (99.3%). The diagnostic yield was 4.4% because of the presence of tumors (n = 3) or polyps (n = 3) located in the jejunum (n = 3, 50 %), ileum (n = 2, 33.3%), and duodenum (n = 1, 16.7%). Characteristics of patients with a positive CE for screening are shown in Table 1. There was a difference in the median age of patients presenting with an SB tumor (71.4 years, range: 61.5–74.4), compared with those with no tumor detected by CE (52.2 years, range: 30.9–82.2), and this difference was statistically significant (p = 0.021). No patient with a positive-CE had a family history of SBN and there was no statistically significant association between the path_MMR and the diagnostic yield (p = 0.99). All patients with an SB tumor (Figure 1) underwent surgery, and endoscopic resection by DBE was performed in those presenting with polyps. The capsule also detected angioectasias (n = 15, 11.1%), erosions (n = 3, 2.2%), caecal polyp, (n = 1, 0.7%) and colorectal cancer (n = 1, 0.7%), but all these results were considered as a negative-CE. There were no procedure-related adverse events.
Characteristics of patients presenting with Lynch syndrome and a positive capsule endoscopy for baseline screening of small bowel neoplasms.
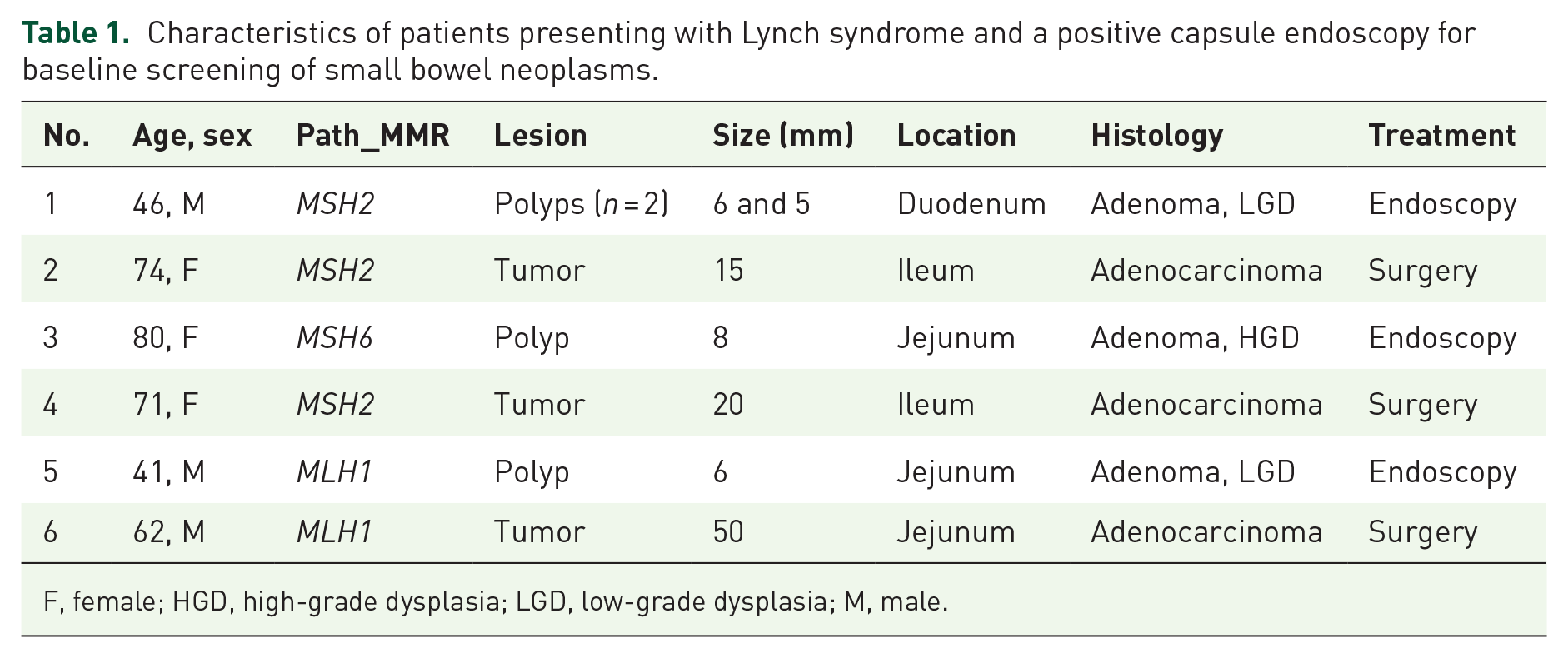
F, female; HGD, high-grade dysplasia; LGD, low-grade dysplasia; M, male.

Capsule endoscopy findings in two asymptomatic path_MMR carriers. (A) identification of a low-grade dysplasia adenoma of the jejunum, and (B, C) of a T2N0M0 ulcerated tumor of the ileum.
Considering a per-procedure approach, a total number of 87 follow-up CEs were performed (64.4%). They were considered positive in four cases. After exclusion of the 48 patients in whom the follow-up CE was not performed, the overall diagnostic yield was 4.5%.
Follow-up and CE accuracy
A total of 87 patients underwent follow-up CE. The mean interval between baseline and follow-up procedures was 24 (11–34) months. Four patients were considered positive at follow-up due to the presence of a tumor (n = 2) or polyp (n = 2), as described in Table 2. All of them presented with a negative baseline CE and a positive follow-up CE. Notably, these SBN were located in the duodenum (n = 2), ileum (n = 1), and jejunum (n = 1). Surgical or endoscopic therapy was carried out in all cases and a histopathological confirmation of adenoma or adenocarcinoma was made.
Characteristics of patients with Lynch syndrome presenting with a negative baseline and a positive follow-up capsule endoscopy.

F, female; LGD, low-grade dysplasia; M, male.
Predictive values of baseline CE
After follow-up analysis, the baselines sensitivity, specificity, PPV, NPV, and accuracy of CE for SBN screening (Table 3) were 60%%, 100%, 100%, 96.9%, and 97%, respectively. Notably, there were four false negative-CE as previously described. The sensitivity, specificity, PPV, NPV, and accuracy for SBC (excluding adenomas) were 60%, 100%, 100%, 98.5%, and 98.5%, respectively.
Diagnostic accuracy values of baseline CE for screening of small bowel neoplasms in patients with Lynch syndrome.

A positive screening was retained when a histopathological confirmation of adenoma or adenocarcinoma, or the presence of an SB neoplasm, in follow-up examinations was achieved.
CE, capsule endoscopy.
Discussion
In the present study, we report the effectiveness of a dedicated screening program by CE in patients with LS. This technique achieved a baseline diagnostic yield of 4.4% in 135 asymptomatic patients with different pathogenic variants. In addition, using a composite gold standard that includes histology and follow-up by CE, we described a 96.9% accuracy for detecting tumors or polyps. Of note, the baseline and follow-up diagnostic yields were comparable, which implies that a short follow-up should be encouraged in these patients.
Presently, SBN screening in LS is offered to patients presenting with symptoms suggesting an SB disease, similarly to the general population. A Korean multicenter study 13 described that CE can effectively identify sporadic SB tumors undetectable by conventional radiological examinations, achieving a diagnostic effectiveness of 52.6%. This technique has also modified the therapeutic course in 12.3% of cases. Similarly, DBE has been reported as an accurate technique with a good concordance with CE 14 and has an effect on the clinical course of these patients. 15 There are few reports on patients with inherited polyposis syndromes. Caspari et al. 16 concluded that there is no significant difference between MRE and CE for the detection of large (i.e. more than 15 mm), clinically significant polyps in these selected cases. Recently, both the European Society for Paediatric Gastroenterology Hepatology and Nutrition and the European Society of Gastrointestinal Endoscopy (ESGE) recommend the gastrointestinal surveillance by upper-gastrointestinal (GI) endoscopy, colonoscopy, and CE in Peutz–Jeghers syndrome.17,18
In our study, we analyzed the diagnostic yield of CE in asymptomatic patients with LS under a dedicated screening program. The CE achieved baseline diagnostic yields of 4.4% for SBN and 2.2% for SBC, which were similar to those previously reported (1.5–8.6%).6,11 We reported four false negatives. Among them, two presented with a duodenal SBN and two with a jejunal tumor during the follow-up. Of the two patients with SB adenocarcinoma, we report a 63 years-old female with poor SB cleanness at baseline and a positive CE at 1 year, and a 48 years-old female with a positive CE at 24 months from baseline CE. Both patients had a normal upper-GI endoscopy before baseline screening. Technical issues such as a faster transit and limited bowel distension may explain the proximal cases of false negative. In the same setting, Haanstra et al. 6 reported a false negative in a patient diagnosed with duodenal cancer 7 months after a negative CE. However, definition of a false negative in LS is complex and has to be balanced with the syndrome’s specificities. First, Edelstein et al. 19 have reported in colorectal lesions a faster adenoma to carcinoma sequence compared with sporadic adenomas. 19 Second, Kloor et al. 20 reported development of colorectal cancer from normal mucosa without a polyp precursor, probably arising from MMR deficient crypt foci. To our knowledge, these valuable data are not available for SB but may contribute to the development of a “false negative.”
In our series, baseline localizations of the SBN were as follows: duodenum 16.7% (1), jejunum 50% (3), and ileum 33.3% (2). Notably, the lesions were diagnosed equally between men and women (0.5 sex ratio). We reported only one patient with a duodenal neoplasia, and most of the adenocarcinomas (66.6%) were located in the ileum. Our reports emphasizes the results of previous and recent studies. Indeed, most of SBN are usually diagnosed in males with a majority of proximal lesions located in the duodenum and jejunum.21–23 In the recent Dutch consortium study (200 LS patients), the baseline SBC diagnostic yield was 1%. 6 Characteristics of adenocarcinomas were consistent with the literature, both developing in males and located in the duodenum. More recently, Hammoudi et al. 24 reported the prevalence of duodenal lesions by upper-GI endoscopy performed every 3–4 years. Among the 154 patients included (path_MLH1 and path_MSH2), a total of 12 duodenal neoplasia were diagnosed, including 3 invasive adenocarcinomas and 1 lesion arising from the ampulla. Of note, all patients included in our study also had an upper of upper-GI endoscopy every 4 years in accordance with the PRED-IdF guidelines, and no additional duodenal lesion was detected. Of the two patients with duodenal lesion, both had a normal upper-GI endoscopy before baseline CE. According to these findings, and because of the low reported prevalence of SBN among asymptomatic patients with LS, the ESGE published guidelines in 2019 that do not recommend routine SB screening in asymptomatic patients with LS. However, these guidelines may be challenged with regards to our results.
One of the strengths of our analysis is the comparison of CE with a gold standard. Indeed, not all abnormalities detected by CE are clinically relevant, and this technique can also have false positives. Haanstra et al., 12 in a multicenter prospective study of 155 asymptomatic patients, analyzed the role of a second CE procedure 2 years after the first screening procedure. CE detected possibly significant lesions in 17 cases (11% diagnostic yield), but, interestingly, further investigations revealed no significant adenoma or cancer. In our study, all positive-CE at baseline or follow-up had a histopathological confirmation and the diagnostic yield at follow-up was 4.6%.
The present study has several limitations aside from its retrospective design. All patients followed up at our center were sent for SB screening by CE and upper-GI endoscopy according to our guidelines. First, this strategy may lead to an over screening of proximal SB lesions. Second, a cost-effective analysis of our strategy is lacking and would be of interest. Finally, even if the overall CE accuracy was high (96.9%), the sensitivity was low (60%), which is an important feature for a screening test.
Conclusion
CE is a safe and accurate procedure in the screening of SBN in asymptomatic patients with LS, allowing detection of both proximal and distal lesions. Our data suggest the use of CE as an initial workup, however the optimal starting age of screening and intervals of follow-up must be clarified in further studies.
Footnotes
Acknowledgements
We would like to thank all patients followed up in our network who kindly authorized us to use their medical data and perform this study. We also would like to thank all physicians and nurses from our department who helped us to perform this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.