
Abstract
A link between chronic inflammation and carcinogenesis has been depicted in many organ systems. Helicobacter pylori is the most prevalent bacterial pathogen, induces chronic gastritis and is associated with more than 90% of cases of gastric cancer (GC). However, the introduction of nucleotide sequencing techniques and the development of biocomputional tools have surpassed traditional culturing techniques and opened a wide field for studying the mucosal and luminal composition of the bacterial gastric microbiota beyond H. pylori. In studies applying animal models, a potential role in gastric carcinogenesis for additional bacteria besides H. pylori has been demonstrated. At different steps of gastric carcinogenesis, changes in bacterial communities occur. Whether these microbial changes are a driver of malignant disease or a consequence of the histologic progression along the precancerous cascade, is not clear at present. It is hypothesized that atrophy, as a consequence of chronic gastric inflammation, alters the gastric niche for commensals that might further urge the development of H. pylori-induced GC.
Here, we review the current state of knowledge on gastric bacteria other than H. pylori and on their synergism with H. pylori in gastric carcinogenesis.
Introduction
Helicobacter pylori colonizes the human stomach, a unique ecological niche not amenable for colonization by other bacteria. The bacterium is an obligate pathogen, induces chronic gastritis and has been recognized as ‘definite carcinogen’ by the World Health Organization since 1994. Lines of evidence for its role in the development of gastric cancer (GC) were extended and updated in 2012, 1 and H. pylori is now considered to be the most prevalent carcinogenic bacterium endangering human health.
The carcinogenic gastric cascade initiated by H. pylori is detailed in the Correa sequence of histological changes. 2 Several bacterial virulence factors, host genetic make-up and facilitating ambient, predominantly nutritional, factors concur in this uneventful process. Robust clinical trials have demonstrated the beneficial effect of GC prevention by H. pylori eradication and thus completely proved the carcinogenic role of the bacterium. The role of bacteria other than H. pylori has now moved into focus in the study of gastric diseases. The introduction of nucleotide sequencing techniques and the development of biocomputional tools have surpassed traditional culturing techniques and opened a wide field for studying the mucosal and luminal composition of the gastric microbiota. A close connection between gastric microbiota and the bacterial composition in adjacent ecological niches such as the oral cavity and the duodenum has been demonstrated in recent studies. 3 A potential role in gastric carcinogenesis for bacteria other than H. pylori has been shown in several experimental animal models. However, whether the microbial changes observed in GC are a driver of disease or a consequence of the histologic progression through the precancerous cascade, is not clear at present.
The link between H. pylori and GC development has been established using data from epidemiological, basic and translational studies (Table 1). Although GC development is without doubt a result of a complex interplay between host, bacterial and environmental factors, noncardia adenocarcinomas are attributed to H. pylori with an odds ratio (OR) of 21.0.4,5
Key epidemiological studies supporting the link between H. pylori infection and gastric carcinogenesis.
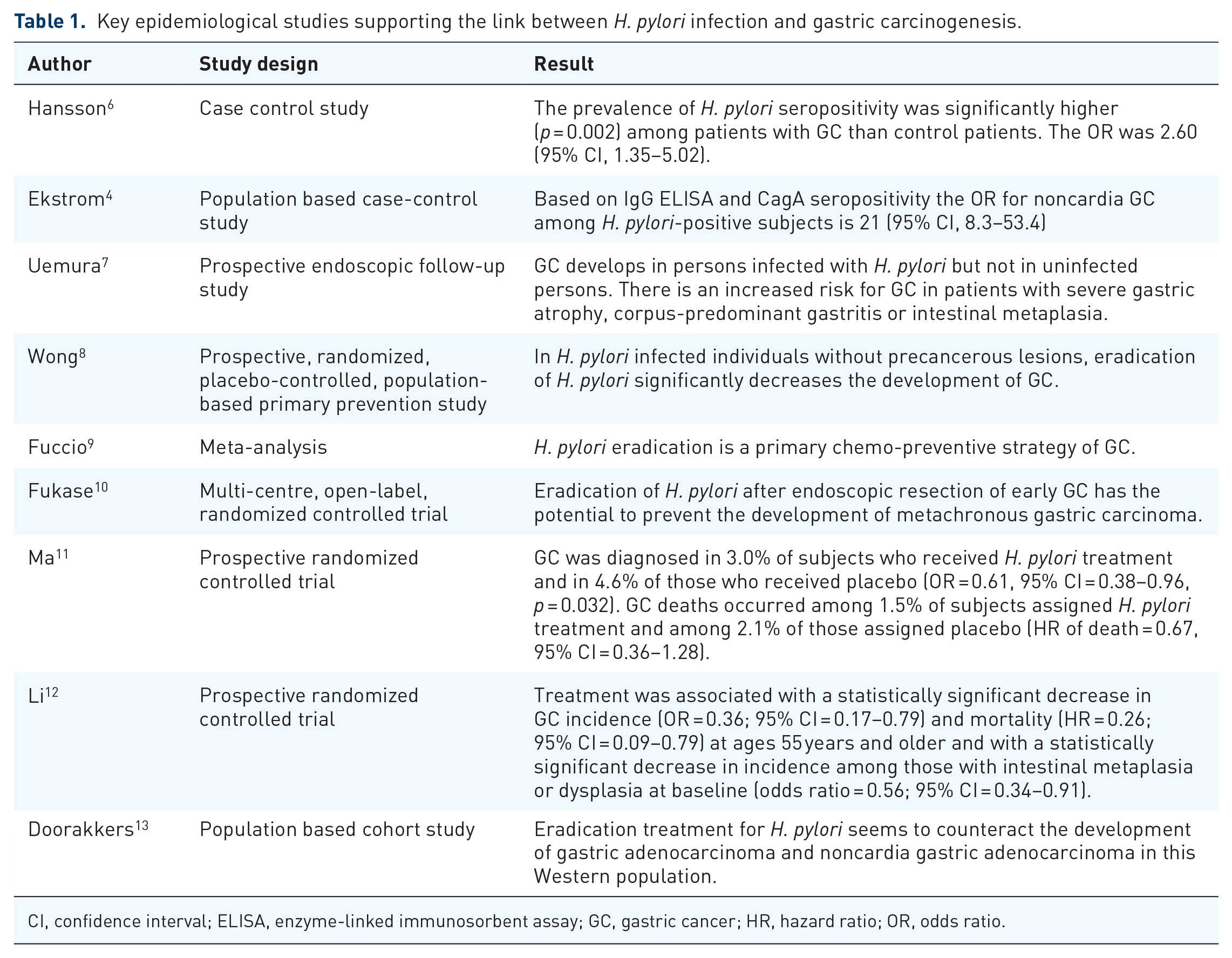
CI, confidence interval; ELISA, enzyme-linked immunosorbent assay; GC, gastric cancer; HR, hazard ratio; OR, odds ratio.
In this paper, we review the current state of knowledge on gastric bacteria other than H. pylori on the one hand, and on their synergism with H. pylori in gastric carcinogenesis on the other.
Infection-associated cancer: a global burden
Chronic infections are major risk factors triggering carcinogenesis in several organs. 26 About 15% of all diagnosed cancer cases are attributable to infections. 27 The International Agency for Research on cancer (IARC) has classified a total of 11 infectious agents as group 1 carcinogens, but only H. pylori belongs to the domain bacteria. 28 This knowledge and awareness open doors for prevention and therapy of chronic infections to decrease the incidence of infection-associated cancer. Socioeconomic conditions have a major impact on regional differences in risk patterns for infection driven carcinogenesis. While in high and very high developed regions, H. pylori is the most relevant infectious carcinogenetic agent, in low and very low developed countries, HHV8, HPV, HBV and HCV play a more dominant role in infection-associated cancers. 29
Screen-and-treat strategies to prevent GC by H. pylori eradication are cost-effective in countries with a high prevalence of GC, but may be extended to countries with an intermediate GC risk. 13,30,31
Helicobacter pylori in gastric carcinogenesis
The vast majority of noncardia adenocarcinomas is attributed to H. pylori. The risk of cardia cancer attributed to H. pylori is variable and requires stratification according to the precise topographic location. 32 The risk of cancer arising from H. pylori infection is identical for GC of both the intestinal and diffuse type.31,33,34
H. pylori was initially classified as a carcinogen based solely on large and well-performed epidemiological studies. The evidence has later been extended and strengthened by in vitro and in vivo studies.35,36 Bacterial virulence, host susceptibility genes and environmental factors such as nutritional factors are recognized to be part of a complex interplay involved in GC development. 5
Different allotypes of bacterial virulence factors such as CagA and VacA are associated with an increased GC risk. CagA is translocated into the host cell by the type IV secretion system and acts as a classic oncogene. 5 On the host side, polymorphisms and epigenetic alterations in genes encoding factors involved in the inflammatory immune response to the infection, including gene alterations in both the adaptive and the innate immune system such as interleukins (IL1β, IL8), transcription factors (CDX2, RUNX3, TLR1) and DNA repair enzymes, play a crucial role.37–40
H. pylori eradication therapy is effective in preventing GC.8,9,41–43 In intestinal type GC, carcinogenesis develops stepwise with the transition from chronic atrophic gastritis to intestinal metaplasia, dysplasia to invasive neoplasia (Correa Cascade). 2 Wether eradication of H. pylori has the potential to stop or even reverse this process and prevent carcinogenesis at any stage of this cascade or if there is a point of no return has been studied intensively (Figure 1). More recently, even in patients being treated for early GC, H. pylori eradication was shown to be still effective in a subset of patients by minimizing the risk of metachronous GC.44,45 Several studies have identified patients with severe atrophic gastritis with and without intestinal metaplasia to be at high risk of developing GC.46,47 Thus, guidelines recommend that patients with severe gastric atrophy, corpus-predominant gastritis or intestinal metaplasia should be regularly followed up by surveillance endoscopies.31,48,49

Stepwise carcinogenesis in intestinal type gastric cancer.
Later stages of the mucosal damage due to H. pylori-induced inflammation might enhance the carcinogenic effect of other risk factors such as other gastric microbiota, salt intake or tobacco smoking.
Gastric bacteria other than Helicobacter pylori and their role in gastric carcinogenesis
Despite the selective advantage of H. pylori to survive in the acidic gastric environment, other bacteria, either as resident community or as transient microbes, interact with the gastric mucosa. Studies based on culturing techniques have demonstrated bacteria other than H. pylori in conditions of hypo/achlorhydria that carry an oncogenic potential through their nitrosamine forming functions.3,33 The availability of high-throughput sequencing permits completely new insights into the gastric microbiota composition (Table 2).
Key findings from pivotal studies on other bacteria than H. pylori in gastric carcinogenesis.

AG, atrophic gastritis; ASF, Altered Schaedler’s flora; CFU, colony forming units; GC, gastric cancer; HP, Helicobacter pylori; IM, intestinal metaplasia; PPI, proton pump inhibitor; SG, superficial gastritis.
From a historical viewpoint, initial studies on this topic applied culturing methods to stomach aspirates and documented the presence of members of the phyla Firmicutes, Proteobacteria and Bacteroidetes, which are also dominating in the whole human gastrointestinal tract.34,35 However, there is a dominance of anaerobic bacteria, which are difficult to culture, in the gastrointestinal tract. Recent comparative studies applying next-generation sequencing (NGS) revealed that the active bacterial community in the gastric mucosa comprises more than 600 bacterial phylotypes and that mainly microbiota communities from the oral cavity are acquired with the use of aspirates from the stomach. The mucosa-associated gastric microbial community is dominated by Helicobacter spp. that additionally significantly impact on duodenal and oral communities. 36
Several animal studies have demonstrated a potential role in gastric carcinogenesis for additional bacteria besides H. pylori. In the absence of intestinal bacteria in germ-free, but H. pylori-infected, INS-GAS mice, a reduction in the development of preliminary carcinogenic stages such as atrophic gastritis or intestinal metaplasia was observed. Mice cocolonised with altered Schaedler flora, including ASF356 Clostridium species, ASF361 Lactobacillus murinus and ASF519 Bacteroides species or intestinal flora and H. pylori developed the most severe pathology. 37 These results led to the hypothesis that atrophy as consequence of inflammation alters the gastric niche for commensals that might further urge the development of H. pylori-induced GC.
With a clinical approach, gastric biopsies from patients living in an area of Colombia with high risk for the development of GC were compared with matched samples from a distant area with a 25-fold lower risk of GC. Sequencing analysis revealed two significantly more abundant taxa in the high-risk region (Leptotrichia wadei and Veillonella spp.) whereas Staphylococcus spp. were more abundant in the low-risk region. However, a high interindividual variability between all individuals was detected and conclusive interpretation of the findings is not yet possible. 38
A comparison of gastric microbiota in mucosal biopsies of 54 patients with gastric carcinoma and 81 patients with chronic gastritis by 16S rRNA gene profiling revealed that patients with GC had significantly decreased microbial diversity. Patients with GC presented with an overpresentation of non-Helicobacter Proteobacteria. The authors conclude that colonization with bacteria other than H. pylori, namely gut commensals, contributes to altering the equilibrium between the resident gastric microbiota and the host, and that this dysbiotic microbial community may augment the risk for H. pylori-related cancer. 39 Another study also evaluated gastric biopsies from cancer patients compared with chronic active gastritis patients. On the phylum level, no significant differences were detected, which was discussed to be a consequence of reduced acid secretion leading to reduced bacteriocidic capacity of the stomach in patients with GC or advanced stages of gastritis due to the loss of parietal cells. 40 Additionally, a quantitative PCR was used to compare the bacterial load of biopsies in more extensive groups (n = 212 chronic gastritis and n = 103 GC). A significantly increased bacterial load per gram tissue was found in the cancer group, also indicating a loss of hostile conditions in cancerous lesions.
In a 16S rRNA gene analysis of gastric mucosal samples from 81 cases including superficial gastritis (SG), atrophic gastritis, intestinal metaplasia and GC from China, which was validated in a Mongolian cohort, significant mucosa microbial dysbiosis in subjects with intestinal metaplasia and GC was observed with significant enrichment of 21 and depletion of 10 bacterial taxa in GC compared with SG [q < 0.05 after adjusting p-values for multiple comparisons by the false discovery rate (FDR) method]. Important roles for P. stomatis, D. pneumosintes, S. exigua, P. micra and S. anginosus in gastric cancer progression were suggested. 41 Another study evaluated 33 individuals including subjects with H. pylori-associated chronic gastritis, gastric intestinal metaplasia, gastric adenocarcinoma and H. pylori-negative controls. Microbiota in the stomach were analyzed by Illumina MiSeq platform targeting the 16 S rDNA from gastric biopsies. A strong negative correlation between H. pylori relative abundance and bacterial diversity was observed. In samples from patients with GC, this inverse association was weak. These samples tended to have lower bacterial diversity compared with other samples with similar H. pylori levels. After H. pylori eradication therapy, bacterial diversity increased, and the relative abundance of other bacteria to levels similar to individuals without H. pylori was restored. 50
A comparison of gastric microbiota composition between normal tissue, peritumoral and tumoral tissues in a cohort of 276 patients with GC with an approach targeting the 16S rRNA gene by MiSeq sequencing, bacterial richness was lowered in peritumoral and tumoral microhabitats. Additionally, the tumoral microhabitat presented with a simplified correlation network of abundant gastric bacteria. H. pylori (HP), Prevotella copri and Bacteroides uniformis were less prevalent, whereas Prevotella melaninogenica, Streptococcus anginosus and Propionibacterium acnes were more abundant in tumoral microhabitat. 43 The same group focused on the tumor-immune environment in relation to gastric microbiota in GC patients in a second analysis and depicted a correlation of regulatory T cells and plasmacytoid dendritic cells within the tumor microenvironment with gastric microbiota dysbiosis. 44
Nitrate-reducing bacteria are considered to aggravate gastric carcinogenesis in addition to H. pylori infection. Therefore, Jo and colleagues analyzed the bacterial composition in gastric biopsies of different sites, and divided the cohort into four subgroups (cancer ±, H. pylori ±). Using pyrosequencing of the 16S rRNA gene with special focus on nitrate-reducing bacteria, no significant differences were detected. 45 Later, one of the studies mentioned above revealed increased nitrate reductase functions promoting the reduction of nitrate to nitrite in addition to increased nitrite reductase functions promoting the reduction of nitrite to nitric oxide in gastric carcinoma microbiota in comparison to microbiota in chronic gastritis. 39
Other authors bring up the hypothesis of a potential role of biofilm formation in the development of GC, but convincing data to support this assumption is still lacking.51,52
However, the analysis of gastric microbiota with sequencing approaches is impeded by the high content of human DNA in mucosal samples, which confounds microbial identification. This can in part be overcome if whole genome sequencing approaches are applied combined with intensive human DNA filtering methods. A study using whole genome sequencing, however, revealed highly consistent results in terms of microbiome profiling of endoscopic biopsy samples with qPCR quantification of H. pylori and universal 16S bacterial quantification. 53 Furthermore, a comparison of published sequencing data on the bacterial gastric microbiome is further hampered by methodological differences in published studies with respect to the target of analysis (bacterial RNA or DNA), amplification and extraction methods. 54
Summarizing current knowledge, the hypothesis is raised that the microenvironment modification, as consequence of chronic atrophic gastritis with atrophy and reduced acidity, results in H. pylori substitution by a cancer-prone microbiota. As a consequence, it is discussed that H. pylori infection is exclusively linked to a premalignant phase of chronic gastritis, but that the tremendous shifts in gastric microbiota composition in later stages play a more relevant role in carcinogenesis itself. This might have implications for clinical management (Figure 2). 55 The complex interplay between the bacterial gastric microbiota, other players of the microbiome and the host and its immune system in gastric carcinogenesis, however, is far from being fully understood.

Hypothesis on the impact of other gastric microbiota on gastric cancer development (adopted from Schulz and colleagues). 3
Role of eradication therapy in gastric cancer prevention and interplay with gastric microbiota
Eradication of H. pylori is associated with a reduced risk of GC in Asian populations, but also in Western populations with lower incidence of the disease.11,56 Whether this is a consequence of the eradication of the carcinogen or of the alterations of the whole gastric microbiota following eradication in the short and long term, cannot be answered at this time. A study in 10 asymptomatic young adults compared the structure of the gastric microbiota before and after bismuth quadruple therapy. It demonstrated an increased alpha diversity after eradication over time with an increase in Lactobacillus and Bifidobacterium, which are assumed to act beneficially. 57 This is in line with findings from a study mentioned before revealing that H. pylori infection results in alterations of gastric microbiota and reduction in bacterial diversity, which can be restored by eradication treatment. 50
Conclusion
To date, not a single published trial provides convincing evidence for a strong involvement of bacteria other than H. pylori in human gastric carcinogenesis, albeit several studies have revealed differences in gastric microbiota composition between healthy individuals, patients with chronic gastritis and GC patients. The functional role of the changes in bacterial microbiota composition observed in advanced gastritis still needs to be elucidated. Additionally, a proportion of GC is associated with EBV infection. 58 Incorporation of the virome and mycome into the complex picture of gastric carcinogenesis is a further challenge.
Future studies not only need to differentiate between active resident and transient bacteria, to prove their mucosal adherence or intracellular localization but to also take the whole complexity of microbiota into account. Additionally, the host response to the alterations observed needs to be characterized.