
Abstract
Background:
Hepatic encephalopathy (HE) is a serious complication of cirrhosis. Decreased serum albumin (ALB) level may facilitate the development of HE and accelerate the death of cirrhotic patients with HE. Recent evidence also suggests that human albumin infusion may reduce the incidence of HE and improve the outcomes of cirrhotic patients. This study aimed to explore the association of serum ALB level with the development of overt HE and HE-associated mortality during hospitalization.
Methods:
Cirrhotic patients admitted to our hospital between January 2010 and February 2019 were screened. Independent predictors for HE were identified by logistic regression analyses. Odds ratio (OR) with 95% confidence interval (95% CI) was calculated. Area under curve (AUC) was calculated by receiver operator characteristic curve analyses.
Results:
Of the 2376 included patients with cirrhosis but without HE at admission, 113 (4.8%) developed overt HE during hospitalizations. ALB level (OR = 0.878, 95% CI = 0.834–0.924) was an independent risk factor for development of overt HE. AUC of ALB level for predicting the development of overt HE was 0.770 (95% CI = 0.752–0.787, p < 0.0001), and the best cut-off value was ⩽31.6 g/l. Of the 183 included patients with cirrhosis and overt HE at admission, 20 (10.9%) died during hospitalizations. ALB level (OR = 0.864, 95% CI = 0.771–0.967) was an independent risk factor for death from overt HE. The AUC of ALB level for predicting death from overt HE was 0.737 (95% CI = 0.667–0.799, p = 0.0001), and the best cut-off value was ⩽22.8 g/l.
Conclusions:
Decreased serum ALB level may be associated with higher risk of overt HE and HE-associated mortality during hospitalizations in cirrhosis.
Introduction
Hepatic encephalopathy (HE) is a common and serious complication of end-stage liver disease. 1 It is divided into covert and overt HE according to the clinical manifestations and severity of HE. The incidence of overt and covert HE during the clinical course of liver cirrhosis is 30–40% and 20–80%, respectively. 1 The risk of death in liver cirrhosis is greatly increased by the occurrence of HE which exerts a huge burden on patients, caregivers, and healthcare systems. 2
Except for the well-known drugs, such as lactulose, 3 rifaximin, 4 L-ornithine-L-aspartate, 5 probiotics, 6 and zinc, 7 the role of human albumin (HA) infusion for the management of HE has been widely and increasingly recognized, but remains controversial.8–10 Recently, an Italian multicenter trial (ANSWER) found that long-term HA administration to patients with decompensated cirrhosis significantly reduced the incidence of grade 3–4 HE. 11 The Italian Association for the Study of the Liver (AISF) practice guideline also suggested that HA infusion could decrease the incidence of type C overt HE in cirrhotic patients with ascites. 12 By comparison, the AASLD-EASL practice guideline did not recommend HA infusion for the management of HE. 1 The inconsistence of recommendations among these societies may be because the potential mechanism of HA infusion in the prevention and treatment HE is elusive and the current evidence is conflicting among the published clinical studies. In the study by Simón-Talero and colleagues, 8 which included patients with a mean serum albumin (ALB) level of 30 g/l, the effect of HA infusion was not significant. On the contrary, in the Sharma and coworkers’ study, 9 which included patients with a mean serum ALB level of nearly 24 g/l, the effect of HA infusion was significant. Therefore, one may speculate that the difference in patients’ serum ALB levels led to the heterogeneity in the effect of HA infusion on the development and prognosis of HE.
In the present study, we aimed to explore the association of serum ALB level with the incidence and mortality of overt HE in cirrhotic patients during hospitalization.
Methods
Study design
This study protocol was approved by the Medical Ethical Committee of the General Hospital of Northern Theater Command (formerly called as General Hospital of Shenyang Military Area), with approval no. k(2019)18 (ethical approval was obtained on 5 June 2019). The requirement of informed written consent was waived because we only extracted the data from the inpatients’ medical records. The source of our patients comprised two major parts: the first part was a cohort which retrospectively enrolled the patients with liver cirrhosis, without malignancy, consecutively admitted to our hospital from January 2010 to June 2014; the second part was a cohort which prospectively enrolled the patients with liver cirrhosis, without malignancy, consecutively admitted to the Department of Gastroenterology of our hospital and underwent contrast-enhanced computed tomography and upper gastrointestinal endoscopy from December 2014 to February 2019. 13 All patients were screened for eligibility. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
As for the association of serum ALB level with development of HE during hospitalizations, the exclusion criteria were as follows: (a) patients with overt HE at admission; (b) patients who received HA infusion before diagnosis of overt HE during hospitalizations; (c) patients who were not diagnosed with overt HE but received HA infusion during hospitalization; and (d) patients in whom serum ALB level was missing.
As for the association of serum ALB level with in-hospital mortality of HE, the exclusion criteria were as follows: (a) patients without overt HE at admission; (b) patients who received HA infusion during hospitalizations; and (c) patients in whom serum ALB level was missing.
Data collection
Data were collected as follows: age, sex, etiology of liver cirrhosis, ascites, acute upper gastrointestinal bleeding (AUGIB), infection, hemoglobin (Hb), white blood cell count (WBC), platelet count (PLT), total bilirubin (TBIL), ALB, alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (AKP), gamma-glutamyl transpeptidase (GGT), blood urea nitrogen (BUN), serum creatinine (Scr), potassium (K), sodium (Na), ammonia, prothrombin time (PT), and activated partial thromboplastin time (APTT). Child–Pugh and model for end-stage liver disease (MELD) scores were calculated. 14 We recorded the overt HE events at admission or during hospitalization and re-evaluated the diagnosis of overt HE according to the current guideline. 1 In-hospital death was also recorded.
Statistical analysis
All statistical analyses were performed using the SPSS software version 20.0 (IBM Corp, Armonk, NY, USA) and MedCalc software version 11.4.2.0 (MedCalc Software, Mariakerke, Belgium). A two-tailed p < 0.05 was considered statistically significant. Logistic regression analysis was performed to identify the independent predictors associated with the development of, and in-hospital death from, overt HE. Receiver operator characteristic (ROC) curve analysis was used to explore the performance of serum ALB level for predicting the development of, and in-hospital death from, overt HE. Area under curve (AUC) was calculated. The best cut-off value with its sensitivity and specificity was also identified. Then, we divided the patients into high- and low-serum-ALB-level groups according to the best cut-off value. Difference between high- and low-serum-ALB-level groups was compared by the nonparametric Mann–Whitney U test and the Chi-square test. The cumulative rates of overt HE and its associated mortality during hospitalization were further assessed with the Kaplan–Meier curve analyses, and the difference between the groups divided according to the best cut-off value was compared by the log-rank test.
Results
Association of serum ALB level with development of overt HE during hospitalizations
A total of 2376 cirrhotic patients were included (Figure 1). Baseline characteristics were described in Table 1. Median age was 55.26 years (range: 6.20–89.19), and 1619 (68.10%) patients were male. Median serum ALB level was 34.90 g/l (range: 9.60–56.20). Median Child–Pugh and MELD scores were 6 (range: 5–13) and 5.32 (range: –9.67–38.80), respectively. Among them, 113 (4.80%) patients developed overt HE during hospitalizations.
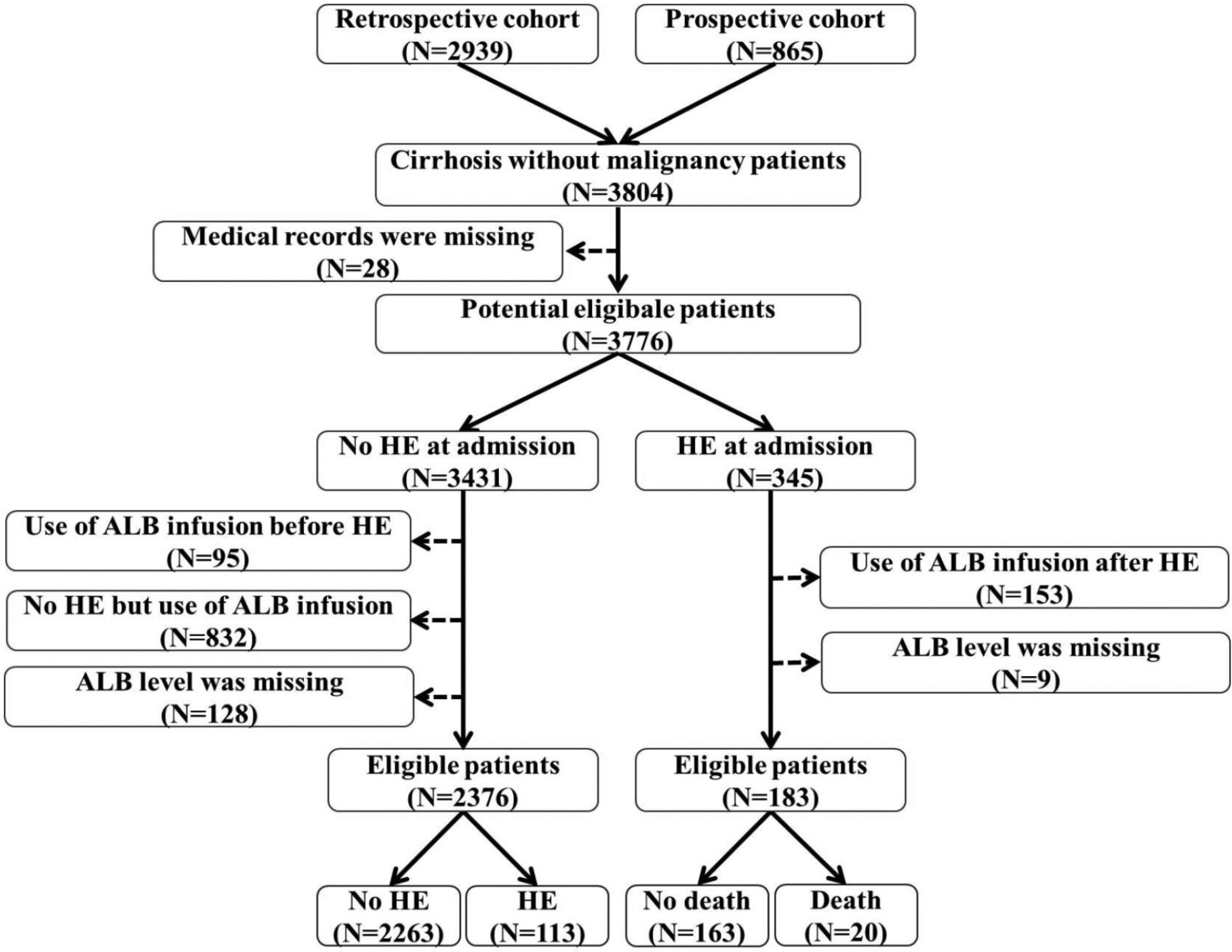
Flow chart of patient selection.
Incidence of overt HE: difference between high-ALB-level (>31.6 g/l) and low-ALB-level (⩽31.6 g/l) groups.

Bolded numerals indicate statistical significance.
AKP, alkaline phosphatase; ALB, albumin; ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; AUGIB, acute upper gastrointestinal bleeding; BUN, blood urea nitrogen; GGT, gamma-glutamyl transpeptidase; Hb, hemoglobin; HBV, hepatic B virus; HCV, hepatic C virus; HE, hepatic encephalopathy; K, potassium; MELD, model for end-stage liver disease; Na, sodium; PLT, platelet count; PT, prothrombin time; Pts, patients; Scr, serum creatinine; TBIL, total bilirubin; WBC, white blood cell count.
Note: *Continuous variables were reported as median (range) and mean ± standard deviation; categorical variables were reported as frequency (percentage).
In the univariate analysis, the statistically significant risk factors associated with the development of overt HE included age, ascites, AUGIB, infection, Hb, WBC, TBIL, ALB, AST, BUN, Scr, K, Na, ammonia, PT, APTT, Child–Pugh score, and MELD score (Table 2). In the multivariate analysis, the independent risk factors associated with the development of overt HE included age (OR = 1.028, 95% CI: 1.003–1.052, p = 0.025), infection (OR = 2.668, 95%CI: 1.481–4.807, p = 0.001), ALB (OR = 0.878, 95% CI: 0.834–0.924, p < 0.001), ammonia (OR = 1.029, 95%CI: 1.022–1.037, p < 0.001), and PT (OR = 1.098, 95% CI: 1.016–1.187, p = 0.018; Table 2).
Univariate and multivariate analyses of predictors associated with the development of overt HE.

Bolded numerals indicate statistical significance.
Child–Pugh and MELD scores, which are complex variables comprising many clinically significant variables, were excluded in the multivariate analysis.
AKP, alkaline phosphatase; ALB, albumin; ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; AUGIB, acute upper gastrointestinal bleeding; BUN, blood urea nitrogen; CI, confidence interval; DBIL, direct bilirubin; GGT, gamma-glutamyl transpeptidase; Hb, hemoglobin; HBV, hepatic B virus; HCV, hepatic C virus; HE, hepatic encephalopathy; IBIL, indirect bilirubin; INR, international normalization ratio; K, potassium; MELD, model for end-stage liver disease; Na, sodium; OR, odds ratio; PLT, platelet count; PT, prothrombin time; RBC, red blood cell count; Scr, serum creatinine; TBIL, total bilirubin; WBC, white blood cell count.
AUC of serum ALB level for predicting the development of overt HE was 0.770 (95% CI: 0.752–0.787, p < 0.0001; Figure 2). The best cut-off value was ⩽31.6 g/l with a sensitivity of 71.68% and a specificity of 70.97%. According to the cut-off value, 2376 patients were divided into high (n = 1638) and low (n = 738) serum ALB level groups (Table 1). The low-serum-ALB-level group had a significantly higher prevalence of ascites (p < 0.001), AUGIB (p < 0.001), and infection (p = 0.012) than the high-serum-ALB-level group. Hb, WBC, PLT, TBIL, ALB, AST, AKP, BUN, K, Na, ammonia, PT, APTT, Child–Pugh score, and MELD score were significantly different between high- and low-serum-ALB-level groups (p < 0.05, in all comparisons). The low-serum-ALB-level group had a significantly higher incidence of overt HE during hospitalization (11.00% versus 2.00%, p < 0.001; Table 1). Kaplan–Meier curve analysis also found that the low-serum-ALB-level group had a significantly higher cumulative rate of overt HE (p < 0.001; Figure 3).
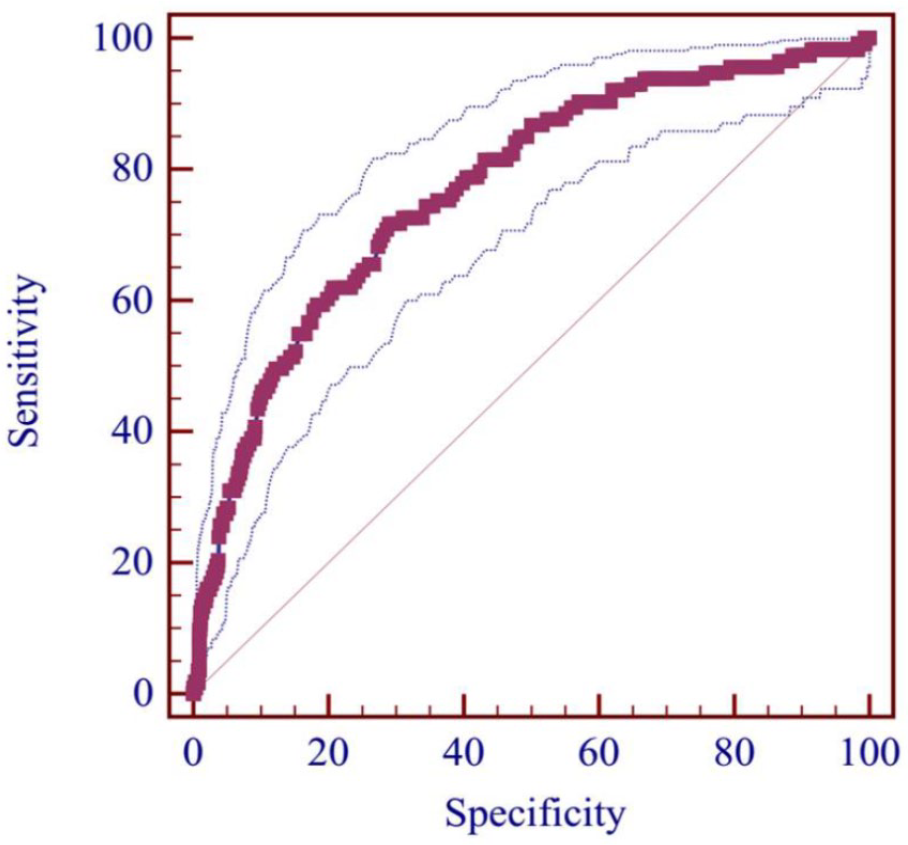
ROC curve of ALB level for predicting the development of overt HE.
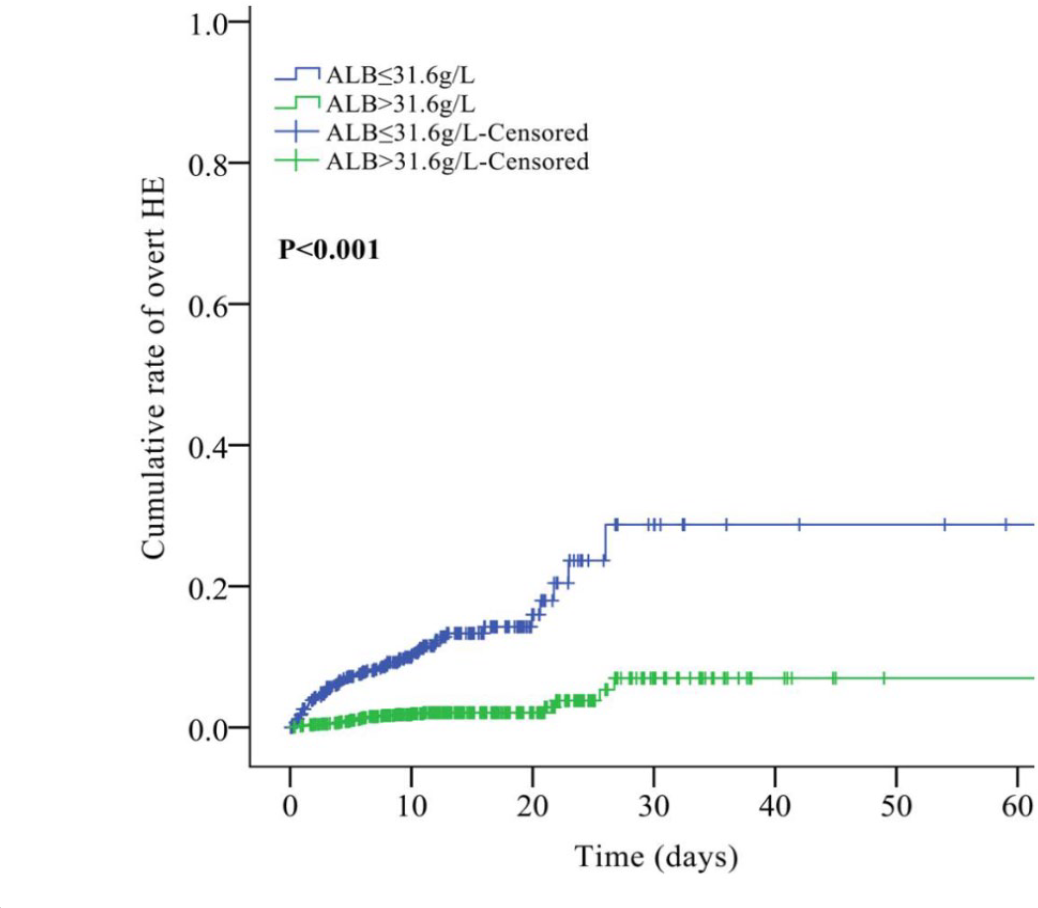
Cumulative rate of overt HE between high and low-ALB-level groups.
Association of serum ALB level with mortality of patients with overt HE during hospitalizations
A total of 183 cirrhotic patients with overt HE were included (Figure 1). Baseline characteristics are described in Table 3. Median age was 57.17 years (range: 27.49–95.13), and 134 (73.20%) patients were male. Median ALB level was 30.40 g/l (range: 12.40–48.90). Median Child–Pugh and MELD scores were 9 (range: 6–15) and 9.49 (range: –1.73–51.64), respectively. Among them, in-hospital mortality was 10.9% (20/183).
Mortality of overt HE: difference between high-ALB-level (>22.8 g/l) and low-ALB-level (⩽22.8 g/l) groups.

Bolded numerals indicate statistical significance.
AKP, alkaline phosphatase; ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; APTT, activated partial thromboplastin time; AUGIB, acute upper gastrointestinal bleeding; BUN, blood urea nitrogen; Hb, hemoglobin; HBV, hepatic B virus; HCV, hepatic C virus; K, potassium; MELD, model for end-stage liver disease; Na, sodium; PLT, platelet count; PT, prothrombin time; Pts, patients; TBIL, total bilirubin; GGT, gamma-glutamyl transpeptidase; Scr, serum creatinine; WBC, white blood cell count.
Note: *Continuous variables were reported as median (range) and mean ± standard deviation; categorical variables were reported as frequency (percentage).
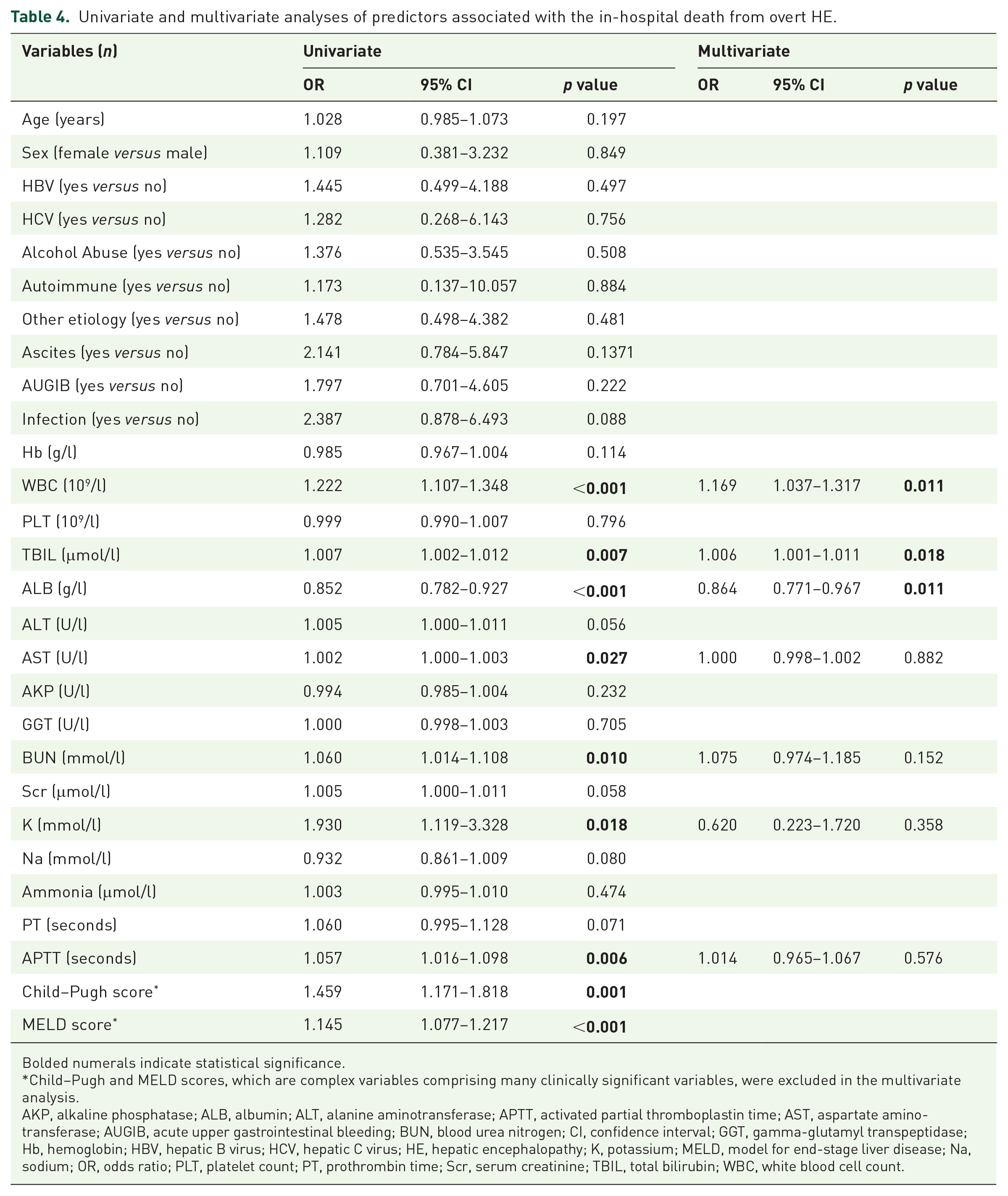
In the univariate analysis, the statistically significant risk factors associated with the in-hospital death of patients with overt HE included WBC, TBIL, ALB, AST, BUN, K, APTT, Child–Pugh score, and MELD score (Table 4). In the multivariate analysis, the independent risk factors associated with the in-hospital death of patients with overt HE included WBC (OR = 1.169, 95% CI: 1.037–1.317, p = 0.011), TBIL (OR = 1.006, 95% CI: 1.001–1.011, p = 0.018), and ALB (OR = 0.864, 95% CI: 0.771–0.967, p < 0.001; Table 4).
Univariate and multivariate analyses of predictors associated with the in-hospital death from overt HE.
Bolded numerals indicate statistical significance.
Child–Pugh and MELD scores, which are complex variables comprising many clinically significant variables, were excluded in the multivariate analysis.
AKP, alkaline phosphatase; ALB, albumin; ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; AUGIB, acute upper gastrointestinal bleeding; BUN, blood urea nitrogen; CI, confidence interval; GGT, gamma-glutamyl transpeptidase; Hb, hemoglobin; HBV, hepatic B virus; HCV, hepatic C virus; HE, hepatic encephalopathy; K, potassium; MELD, model for end-stage liver disease; Na, sodium; OR, odds ratio; PLT, platelet count; PT, prothrombin time; Scr, serum creatinine; TBIL, total bilirubin; WBC, white blood cell count.
AUC of serum ALB level for predicting the in-hospital death of patients with overt HE was 0.737 (95% CI: 0.667–0.799, p = 0.0001). The best cut-off value was ⩽22.8 g/l, with a sensitivity of 45.0% and a specificity of 93.9% (Figure 4). According to the cut-off value, 183 patients were divided into high (n = 164) and low (n = 19) serum ALB level groups (Table 3). The low-serum-ALB-level group had a significantly higher prevalence of ascites (p = 0.005) than the high-serum-ALB-level group. Hb, TBIL, ALB, AST, Scr, PT, APTT, Child–Pugh score, and MELD score were significantly different between high- and low-ALB-level groups (p < 0.05, in all comparisons). The low-serum-ALB-level group had a significantly higher mortality of overt HE during hospitalization (47.4% versus 6.7%, p < 0.001; Table 3). Kaplan–Meier curve analysis also found that the low-serum-ALB-level group had a significantly higher cumulative rate of mortality (p < 0.001; Figure 5).

ROC curve of ALB level for predicting the in-hospital death from overt HE.
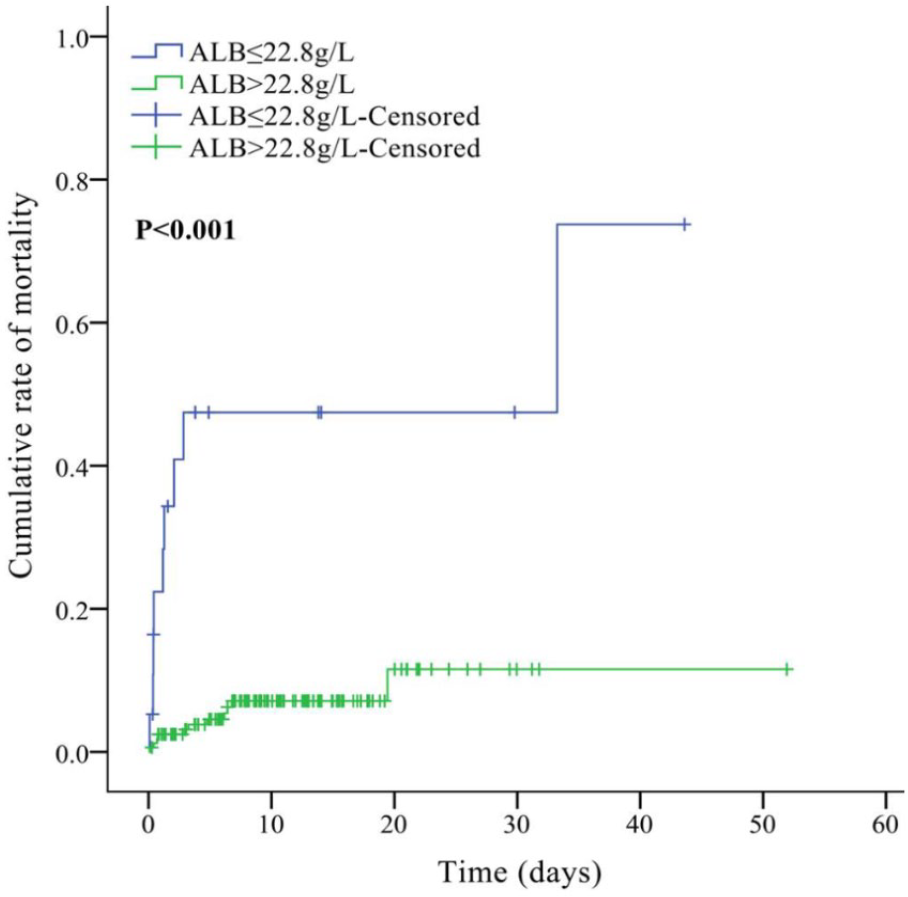
Cumulative rate of mortality between high and low-ALB-level groups.
Discussion
Our study confirmed that serum ALB level was significantly associated with the development of overt HE in liver cirrhosis during hospitalization. As compared with those with serum ALB level > 31.6 g/l, patients with serum ALB level ⩽ 31.6 g/l had a 5.5-fold increased risk of developing overt HE in cirrhotic patients. Our study also found that the serum ALB level was significantly associated with the in-hospital death of cirrhotic patients with overt HE. As compared with those with serum ALB level > 22.8 g/l, patients with serum ALB level ⩽ 22.8 g/l had a nearly 7-fold increased risk of in-hospital death in cirrhotic patients with overt HE.
Serum ALB level and development of HE
Previous studies have explored the epidemiology of HE in cirrhosis and risk factors associated with development of HE. Among the studies we reviewed (Supplementary Table 1), five studies were cross-sectional studies, four were prospective cohort studies, three were retrospective cohort studies, and one was a case-control study. Among them, eight studies explored the association of serum ALB level with development of HE, and six and two studies focused on minimal/covert HE and overt HE, respectively. All of the eight studies performed the univariate analyses and seven of them reported that serum ALB level was a statistically significant risk factor associated with development of HE; six studies performed the multivariate analyses and four of them reported that serum ALB level was an independent risk factor associated with development of HE. Similarly, our study also suggested serum ALB level was a statistically significant risk factor associated with development of HE, regardless of univariate or multivariate analyses.
Compared with previous studies, our study had particular features. First, our study had a larger number of cirrhotic patients than previous studies. Second, Child–Pugh and MELD scores, which are complex variables comprising many clinically significant variables, were excluded in our multivariate analysis. By contrast, the studies by Bhanji and colleagues, 15 Bale and colleagues, 16 and Nardelli and colleagues 17 included Child–Pugh score with or without MELD score in their multivariate analyses. This might affect the statistical results because the two scores had a potential collinearity with many variables for assessing liver dysfunction. Third, the selection of the target population was more appropriate. The patients receiving HA infusion, which would affect serum ALB level, were excluded from our study. Although serum ALB level was also an independent risk factor in the studies of Zhang and colleagues, 18 Nardelli and colleagues, 17 Tapper and colleagues, 19 and Labenz and colleagues, 20 none of them had excluded the patients receiving HA infusion. Fourth, the incidence of HE in our study was 4.8% and significantly lower than previous studies in which the incidence of HE was 20.8–45.9% (Supplementary Table 1). This could be explained by the occurrence of HE events observed during hospitalization in our study; by comparison, the occurrence of HE was observed during the long-term follow up in previous studies (length of follow up: 6 months to 5 years). Additionally, we evaluated overt HE, and did not consider minimal HE. Fifth, we performed the ROC curve analysis and identified the best cut-off value of serum ALB level for predicting the development of overt HE.
Serum ALB level and death of cirrhotic patients with HE
We also reviewed previous studies looking at mortality and risk factors associated with death of cirrhotic patients with HE (Supplementary Table 2). Among the five reviewed studies, four studies were retrospective cohort studies and one study was a prospective cohort study. The mortality of HE in the studies of Bustamante and colleagues, 21 Fichet and colleagues, 22 Cordoba and colleagues, 23 and Cui and colleagues 24 were 73.9%, 58.6%, 42.8%, and 67.7%, respectively, which was higher than that in our study (10.9%). This could be because the death event during hospitalization was observed in our study; by comparison, the death event during the long-term follow up was observed in previous studies (length of follow up: 3 months to 1 year). Notably, in the study by Jeong and colleagues, 25 where the length of follow up was 30 days, the mortality of HE was 6.7%, which was similar to that in our study. All of the five reviewed studies explored the association of serum ALB level with death from overt HE. Four studies reported the statistical results from univariate analyses and two studies showed that serum ALB level was a statistically significant risk factor associated with death from HE. Five studies reported the statistical results from multivariate analyses and one study showed that serum ALB level was an independent risk factor associated with death from HE. Notably, in the study of Cui and colleagues, 24 serum ALB level was not associated with death from HE in both univariate and multivariate analyses; this was because all patients with low serum ALB level received HA infusion.
Timing of HA infusion for preventing from development and death from HE in cirrhosis
Early studies explored the role of HA infusion in the prognosis of hospital-admission patients. In 1998, a systematic review of randomized control trials 26 showed that HA infusion might increase the mortality of critically ill patients. This conclusion had led to a significant decrease in the application of HA. 27 By contrast, in 2011, an updated systematic review did not show that HA infusion increased the risk of death. 28 Recently, more and more studies have supported the use of HA infusion in improving the prognosis of patients with cirrhosis and its complications.11,29 However, the timing of HA infusion in cirrhotic patients remained unclear.
Conventionally, hypoalbuminemia in adults is defined by a decreased serum ALB level of <35 g/l, and clinically significant hypoalbuminemia is probably identified by serum ALB level < 25 g/l. 30 Current guidelines suggested that the timing of HA infusion should be a serum ALB level of <25 g/l or <20 g/l in various types of patients.31,32 But it should be noted that HA infusion can be commenced earlier in cirrhotic patients with hypovolemia and refractory ascites; even those with a serum ALB level of >25 g/l. 31
The cut-off value of serum ALB level for predicting the risk of death was often heterogeneous among the study population, suggesting the heterogeneous timing of HA infusion in different clinical settings. In patients with major abdominal procedures or kidney cancer, serum ALB level < 32 g/l was associated with an increased risk for complications or death.33,34 In patients with hilar cholangiocarcinoma, serum ALB level < 30 g/l was significantly associated with worse outcomes. 35 In cirrhotic patients with spontaneous bacterial peritonitis, serum ALB level < 28.5 g/l was associated with worse long-term survival. 36 By comparison, our study showed that serum ALB level ⩽ 31.6 g/l might be associated with higher risk of development of HE, and serum ALB level ⩽ 22.8 g/l might be associated with higher risk of in-hospital death from HE. Therefore, we proposed the following assumptions: as for the patients without HE at admission, physicians might consider serum ALB level ⩽ 31.6 g/l as a threshold of HA infusion for prevention of overt HE; as for patients with HE at admission, physicians might consider serum ALB level ⩽ 22.8 g/l as a threshold of HA infusion for preventing the in-hospital death from HE. Certainly, these considerations should be confirmed in future cohort studies regarding albumin infusion for HE.
Limitations
Our study has some limitations. First, our study is a retrospective cohort study in which some patients’ data were missing. Second, we did not consider minimal HE. Third, we focused on the in-hospital outcomes, but not long-term outcomes. Fourth, we cannot explore the mechanism of serum ALB level in predicting the development of, and death from, overt HE.
In conclusion, a decrease of serum ALB level may play an important role in predicting the development of, and death from, overt HE during hospitalization in liver cirrhosis. A serum ALB level of ⩽31.6 g/l may be associated with higher risk for development of overt HE in cirrhosis. A serum ALB level of ⩽22.8 g/l may be associated with higher risk for death from overt HE. However, these findings should be externally validated in different populations. Whether these cut-off values can be considered as the thresholds for HA infusion for preventing the development of, and death from, overt HE in cirrhotic patients should be further explored.
Supplemental Material
Supplementary_Table_1 – Supplemental material for Association of serum albumin level with incidence and mortality of overt hepatic encephalopathy in cirrhosis during hospitalization
Supplemental material, Supplementary_Table_1 for Association of serum albumin level with incidence and mortality of overt hepatic encephalopathy in cirrhosis during hospitalization by Zhaohui Bai, Xiaozhong Guo, Frank Tacke, Yingying Li, Hongyu Li and Xingshun Qi in Therapeutic Advances in Gastroenterology
Supplemental Material
Supplementary_Table_2 – Supplemental material for Association of serum albumin level with incidence and mortality of overt hepatic encephalopathy in cirrhosis during hospitalization
Supplemental material, Supplementary_Table_2 for Association of serum albumin level with incidence and mortality of overt hepatic encephalopathy in cirrhosis during hospitalization by Zhaohui Bai, Xiaozhong Guo, Frank Tacke, Yingying Li, Hongyu Li and Xingshun Qi in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
Zhaohui Bai, Xiaozhong Guo and Frank Tacke are first co-authors.
Zhaohui Bai: reviewed and searched the literature, wrote the protocol, collected the data, performed the statistical analysis, interpreted the data, and drafted the manuscript.
Xiaozhong Guo, Frank Tacke, and Hongyu Li: discussed the findings, and gave critical comments.
Yingying Li: checked the data and performed the statistical analysis.
Xingshun Qi: conceived the work, reviewed and searched the literature, wrote the protocol, checked the data, performed the statistical analysis, interpreted the data, and revised the manuscript.
All authors have made an intellectual contribution to the manuscript and approved the submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.