
Abstract
Background:
Recurrent Clostridium difficile infection (rCDI) is becoming increasingly common. Faecal microbiota transplantation (FMT) is effective for rCDI, but the costs of an FMT and hospital cost savings related to FMT are unknown. The aim of this study was to calculate the cost of an FMT and the total hospital costs before and after FMT.
Methods:
This was an observational single-centre study, carried out in a public teaching hospital. We included all patients referred for rCDI from January 2014 through December 2015 and documented costs related to donor screening, laboratory processing, and clinical FMT application. We calculated patient-related hospital costs 1 year before FMT (pre-FMT) and 1 year after FMT (post-FMT). Sensitivity analyses were applied to assess the robustness of the results.
Results:
We included 50 consecutive adult patients who had a verified diagnosis of rCDI and were referred for FMT. The average cost of an outpatient FMT procedure if donor faeces were applied by colonoscopy was €3,326 per patient and €2,864 if donor faeces were applied using a nasojejunal tube. The total annual pre-FMT hospital costs per patient were €56,415 (95% confidence interval (CI) 41,133–71,697), and these costs dropped by 42% to €32,816 (22,618–42,014) post-FMT (p = 0.004). The main cost driver was hospital admissions. Sensitivity analyses demonstrated cost reductions in all scenarios.
Conclusions:
In a public hospital with an implemented FMT service, the average cost of FMT applied by either colonoscopy or nasojejunal tube was €3,095. Total hospital costs dropped by 42% the first year after FMT. The reduction was mainly caused by reductions in the number of hospital admissions and in length of stay.
Introduction
Clostridium difficile infection (CDI) is a major cause of nosocomial diarrhoea and constitutes 20–30% of all incidents with antibiotic-associated diarrhoea. 1 CDI incidence is increasing, and the disease poses a serious public health challenge. 2 It is associated with a high mortality rate, prolonged length of hospitalization, and risk of readmission.3–5 Risk factors for developing CDI include high age, comorbidity, and recent antibiotic use. 4 Recurrence of CDI further increases mortality rates and rates of readmission and is a major determinant of hospital costs.6,7 The recurrence rate following treatment of an initial CDI is 20–40%.8,9 In patients with multiple recurrences, the risk of another recurrence approaches 75%.10,11
The healthcare resource use and financial burden attributable to CDI are significant.3,12,13 Patients who present with CDI have longer inpatient stays, are more often admitted to an intensive care unit (ICU) and have high readmission rates. Indirect costs and productivity losses caused by illness-related disability or death from CDI must be added to the economic burden of CDI. Particular challenges apply to patients with recurrent CDI (rCDI). A micro-costing analysis carried out in the United Kingdom found that the mean annual total costs per patient for CDI and rCDI were £12,710 [95% confidence interval (CI) £9,652–15,769] and £31,121 (95% CI £19,792–42,447), respectively. 14 Most excess costs were driven by additional length of hospital stay.
Antibiotics are the first treatment of choice for CDI. Metronidazole and vancomycin are superior to placebo in CDI, and present clinical guidelines recommend vancomycin as first-line treatment for CDI.15,16 In rCDI, second-line treatments such as tapered vancomycin, fidaxomicin and adjuvant rifaximin may be used. 9 Repeated courses of antibiotic treatment may have detrimental effects on the intestinal microbiota,17,18 and therapies that ensure sustained remission and recovery of the intestinal microbiota are warranted.
Faecal microbiota transplantation (FMT) is an emerging therapeutic option for rCDI and is superior to both high-dose 10 and tapered 11 vancomycin as well as autologous FMT. 19 Resolution rates of 70–90% following FMT for rCDI have been consistently reported in both observational studies20–24 and randomized trials.10,11,19,25,26 FMT may provide sustained symptom resolution and general well-being, 27 and it may also be effective in treating complicated or severe CDI.28,29 Accordingly, clinical FMT frameworks have evolved across Europe, Australia, Asia and the USA30–36 to safely provide FMT for patients with rCDI. The costs related to operating these clinical services and their derived cost savings are unknown. A number of health economic evaluations have been published, all indicating that FMT is cost-effective.37–39 All these studies were model-based incremental analyses where only relevant costs, that is, costs that differ between the alternatives, were included. They did not provide an accurate measure of the total mean cost of FMT. Most studies were carried out in countries with a fully or partly privately funded healthcare system. Furthermore, modelling studies that present evidence-based care pathways tend to underestimate real-world cost because waste and most types of adverse events are assumed to be constant. 40
Clinicians and healthcare decision-makers need ways to understand and measure their costs over the full course of treating the patient’s medical condition, with a way to increase the value to patients with similar or reduced costs. 41 Calculated costs may differ from estimated costs, and costs depend on the national and regional healthcare systems. Cost analyses based on detailed real-world data are needed to accurately guide decision-making and the dissemination of FMT.37–39,42–44
In this study, we calculated the direct cost of an FMT in a public, hospital-based, European gastroenterology centre with an established clinical FMT service that was affiliated with a public blood centre. We further calculated the one-year cost savings following treatment with FMT to a consecutive cohort of patients with rCDI.
Methods
Study design
This was an observational, cohort-based cost analysis carried out in a public Danish referral centre for gastroenterology. We included all adult patients with rCDI who were referred for FMT from 1 January 2014 to 31 December 2015. Disease recurrence was defined as recurrence of diarrhoea with positive Clostridium difficile toxin test less than 8 weeks following treatment with vancomycin or fidaxomicin and initial symptom resolution with this treatment. In Denmark, access to healthcare services is public and free of charge. Funding is tax based, and the access to treatments is decided by the National Board of Health. In this study, experimental treatments were funded by a grant donation from the Danish Regions, aiming to investigate the potential to rationalize or prevent antibiotic treatments.
To obtain an accurate measure of the FMT costs and the hospital cost savings during the complete cycle of hospital care, we applied a time-driven activity-based costing approach (TDABC). 45 TDABC is a bottom-up approach that uses process mapping to identify all types of costs and all personnel used in the complete cycle of care. The method is suggested for healthcare research as a cost approach that provides more accurate estimates of healthcare costs than traditional full-cost allocation methods. The cost analysis involves the following distinct phases: (1) process mapping, (2) identification of types of resources, (3) measuring the amount of resources used, (4) valuation of individual resource items, (5) estimation of total and average costs per patient and (6) sensitivity analyses.41,45–47
Calculation of FMT cost
The economic perspective used for estimating costs of FMT was that of a publicly funded hospital, including the blood bank collection centre. In Denmark, donors are voluntary and unpaid local citizens, and donors’ private cost of transport and time was not reimbursed and, thus, not included. The clinical FMT framework within this study is described elsewhere. 34 In brief, the clinical framework is separated into three main activities that map all aspects related to FMT: (1) donor recruitment and screening, (2) laboratory processing and (3) clinical application (Figure 1). Cost calculations were performed separately for the three main activities. All costs were adjusted to the price level in year 2015.
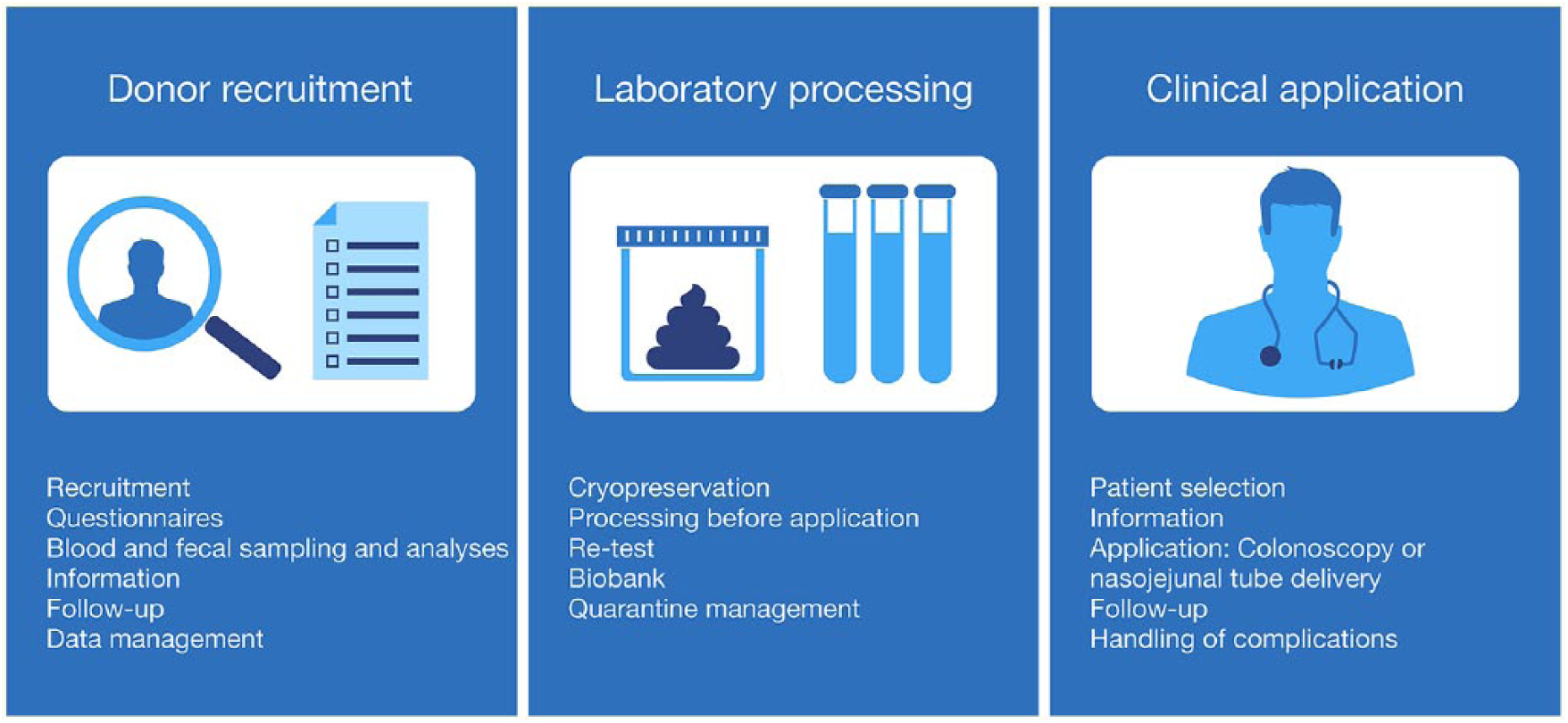
Clinical application framework for faecal microbiota transplantation (FMT), including donor recruitment and screening, laboratory processing and clinical application (adapted from Jørgensen et al. 34 ).
Cost of donor recruitment and screening
The cost calculation was based on a stepwise screening algorithm that was applied in a cohort of healthy, Danish blood donors. 48 Among 155 healthy blood donors who were asked to become faeces donors, 31 (20%) eventually passed all screening tests. Among 137 (88%) who consented to participate, 79 (58%) were excluded following completion of an electronic prescreening questionnaire. Among the remaining 58, 15 (26%) failed the blood and faecal screening, and 12 (21%) had an incomplete screening. Among the 31 blood donors who eventually qualified as faeces donors, 8 delivered donor faeces for patient treatment in the present study. Faeces donation was scheduled in donation rounds, which each consisted of faeces from five defaecations from the same donor and delivered during 1–3 weeks. At each donation, documentation of donor health and traceability of the donor faeces was documented. A negative predonation screening was valid up to 6 months before initiation of a donation round. After each donation round, all blood and faecal screening tests were repeated using repeat blood samples and the donated faeces, before release of the donor material for patient treatment.
Measurements of the personnel’s time used to conduct donor interviews, screening procedures and documentation as well as all unit costs including overhead costs for the screening procedures were provided by the Department of Biochemistry at Aarhus University Hospital (AUH), Denmark, the National Serum Institute (www.ssi.dk), Copenhagen, Denmark and the Department of Clinical Microbiology, Hvidovre Hospital, Denmark.
Cost of laboratory processing
Data for actual purchase prices of equipment excluding taxes and of disposables and wage levels (gross salaries) for all personnel groups were provided by the local accounting department (Table 1). Time measurements were provided by the Department of Hepatology and Gastroenterology and the Department of Biochemistry, AUH. The costs for laboratory processing were used to calculate the average cost per 50 g of donor faeces. Overhead costs, including facilities, equipment and other indirect costs, were estimated in cooperation with the Accounting Department, AUH.
Applied unit costs (in euros) of healthcare resources and quantity over 2 years in 50 patients treated with faecal microbiota transplantation (FMT).

Cost of clinical application
Costs of the components related to the clinical application of FMT, that is, patient assessment, diagnostic tests, antibiotics, transplantation, monitoring and follow-up were obtained from the patients’ electronic patient records (EPRs) as a quality improvement study conducted within the Department of Hepatology and Gastroenterology, AUH. Two separate cost calculations were performed, depending on whether colonoscopy or nasojejunal (NJ) tube was used for application. Costs for both procedures were calculated using reimbursement tariffs from the Danish Ambulant Grouping System (DAGS), 2015, for an outpatient visit with patient history and two follow-up contacts by telephone. DAGS rates are determined at the national level and are provided each year from the Ministry of Health. The rates cover all hospital costs except research, depreciation and capital costs. Tariffs are calculated from the principles of activity-based costing (without profit) based on publicly available accounting information from all Danish public hospitals. The cost per colonoscopically administered FMT further included a DAGS rate for an uncomplicated colonoscopy, and the cost of application by NJ tube included the DAGS rate for an uncomplicated abdominal X-ray. The price for the NJ tube (Flocare Bengmark, Nutricia, Utrecht, Netherlands) was provided by AUH and was included in the total costs for the NJ tube procedure.
Six (12%) of the patients each required 1 day of admission for preparation for the FMT procedure and monitoring. A rate for hospital admission was calculated using an average reimbursement tariff for the Department of Hepatology and Gastroen-terology, AUH. None of the included patients experienced complications following FMT. Therefore, no costs from hospital admissions for complications contributed to FMT costs. Expenses related to research and development were not included in the FMT cost calculation.
Calculation of hospital costs and savings
Patient EPRs were reviewed to document the number and length of hospital admissions, admissions to an ICU, antibiotic use, outpatient visits, emergency room visits and telephone consultations 1 year before the index FMT (pre-FMT) and 1 year following the index FMT (post-FMT). The index FMT was defined as the first FMT for each patient and separated the pre-FMT year from the post-FMT year (Figure 2).

Study design with calculation of total hospital-related costs 1 year before the first faecal microbiota transplantation (FMT) (pre-FMT) and 1 year after the first FMT (post-FMT). Cost drivers included hospital admission days, intensive care unit admission days, antibiotics use, outpatient visits, telephone consultations, and costs related to the FMT procedure. All costs related to FMT procedures were included in the post-FMT year.
Hospital costs
The applied average unit costs of hospital admission and intensive care admission were €1,108 and €4,421, respectively, using the DAGS tariff in 2014 for the Department of Hepatology and Gastroenterology, AUH. To calculate the costs of outpatient visits and telephone consultations, DAGS rates for an outpatient visit with patient history and a telephone consultation were applied. These rates were €208 and €20, respectively. The costs of contacts with the emergency room were assumed to be the same as outpatient visits. Prices for antibiotic treatments with metronidazole, vancomycin, or fidaxomicin were obtained from the Danish Medicines Agency and were €1, €27 and €213 per day, respectively (www.medicinpriser.dk). All unit costs were adjusted to the price level in 2015. All applied unit costs are listed in Table 1.
Sensitivity analyses
When data are collected and assumptions are made to estimate costs, uncertainty arises as to the accuracy of the estimates and the emphasis that can be placed on the results. The impact of this uncertainty can be assessed by undertaking a number of sensitivity analyses. In the present study, the risk of bias related to the study design and patient selection is of particular interest. As a supplement to confidence intervals for costs and statistical testing, we therefore conducted a number of scenario analyses. This is a particular form of multi-way sensitivity analysis where the expected outcomes are estimated under an alternative, but realistic set of assumptions. In each sensitivity analysis, absolute and relative differences between the base case and the specific scenario were calculated. All costs in the sensitivity analyses were calculated as average costs per patient.
First, comorbidity preceding the index CDI may have contributed to pre-FMT costs, particularly in patients who had their FMT performed less than 1 year after their index CDI. In the scenario analysis, only days of admission and days in ICU that occurred after the index CDI were included in the pre-FMT cost calculation. The post-FMT time period was truncated to the same number of days on a patient-to-patient basis.
Second, patients who died during follow-up did not contribute to post-FMT costs to the same degree as patients with complete follow-up. In the second analysis, we excluded patients who died during follow-up.
Third, a few patients with an extraordinarily high number of hospital admission days may have driven up hospital costs. We therefore excluded the 5 (10%) patients with the highest pre-FMT hospital costs in the third analysis.
Fourth, patients in intensive care may have driven up costs for both ICU treatment and overall hospital costs. In the fourth analysis, all patients with ICU admission during the study period were excluded.
Statistical analyses
All patient and cost data were documented in a central database using Research Data Capture software (REDCap, www.redcap.au.dk). Data obtained from EPRs were entered in REDCap 4.4.17 and exported and analysed using the Statistical Package for the Social Sciences (SPSS Corp., IBM Analytics, NY, USA) version 23. Mean and 95% CIs were determined for all hospital costs. In situations where cost variation could not be calculated, the uncertainty in mean costs was estimated using an expert opinion and applying a conservative estimate of ±20%. Median, interquartile range (IQR) and total range were reported for the baseline characteristics of the study population. A paired t-test was used to test for statistically significant differences between means of admission costs before and after FMT. A statistical significance level of 0.05 was applied throughout.
Ethical considerations
All procedures were performed in compliance with the standards outlined in the European Union Tissue and Cells Directives. Informed consent was obtained from all 50 patients and 8 faeces donors. Because this was a quality improvement study, the board of the Department of Hepatology and Hepatology at AUH approved the study and no formal Ethics Committee approval was required. The Danish Data Protection Agency approved data storage (j.no. 1-16-02-15-16).
Results
Patient characteristics
A total of 50 patients with rCDI were included in this study. The median age was 65 years, and 29 (58%) were female. The patients had a median Charlson comorbidity score of 3 (IQR 0.3–4.8) and a median World Health Organization (WHO) performance score of 1 (0.3–3). Eleven (22%) patients were admitted to the ICU, 13 patients (26%) suffered from inflammatory bowel disease (IBD) and 29 (58%) were being treated with proton pump inhibitor (PPI) prior to their index FMT. All baseline patient characteristics are presented in Table 2.
Patient characteristics (n = 50) at referral for faecal microbiota transplantation (FMT) for recurrent Clostridium difficile infection (rCDI).

IQR, interquartile range; WHO, World Health Organization.
Twenty-nine (58%) patients received their index FMT via colonoscopy and 21 (42%) via NJ tube. The median number of days from the index CDI to the index FMT was 259 days (IQR 80–365 days), and 12 (24%) patients suffered their first CDI more than 1 year prior to their index FMT. Four (8%) patients died during the year of follow up. No deaths were related to the FMT procedures. Two (4%) patients declined follow up before week 52. Of the remaining 44 with complete 1-year follow-up data, 40 (91%) had clinical resolution and a negative Clostridium difficile toxin test 52 weeks after the index FMT. Antibiotic treatment during follow up was provided to 29 patients, and seven patients underwent a colectomy owing to active IBD. During the follow-up period, 18 patients required an additional FMT owing to CDI recurrence; this was delivered by colonoscopy to 5 (28%) patients and by NJ tube to 13 (72%) patients.
Cost of FMT
The total cost of one FMT was calculated as the sum of average costs related to donor screening, laboratory processing, and clinical application. 34 The total calculated cost of an FMT applied by colonoscopy was €3,326 (95% CI 2,660–3,991) and €2,864 (2,291–3,437) for an FMT delivered through an NJ tube. The weighted average cost per FMT was €3,095 (2,476–3,714). Divided into each major activity of the FMT service, the costs of screening were €1,029 (823–1,235), laboratory processing €665 (532–798) and clinical application €1,632 (1,306–1,958) for colonoscopy and €1,170 (936–1,404) for an NJ tube (Table 3).
Average hospital costs for a faecal microbiota transplantation (FMT). All amounts in euros.

Hospital-related costs
The total annual costs of hospital admissions, ICU admissions, antibiotic use, outpatient visits, emergency room visits and telephone consultations per patient amounted to €56,415 (41,133–71,697) pre-FMT, and these dropped by 42% to €32,816 (22,618–42,014) post-FMT (p = 0.004). Costs for hospital admissions were the main cost driver (Figure 3). The average calculated costs of hospital admissions per patient pre-FMT were €41,286, and this dropped to €22,649 post-FMT, a cost reduction of €18,638 (45%). The cost reduction was caused by reductions in both the number of admissions and the length of stay for each hospital admission (Figure 4). The median number of days of hospital admission, excluding admissions to ICUs, dropped from 31 days pre-FMT to 8 days post-FMT (p < 0.0001). Costs of admissions to ICUs aggregated to €9,285 per patient pre-FMT and €796 post-FMT, corresponding to a cost reduction of 91% (p = 0.04). The number of outpatient visits, telephone consultations, antibiotic treatments, and visits to the emergency room remained largely unchanged (Figure 3).

Comparison of costs 1 year before (pre-FMT) and 1 year after (post-FMT) faecal microbiota transplantation (FMT) for recurrent Clostridium difficile infection (rCDI), in total (A) and subdivided into hospital cost of hospital admission (B), intensive care unit (C), outpatient visits (D), and antibiotics (E). Costs are displayed in euros as the mean per patient with 95% confidence intervals (CI) as error bars.

The number of admissions and the length of each admission dropped from the year before (left) to the year after (right) faecal microbiota transplantation (FMT) for recurrent Clostridium difficile infection (rCDI).
Sensitivity analyses
We analysed the robustness of the results using multiway scenario analyses to characterize four alternative sets of assumptions for estimating costs of FMT and potential cost savings (Table 4). The results of the scenario analyses were compared to the base case mean total hospital costs of €56,415 per patient pre-FMT and €32,816 post-FMT.
Estimates of hospital cost savings in the base case and sensitivity analysis in 50 patients who received a total of 68 faecal microbiota transplantations (FMTs) for recurrent Clostridium difficile infection (rCDI).
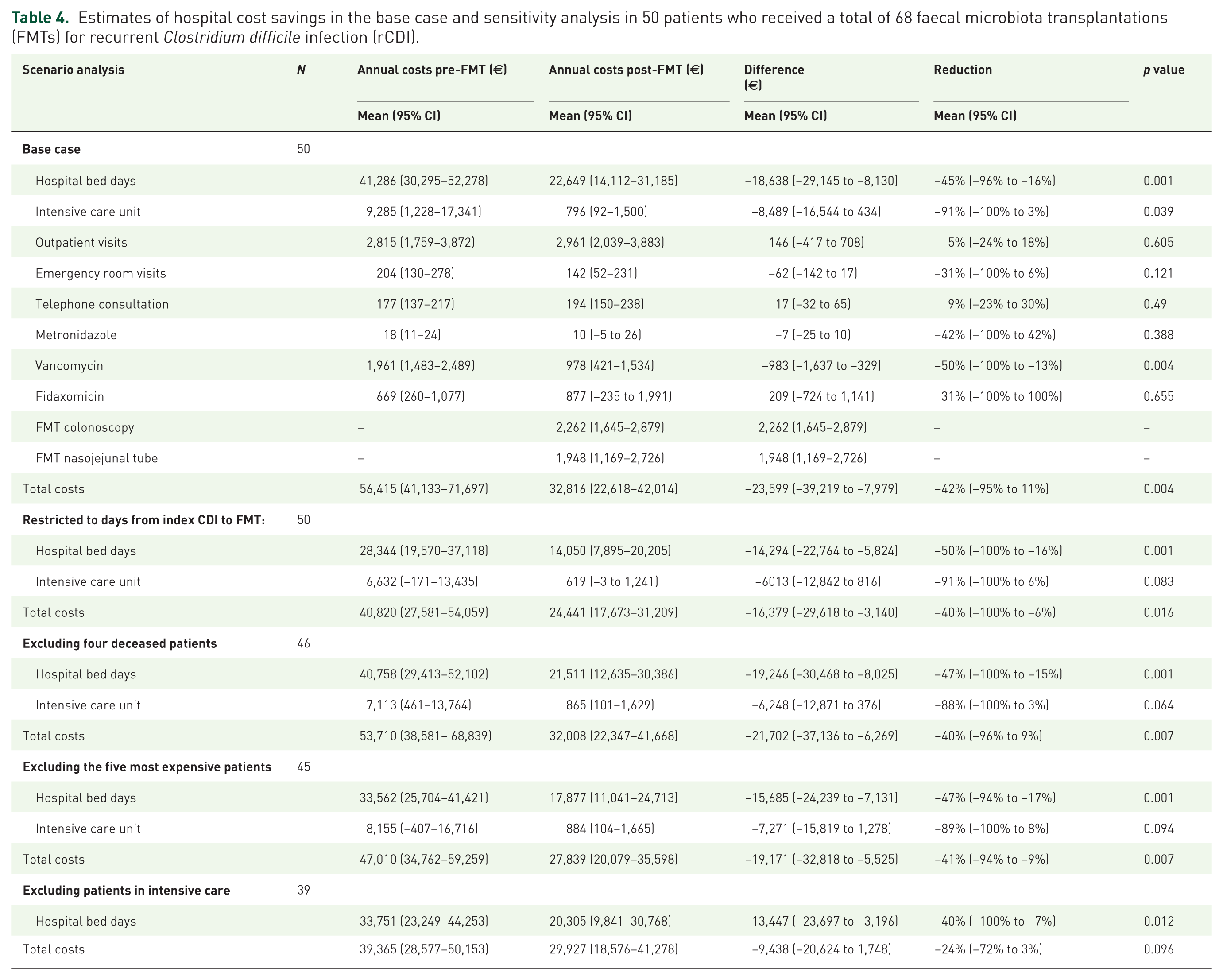
Because CDI most commonly follows antibiotic treatment, comorbidity preceding the index CDI could contribute to and in part explain the high pre-FMT hospital costs. In the first sensitivity analysis, we therefore truncated the study period to the duration from the index CDI to the index FMT in order to exclude costs related to the morbidity leading to the first CDI. Total costs per patient in this scenario were €40,820 pre-FMT, compared with €56,415 in the base case. Costs dropped by 40% to €24,441 post-FMT, documenting an unchanged relative cost reduction.
Second, four patients died during the follow-up period and did not have complete follow-up data. After analysis excluding these patients, the costs dropped from €53,710 per patient pre-FMT to €32,008 per patient post-FMT, corresponding to a 40% reduction.
Third, if the five patients who contributed most to hospital costs were removed from the study, absolute but not relative cost reductions dropped. Total costs dropped from €47,010 per patient pre-FMT to €27,839 per patient post-FMT, that is, a reduction of 41%.
Fourth, if the patients who were admitted to ICUs were excluded from the study, the costs before FMT were €39,365, and these dropped to €29,927 after FMT, that is, a 24% reduction.
Taken together, the primary findings were robust and insensitive to exclusion of outliers or patients with skewed contribution to the study data.
Discussion
This cohort study is the first to provide a direct calculation of the costs of an FMT and the derived hospital cost savings following FMT in patients with rCDI. The average net price for an FMT was €3,095. Total annual hospital costs dropped by 42% during the first year after an FMT.
No previous study calculated the costs of an FMT based on real-world data and with separation into the three major activities of a clinical framework, that is, donor recruitment and screening, laboratory processing and clinical application. Costs specifically related to screening were calculated in a recent Canadian survey where 49 volunteers were screened, only to obtain one (2%) eligible donor, with a cost of $15,190 equivalent to €13,546 in 2016. 49 In the present study, expenses for screening 40 potential donors that yielded eight eligible donors who delivered faeces for 68 FMT procedures were €69,972, or €8,746 per donor. A recent study investigated CDI subtype-guided FMT compared with vancomycin treatment and reported an FMT cost per patient of €7,614 over a 30-day period and a 10% reduction in costs compared with vancomycin, despite an isolated cost per FMT of €1,188. 50 This price for an FMT is considerably lower than the price reported in the present study. The different FMT costs may be attributable to different scenarios, one of which related to economy of scale, because Jiang and coworkers had access to a universal stool bank.
Reduction of FMT costs may be an independent aim of a clinical FMT service, and cost reductions may be achieved through multiple strategies. High donor eligibility is optimum. In our study, donor screening yielded 20% eligibility, which is high compared with 2% in Dutch 36 and 3% in Openbiome investigations. 51 The number of donations per round before recheck may be increased from five used in this study, thus reducing the screening costs per donation. However, such an increase implies a risk of discarding more faecal samples if they fail post-donation tests, and it potentially affects the eligibility if donors feel that too many donations are requested.
The main driver of the cost savings in the present study was a 45% reduction in the total days of hospital admission following FMT. The most marked cost reduction was caused by the 91% reduction in ICU admissions, which indicates that FMT may also reduce the severity of illness by curing rCDI rather than just reducing length of stay. Organizational initiatives to reduce the overall occurrence of CDI remain pivotal, including discontinuation of offending antibiotics where possible and ensuring contact precautions and hand hygiene. 52
Cost-effectiveness studies based on modelling reported high initial costs when using FMT instead of vancomycin. In this study, the high effectiveness and reduction in hospital costs more than make up for the extra costs of a single FMT. The modelling studies compared costs and effects of FMT with standard antibiotic treatments, including vancomycin, metronidazole and fidaxomicin, and indicated a potential for substantial savings and improved quality of life. The reduction in cost when treating patients with FMT was primarily a result of reduced length of stay in the hospital due to a faster recovery time.38,42,44 The present study, using real-world data, confirmed this hypothesis.
The present study demonstrated a 30% decrease in antibiotics use post-FMT. This decrease may in part be caused by the general advice to avoid antibiotics following a CDI. 16 With this in mind, the reduction is less pronounced than expected, and it is uncertain to what degree the FMT itself contributed.53,54 Patients’ fear of suffering another rCDI may have limited the decrease in antibiotic use. 55 Indeed, we found that some patients had antibiotics prescribed only as a precaution in the case of clinical recurrence. This finding contrasts with the findings of a study by Jalanka et al., which advises against the use of antibiotics as prophylaxis or in other treatable aspects immediately after FMT. 27 Future randomized studies should investigate whether FMT may facilitate reduced antibiotic use.
This study has important limitations. It was a single-centre study, carried out in an institution with an established FMT service. Generalizability to institutions without this framework is therefore not straight forward, and future studies should describe means to disseminate FMT as a clinical option for all patients, thus ensuring geographical independence. All costs were standardized to 1 year before and 1 year after FMT. This predisposes to bias because 38 patients suffered their index CDI less than 1 year prior to their index FMT, and the decrease in hospital costs following FMT may therefore be explained by other factors than the FMT itself. Many of the included patients had marked comorbidities and were admitted before their first CDI. The high difference in costs from the year preceding FMT to the year after FMT could in part be due to their comorbidities and not FMT. True cost savings are seen in patients who suffered their index CDI more than 1 year before their index FMT and by truncating the pre-FMT period to the days between the index CDI and the FMT as done in the first sensitivity analysis. Adjustment for increasing patient age during the 2-year study period was not performed and would pull the results towards the null hypothesis. Four of the patients died within 1 year after their index FMT and did not contribute to hospital costs for a whole year. Sensitivity analyses demonstrated that the costs savings were not caused by patients dying and that cost savings were equal in all patient groups. Finally, this study included only hospital costs, but a societal view would have been ideal to clarify the saving potential of curing rCDI with FMT. A cost-effectiveness study of FMT for patients with IBD found that FMT also lead to savings in societal costs, 13 and this may also be applicable to the present study.
In conclusion, the cost of an FMT was low in comparison with rCDI-associated hospital costs, which decreased by 42% the year following the index FMT, even when including costs of FMT in the analyses. Randomized controlled trials that compare FMT with state-of-the-art medical therapies would help clarify to what degree FMT is the main reason for the cost savings.
Footnotes
Author contribution
Guarantor of the article: CLH. Study concept and design: CLH, JFD, LEH. Recruitment and treatment of patients: CLH, JFD. Data collection and manuscript drafting: EDL, BKH, CWJ, MEJ, JSJ. Data analysis: EDL, BKH, SMDJ, LEH, JFD, CLH. Critical manuscript revision: EDL, BKH, SMDJ, CWJ, MEJ, JSJ, LEH, JFD, CLH. Approval of the final manuscript: All authors.
Funding
The work was supported by an independent grant from the Danish Regions Medical Funds (j.no. 14/217). The study was in part supported by Innovation Fund Denmark (grant number 8056-00006B).
Conflict of interest statement
The authors declare that there is no conflict of interest.