
Abstract
The advent of oral direct-acting antiviral agents (DAAs) has dramatically improved the hepatitis C virus (HCV) treatment landscape in the last 4 years, providing cure rates over 95% with a shorter duration of treatment and a very good safety profile. This has enabled access to treatment in nearly all HCV infected patients. The launch of two pangenotypic fixed dose combinations (FDCs) in 2017 made a new step forward in HCV treatment by slightly increasing efficacy and more importantly allowing the treatment of patients without HCV genotyping, and in some cases without fibrosis assessment. However, retreatment of the few DAA failure patients was still an issue for some HCV genotypes. The launch of the triple regimen FDC, sofosbuvir/velpatasvir/voxilaprevir, solves this issue by providing a cure rate over 96% regardless of HCV genotype. In this review, we describe the current HCV treatment landscape and focus on the development of this triple FDC either in treatment-naïve or treatment-experienced patients with previous failure on a DAA regimen.
Keywords
Introduction
Hepatitis C virus (HCV) is a hepatotropic RNA virus that causes progressive liver disease that may result in liver cirrhosis and hepatocellular carcinoma. The latest assessment from the World Health Organization suggests that roughly 71 millions people are chronically infected by HCV worldwide. 1 The major routes of contamination for this blood-born infection are unsafe drug injections and unsafe medical procedures. Sexual transmission is rare except in men who have sex with men with high-risk sexual behavior.2,3
Until 2011, treatment of chronic HCV hepatitis was based on the use of interferon, at first alone, then in combination with ribavirin (RBV) and later on as a combination of pegylated interferon plus RBV (PR) for 24 or 48 weeks. According to genotype and fibrosis stages, the sustained virological response (SVR) rate with PR varied from 40% up to 70%.4,5 Those treatments were associated with numerous side effects and a deterioration of the quality of life of patients.
Since 2011, several direct-acting antiviral agents (DAAs) have been developed which targeted three proteins involved in different key steps of the HCV life cycle: NS3/4A protease, NS5A protein and NS5B RNA-dependent RNA polymerase. The first DAAs, launched in 2011, were the two NS3/4A protease inhibitors, boceprevir and telaprevir. Combined with PR, those were able to shorten treatment duration and increase the SVR rate, 12 weeks after the completion of treatment, by 30% and up to 70–80%.6–9
Since 2013, other DAAs have been launched, targeting the three proteins. The combination of several DAAs improved the SVR rate to over 90%, with an even shorter duration of treatment at 8, 12, 16 or 24 weeks and a very good safety profile. Patients who could not be treated with PR, such as patients with ongoing intravenous use, severe renal impairments, patients with inherited blood disorders and patients with advanced cirrhosis, were finally able to be treated with those combinations.10–15
Current hepatitis C treatment landscape
Since 2013, HCV treatment is composed of oral DAA regimens only. Therapies were based on several associations: (1) combinations using sofosbuvir (SOF) the only potent nucleotide NS5B inhibitor as a backbone combined with either protease inhibitor such as simeprevir (SIM) or NS5A inhibitors such as daclatasvir (DCV) or ledipasvir (LDV); (2) a triple combination (PrOD) with a NS3/4A protease inhibitor boosted by ritonavir (paritaprevir) plus a NS5A inhibitor (ombitasvir) plus a non-nucleoside NS5B inhibitor (dasabuvir); and (3) a combination using a potent NS3/4A protease inhibitor, grazoprevir (GZR) plus a second wave NS5A inhibitor, elbasvir (EBR; Figure 1).

Treatment options with DAA combinations since 2013.
The SVR rate of phase III studies and large real-life data according to genotype and fibrosis stage are reported in Table 1. The first, all oral, DAA combination was SOF and SIM which only achieved high SVR rates in patients with genotype 1 and 4 both in clinical trials and in real-life cohorts.16–21 However, the SVR rates were slightly disappointing in patients with cirrhosis, especially in patients with genotype 1a who harbored a baseline Q80K mutation. The second combination of SOF and DCV was available soon after and was the first pangenotypic combination achieving SVR rates over 90–95% in patients infected by genotypes 1–4, across all studies, excepted in patients with genotype 3 and cirrhosis in whom the SVR rate, with or without RBV, did not achieved the 90% threshold.22–29 The third association available was the triple combination PrOD. This combination achieved a very high SVR rate over 95% in patients with genotype 1, with a lower SVR in patients with cirrhosis or subtype 1a and in those who harbored baseline resistance associated substitutions (RASs).30–37 The double combination of paritaprevir boosted by ritonavir plus ombitasvir (PrO) was also highly potent in patients with genotype 4 in clinical trials and in real-life data.37–39
SVR12 according to genotype and fibrosis stage in phase III trials and large RL studies.
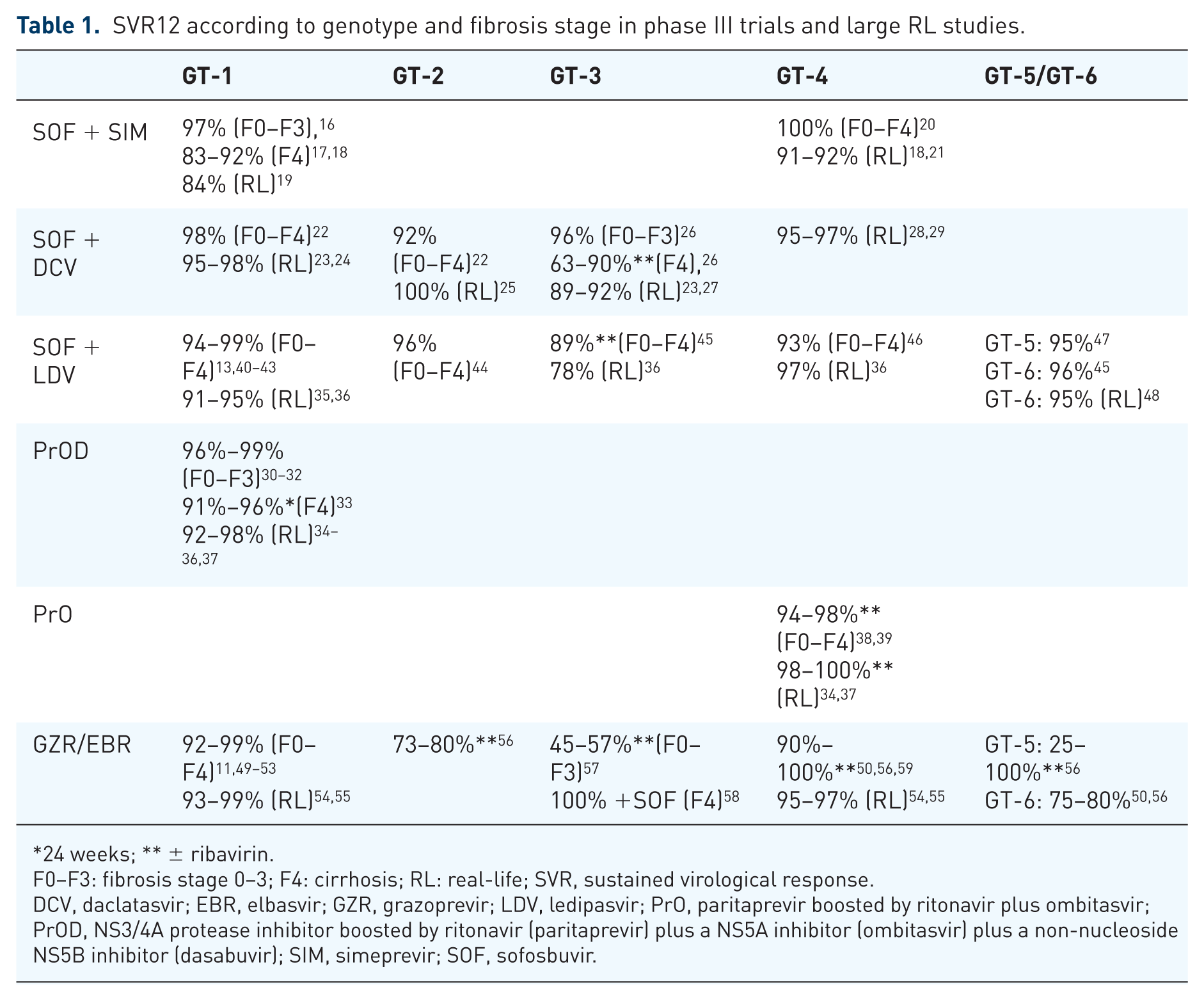
24 weeks; ** ± ribavirin.
F0–F3: fibrosis stage 0–3; F4: cirrhosis; RL: real-life; SVR, sustained virological response.
DCV, daclatasvir; EBR, elbasvir; GZR, grazoprevir; LDV, ledipasvir; PrO, paritaprevir boosted by ritonavir plus ombitasvir; PrOD, NS3/4A protease inhibitor boosted by ritonavir (paritaprevir) plus a NS5A inhibitor (ombitasvir) plus a non-nucleoside NS5B inhibitor (dasabuvir); SIM, simeprevir; SOF, sofosbuvir.
Subsequently a second wave of NS5A inhibitors became available with two new, single pill, fixed dose combinations (FDCs). The combination of SOF plus LDV was the first single pill FDC available and was highly potent in patients with genotype 1, 4, 5 and 6 at any fibrosis stage.13,40–43,45–48 This combination was the first one that demonstrated potent activity in patients with genotype 1 and 4 and decompensated cirrhosis.60,61 This combination was suboptimal for patients with genotype 3 infections. 45 For patients with genotype 2 infections, a small study demonstrated the potency of this combination in New Zealand but this result was not endorsed by European Medicines Agency (EMA) or the United States Food and Drug Administration (US FDA). 44 The FDC of GZR plus EBR was highly potent in patients with genotype 1 and 4 both in studies and in real life, even if patients with subtype 1a and baseline RASs may have needed a longer duration of treatment (16 weeks) in order to achieve the highest SVR rate.49–56,59 The GZR/EBR combination demonstrated a suboptimal SVR rate in patients with genotype 2, 3, 5 and 6.56,57 In contrast, the combination of SOF + GZR/EBR demonstrated a high efficacy rate in patients with genotype 3 and this option was, at least, endorsed by the American Association for the Study of Liver Diseases (AASLD) guidelines but not by European Association for Study of the Liver (EASL) guidelines. 58
Since 2017, two pangenotypic FDCs, SOF/velpatasvir (VEL) and glecaprevir (GLE)/pibrentasvir (PIB) were approved and launched by the US FDA and in some of the European Union countries by the EMA. SOF/VEL is the first FDC, given for 12 weeks regardless of genotype and fibrosis stage.62–65 This combination for 12 weeks with RBV achieved a very high SVR rate in patients with decompensated cirrhosis whatever the genotype. 14 GLE/PIB offers a FDC, three pills daily, for 8 weeks in naïve patients without cirrhosis regardless of the genotype and for 12 weeks in patients with cirrhosis.66–70 However, patients with genotype 3 and compensated cirrhosis need to be treated for 16 weeks. 71 GLE/PIB could not be used in patients with decompensated cirrhosis, due to the presence of NS3/4A protease inhibitors. These treatments provided over 95% of SVR in the phase II and III pivotal studies 15 (Table 2).

SOF/VEL + RBV; ** GLE/PIB for 16 weeks.
F4dc: decompensated cirrhosis; GLE, glecaprevir; PIB, pibrentasvir; RBV, ribavirin; SOF, sofosbuvir; VEL, velpatasvir.
Treatment options in case of DAA treatment failure
Despite the overall high success rate of those new DAA therapies, a small proportion of treated patients did not achieve SVR, mainly due to relapses and, rarely, to viral breakthrough under treatment. 72 Several factors may favor DAA failure to the first generation of DAAs, such as cirrhosis, virological factors, genotype 1a and 3 and RASs either pre-existing as natural polymorphisms or induced by a previous DAA regimen. A recent study using the HCV disease burden model (HEP-SIM) suggested that according to the number of patients treated with DAAs between 2014 and 2020 in five European countries (France, Germany, Italy, Spain and the United Kingdom), we can expect to have 47.000 DAA failure patients during this period and nearly all patients treated since 2015 will be NS5A-failures. 73 In the guidelines, several retreatment options according to genotype were proposed.
Patients who failed on SOF alone or SOF plus RBV or SOF plus PR can be retreated with several combinations according to the genotype. Most of the combinations may reuse SOF due to the fact that the rare NS5B RASs have a bad fitness and therefore are rarely persistent. 15
Patients, who failed the DAA regimen with SOF plus protease inhibitors without NS5A inhibitors, can be retreated with a combination of SOF with NS5A inhibitors (DCV, LDV, VEL).13,22,41,62
In patients with genotype 1 or 4 who failed DAAs regimen containing NS5A inhibitors, four options were available. The first one combined SOF with PrOD for genotype 1 or PrO for genotype 4 plus RBV either for 12 weeks in patients with mild fibrosis or for 24 weeks in patients with subtype 1a and in patients with severe fibrosis or compensated cirrhosis. 15 This option achieved an SVR rate of 95%. 74 The second option combined SOF with GZR/EBR plus RBV for 12 weeks in patients with mild fibrosis or for 24 weeks in patients with subtype 1a and in patients with severe fibrosis or compensated cirrhosis. Few data demonstrated that this combination was highly effective in achieving SVR in all patients with mild disease treated for 12 weeks and in all patients with NS5A RASs treated for 16 weeks.75,76 The third option combined SOF with DCV and SIM plus RBV for 12 weeks in patients with mild fibrosis or for 24 weeks in patients with subtype 1a and in patients with severe fibrosis or compensated cirrhosis. 76 This option was not endorsed by all real-life data.77,78 This combination in DAA failure patients, some with advanced compensated cirrhosis, demonstrated a high rate of adverse (even fatal) events, and a lower rate of response. 78 The last option is the association of GLE/PIB plus RBV for 12 or 16 weeks. The study demonstrated a high SVR rate of 96% and over in patients treated either for 12 weeks in those who harbored at baseline only a NS3 RAS or for 16 weeks in those who harbored at baseline only a NS5A RAS. For patients who have both NS3 and NS5A RASs at baseline, the SVR rate was suboptimal. 79 Therefore, this combination was not recommended in this situation, at least in the EMA label and in the last EASL guidelines. 80
In patients with genotype 2, 3, 5 and 6 who failed a DAA combination with NS5A inhibitors, the recommended retreatment option was the combination of SOF/VEL with RBV for 24 weeks. 15 This recommendation was supported by a small multicenter trial in which 69 patients with genotype 1, 2 or 3, who previously failed a NS5A containing DAAs regimen, were retreated with SOF/VEL and RBV for 24 weeks. The SVR rate was 97% in genotype 1 and 93% in genotype two patients regardless of NS5A RASs, but only 78% in patients with genotype 3. 81 Therefore there was an urgent need for a pangenotypic rescue regimen for patients who failed previous NS5A-containing DAAs regimens.
Sofosbuvir/velpatasvir/voxilaprevir single pill daily regimen
The preclinical development of SOF, VEL and voxilaprevir (VOX) has been run separately during the last decade.
US FDA and EMA have approved SOF for pangenotypic HCV treatment either in combination with PR or in an interferon-free combination either with RBV or with other DAAs. 82 SOF has a high barrier to resistance making it the ideal candidate to be used in combination with other classes of DAA and for retreatment of DAA failure patients.
VEL is a pangenotypic HCV NS5A inhibitor with antiviral activity against the HCV replicon in genotypes 1 through 6. 83 Early clinical data supported clinical development with a single dose of 100 mg once daily. 84 VEL has a higher barrier to resistance in comparison with the previous NS5A inhibitors, LDV or DCV.
VOX (or GS-9857) is a NS3/4A inhibitor with potent in vitro activity against the HCV genotype 1–6 and an improved resistance profile against the commonly encountered genotype 1 NS3 RASs in comparison with other protease inhibitors. 85
Phase II trials
The first phase II study, evaluated FDC SOF/VEL plus VOX 100 mg once daily with food in 161 patients with genotype 1 or 3 for a short treatment duration 4, 6 or 8 weeks 86 (Figure 2). The SVR rate was poor (27%) with the 4-week regimen in treatment-naïve patients with genotype 1 and without cirrhosis. The 6-week regimen was associated with a more optimal SVR rate ranging from 67% in patients with genotype 1 who had previously failed a DAA-containing regimen, to 93% in treatment-naïve patients with genotype 1 and without cirrhosis. The 8-week regimen was associated with an optimal SVR rate over 90% whatever the genotype or treatment history. The safety profile of the combination was good with headaches in 23% and diarrhea in 11% of patients. Overall the relapse rates were 19% in those treated for 6 weeks and 4% in those treated for 8 weeks. Moreover, the SVR rates were similar between patients who did and did not harbor baseline RASs. Only two patients had emergent RASs at the time of failure, confirming the high barrier to resistance of this regimen and suggesting the potential of this combination as a salvage regimen of DAA failure.
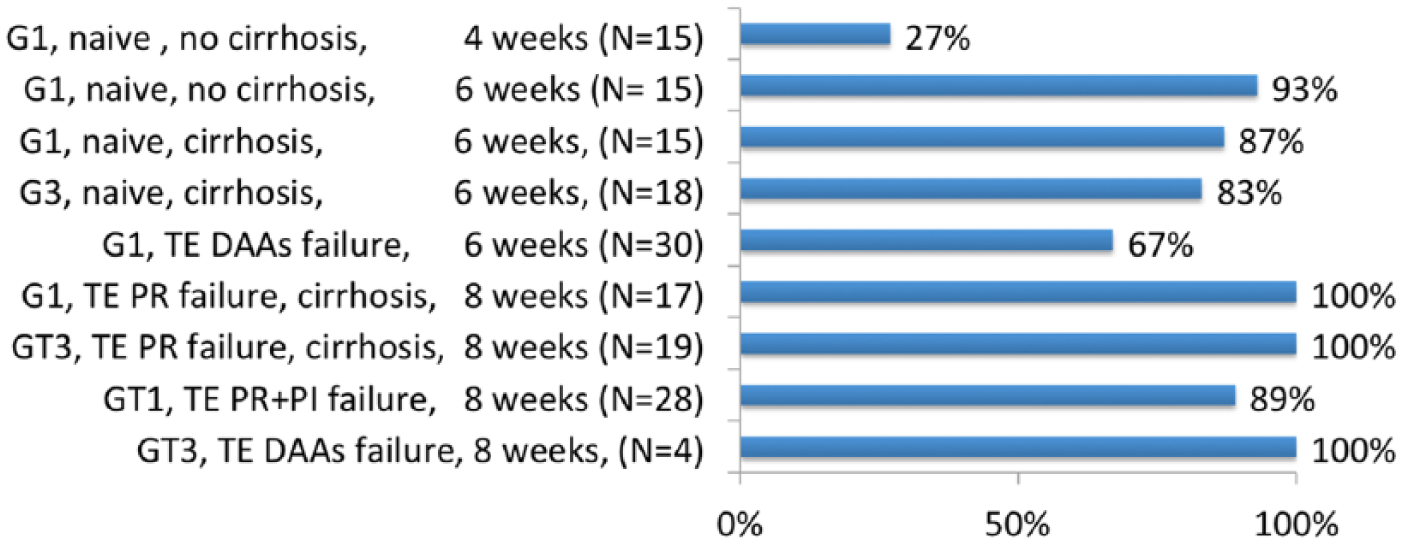
SVR in phase II studies with sofosbuvir/velpatasvir plus voxilaprevir. 86
The second phase II study evaluated the same combination SOF/VEL plus VOX 100 mg once daily in 128 HCV genotype 2, 3, 4 or 6 naïve or treatment-experienced HCV patients for various treatment durations of 6, 8 or 12 weeks. 87 The 6-week regimen achieved a suboptimal overall SVR rate of 88% in treatment-naïve patients without cirrhosis especially in those with genotype 2 and 4. In contrast, the 8-week regimen achieved a good SVR rate of 93% in treatment-naïve patients with cirrhosis. The 12-week regimen achieved an optimal SVR rate in treatment-experienced patients, including previous DAA failure (38 patients), ranging from 97% in patients with cirrhosis to 100% in patients without cirrhosis (Figure 3). One patient with genotype 3 and cirrhosis had a relapse with treatment-emergent NS3 RAS Q80R that does not confer in vitro resistance to VOX. The safety profile of the triple combination was good. Again, the SVR rates were similar between patients with or without baseline RASs, 92% versus 94% for naïve patients with cirrhosis treated for 8 weeks. In conclusion the triple combination appeared to be a well-tolerated and effective treatment in HCV patients of all genotypes with or without compensated cirrhosis.
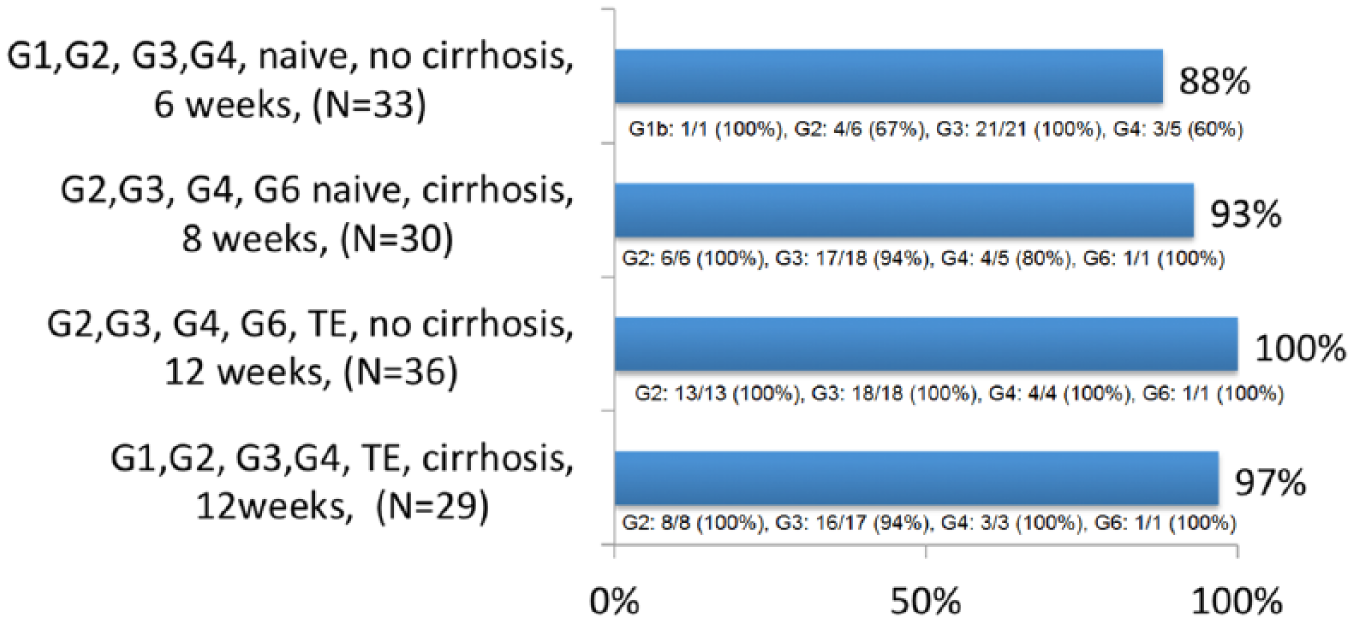
SVR in phase II studies with sofosbuvir/velpatasvir plus voxilaprevir. 87
The third phase II study evaluated the same combination of SOF/VEL plus VOX 100 mg once daily among 197 patients with genotype 1 for a 6–12 week treatment duration, plus RBV for treatment-naïve patients with cirrhosis. 88 In treatment-naïve patients without cirrhosis, 6 weeks of treatment achieved a suboptimal SVR rate (71%). In contrast, 8 weeks of treatment achieved an SVR in all patients. In treatment-naïve patients with cirrhosis, 8 weeks of treatment achieved an SVR rate of 87.5% with no benefit of RBV addition, 81% versus 94%. In treatment-experienced patients who previously failed a DAA regimen (46% with NS5A inhibitors, 54% with NS3/4A protease inhibitors and 39% with SOF) all patients with or without cirrhosis achieved SVR after 12 weeks of treatment (Figure 4). Overall, 18 patients relapsed and no patient experienced breakthrough. Overall, one patient died during follow up from atypical pneumonia. In this study the triple combination appeared well tolerated and effective for 8 weeks in treatment-naïve patients with no benefit of RBV addition. A 12-week treatment duration achieved an SVR in all 63 DAA-experienced patients with genotype 1.

SVR in phase II studies with sofosbuvir/velpatasvir plus voxilaprevir. 88
The last phase II study evaluated the same combination SOF/VEL plus VOX 100 mg once daily with or without RBV for 12 weeks in 49 patients with genotype 1 who previously failed a DAA regimen. 89 A total of 51% of patients had compensated cirrhosis at baseline and 12% of patients had already failed a 2 or 3 DAA regimen. All patients treated without RBV achieved SVR and 24 out 25 patients (96%) treated with RBV achieved SVR. Baseline RASs were present at baseline in 73% of cases and SVR was not different according to the presence of RASs (97% versus 100%). The only patient who relapsed was a black male with cirrhosis previously treated by SOF/LDV for 24 weeks. He had developed new RASs at relapse in both NS5A and NS3 domain. Overall this study demonstrated that 12 weeks of SOF/VEL/VOX was effective and well tolerated among patients with genotype 1 HCV who had previously failed a DAA-based regimen. Moreover, the potency of this regimen can obviate the need for RBV to be included in the regimen to maximize efficacy.
Phase III trials: the POLARIS studies
The phase III program had evaluated the triple FDC SOF/VEL/VOX for 8 weeks in treatment-naïve patients of all genotypes and for 12 weeks in patients of all genotypes who have received previous treatment with any DAA (Figure 5).

Naïve or treatment-experienced without DAA patients
The POLARIS 2 and 3 studies assessed the efficacy of 8 weeks of treatment with the triple FDC in HCV patients either naïve of treatment or treatment-experienced without DAAs in patients with or without compensated cirrhosis. 90 Patients were assigned randomly in groups and given triple FDCs for 8 weeks or dual FDCs (SOF/VEL) for 12 weeks.
POLARIS-2, enrolled patients infected with all HCV genotypes with or without cirrhosis, except patients with genotype 3 and cirrhosis. It was designed to test non-inferiority of 8 weeks of triple FDCs to 12 weeks of dual FDCs using a non-inferiority margin of 5%. A total of 941 patients began treatment, 77% were treatment-naïve, and 18.5% had compensated liver cirrhosis. Overall, 95% [95% confidence interval (CI), 93–97%] of patients had an SVR with 8 weeks of triple FDCs; this did not meet the criteria to establish non-inferiority to 12 weeks of dual FDCs, which produced an SVR in 98% of patients (95% CI, 96–99%; difference in the stratum-adjusted Mantel–Haenszel proportions of −3.2% 95% CI, −6.0 to 0.4%). The difference in the efficacy was primarily due to a lower rate of SVR (92%) among US patients with HCV genotype 1a infection receiving 8 weeks of triple FDCs. The relapse rate was observed in 4% of patients treated with triple FDCs for 8 weeks versus 1% in those treated with dual FDCs for 12 weeks. Baseline RASs to NS3 or NS5A inhibitors were found in 50% of patients. Of these, 94% had an SVR as compared with 98% for patients without RASs. Baseline Q80K RAS nevertheless was associated with a reduction in SVR rate for genotype 1a patients receiving a triple FDC regimen for 8 weeks, 88% with Q80K compared with 94% without. Only one patient had treatment-emergent NS5A RAS Q30R and L31M.
POLARIS-3, which enrolled patients with genotype 3 HCV infections and cirrhosis, compared rates of SVR between a group treated with 8 weeks of triple FDCs and another group treated with 12 weeks of dual FDCs with a performance goal of 83%. A total of 219 patients began treatment, 69% of them were treatment-naïve. Overall, 96% of patients achieved an SVR in both treatment groups, which was significantly superior to the performance goal that was based on the prior results of this dual therapy in this patients population in the ASTRAL-3 trial (SVR, 91%; 95% CI, 83–96). 63 Among the 67 treatment-experienced patients, the SVR rate was numerically higher in patients treated with triple FDCs compared with those treated with dual FDCs (97% versus 91%). All 46 patients with baseline RASs achieved an SVR. Neither of the two patients who relapsed after triple FDCs for 8 weeks had treatment-emergent RAS.
None of the 611 patients receiving 8 weeks of triple FDCs in both studies discontinued treatment owing to adverse events. Less than 3% of patients had serious adverse events, and one patient died during the follow up. The safety profile was fine. The most common adverse events with triple FDCs were headache (26%), fatigue (22%), diarrhea (17%) and nausea (16%). Mild gastrointestinal adverse events were associated with the regimen including VOX. Moreover in these two phase III studies, patient-reported outcomes (PROs) were collected. 93 During treatment, improvements in most PRO scores were significant. After treatment discontinuation, patients treated with both regimens achieved significant and clinically meaningful PRO gains.
Treatment-experienced DAA patients
The POLARIS 1 and 4 studies assessed the efficacy of 12 weeks of treatment with the triple FDCs in DAA treatment-experienced HCV patients with or without compensated cirrhosis. 91
POLARIS-1 enrolled 415 patients, infected with any HCV genotype, who previously failed a regimen containing an NS5A inhibitor. Patients with genotype 1 were randomly assigned in a 1:1 ratio to receive either the triple FDC (150 patients) or matching placebo (150 patients) once daily for 12 weeks. Patients who were infected by other genotypes (114 patients) were enrolled in the triple FDC once daily for 12 weeks. Of these patients, one patient with genotype 4 never received treatment. A total of 46% of patients had compensated cirrhosis. The most common NS5A inhibitors used in a previous unsuccessful treatment were LDV (55%), DCV (23%) and ombitasvir (13%). Overall, 39% of patients had received at least two or more previous HCV treatments. The rate of SVR was 96% compared with 0% with placebo. Overall the rate of SVR was 99% among patients without cirrhosis and 93% among patients with cirrhosis. According to HCV genotype, all patients with genotype 1b, 2, 5 and 6 achieved an SVR. The SVR rate was 96% in patients with genotype 1a, 95% in patients with genotype 3 and 91% in genotype 4. Baseline RASs were present at baseline in 83% of patients and 79% harbored NS5A RASs. The SVR rate was similar between patients with baseline RASs (96%) as compared with those without RASs (99%). A total of six patients with cirrhosis had a relapse (one patient with genotype 1a, four patients with genotype 3 and one patient with genotype 4). Overall, one patient with genotype 4 had treatment-emergent RASs and one patient had a breakthrough during treatment with low plasma concentration of the drug on treatment, suggestive of nonadherence.
A total of 147 genotype 1 patients who received placebo were subsequently treated with triple FDCs once daily for 12 weeks. 92 Overall, one-third of patients had cirrhosis and 77% of them were genotype 1a. Overall the SVR rate was 97%. Patients with cirrhosis had an SVR rate of 98% and those without cirrhosis had an SVR rate of 97%. The SVR rate was 97% for patients with baseline RASs and 100% in those without baseline RASs. Overall, four patients with genotype 1a, one with cirrhosis, experienced relapse. All had baseline RASs and two developed treatment-emergent RASs. Combining the data in the primary and sub-study of POLARIS-1, the overall SVR rate was 97% (396/409).
POLARIS-4 enrolled 333 patients who previously failed a DAA regimen without an NS5A inhibitor. HCV patients with genotype 1, 2 and 3 were randomly assigned in a 1:1 ratio to receive triple FDCs (163 patients) or dual FDCs (151 patients) for 12 weeks. An additional 19 patients with genotype 4 were enrolled in the triple FDC regimen for 12 weeks. 91 A total of 46% of patients had compensated cirrhosis. Overall, 85% of patients had received SOF as part of the previous regimen and 26% had received NS3/4A inhibitors. A total of 39% of patients had received at least two or more previous HCV treatments. Overall, the rate of SVR was 98% in patients receiving triple FDCs and 90% in those receiving dual FDCs. Among patients without cirrhosis the rate of SVR was 98% among those receiving triple FDCs and 94% among those receiving dual FDCs as compared with 98% and 86% respectively among patients with cirrhosis. According to genotype, the SVR rate was, for those receiving triple FDCs as compared with those receiving dual FDCs, in patients with genotype 1a, 98% versus 89%, in patients with genotype 1b, 96% versus 95%, in patients with genotype 2, 100% versus 97%, and in patients with genotype 3, 96% versus 85% respectively. A total of 49% of enrolled patients had baseline RASs to NS3 or NS5A inhibitors. Only 1 patient relapsed in those treated with triple FDCs as compared with 14 patients in those treated with dual FDCs. The patient who failed on triple FDCs had no baseline RASs and no treatment-emergent RASs.
The safety profile in the POLARIS-1 and 4 studies was good. The percentage of patients who discontinued treatment due to adverse events was 1% or lower. The most common adverse events with triple FDCs were headache, fatigue, diarrhea and nausea.
Moreover, in these two phase III studies, PROs were collected. 94 After 12 weeks of treatment some PRO scores improved in both the dual and triple FDC treatment groups but not in the placebo group. All increases in PRO scores were sustained or increased after the end of the treatment. There was no difference in PROs between dual or triple FDCs. These findings indicate the benefit of these regimens during treatment and after SVR.
Regulatory issues and guidelines recommendations
Results of the phase III studies lead to different approvals from US FDA and EMA.
On 18 July 2017, the US FDA approved SOF/VEL/VOX FDC for 12 weeks for adult HCV patients with or without compensated cirrhosis (Child–Pugh A) and any genotypes that have previously failed an HCV regimen containing an NS5A inhibitor. This regimen is also approved in patients with genotype 1a or 3 with or without compensated cirrhosis who have previously failed an HCV regimen containing SOF without a NS5A inhibitor. 95 Those approvals were implemented in the recent AASLD guidelines.
In contrast on 27 July 2017, the EMA approved SOF/VEL/VOX FDC with wider indications: 8 weeks of FDCs, any genotype, in treatment-naïve patients without cirrhosis and in patients with genotype 3 with cirrhosis; 12 weeks of FDCs, any genotype, in treatment-naïve patients with cirrhosis and, in treatment-experienced patients with DAA failures with or without compensated cirrhosis.
The last EASL guidelines have implemented few of the EMA approvals. FDC is recommended for 12 weeks in patients with genotype 3 with cirrhosis, either treatment-naïve or experienced. FDCs for 12 weeks is the first-line treatment recommended in patients with or without compensated cirrhosis who failed a previous regimen with DAAs, either a protease inhibitor or NS5A inhibitor. An alternative option is the combination of SOF plus GLE/PIB ± RBV for 12–16 weeks based on two small studies involving patients who failed previous DAA regimens, including the GLE/PIB regimen.96,97 The SVR rate was 96%. 96 In very difficult-to-cure patients with NS5A RASs who failed twice to achieve an SVR after several DAA regimens, including protease and N5A inhibitors, FDCs are recommended to be used either in combination with weight-based dose RBV or to extend the treatment duration to 16 or 14 weeks.
Conclusion
The FDC of SOF/VEL/VOX is a well-tolerated pangenotypic, once daily, single tablet regimen. The 8-week treatment has shown a very high efficacy, almost similar to the dual FDC SOF/VEL regimen for 12 weeks or the GLE/PIB regimen for 8 weeks in treatment-naïve patients or treatment-experienced without DAA patients, without cirrhosis of any genotype. In patients with compensated cirrhosis, 8 weeks of triple FDCs have shown similar efficacy as the dual FDCs for 12 weeks, except for patients with genotype 1a and cirrhosis. The EMA proposes to use triple FDCs for 12 weeks in patients with compensated cirrhosis with the exception of patients with genotype 3, for which strong data from POLARIS-3 demonstrated the efficacy of 8-week regimen. In DAA treatment-experienced patients, with or without compensated cirrhosis, 12 weeks of triple FDCs achieved a very high efficacy, even in patients with baseline NS5A RASs.
This triple FDC is a hallmark therapeutic achievement in HCV therapy for any genotype, fibrosis stage or previous DAA failure. One pill that fits all is therefore nearly achievable. In combination with other pangenotypic options available, such as dual combination (SOF/VEL or GLE/PIB) or triple combination SOF plus GLE/PIB, we can expect to be near the end of the HCV cure road.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The following are declared: M. Bourlière: advisory board and speaker for: Gilead, AbbVie, MSD, BMS, Janssen, Boehringer-Ingelheim; Paul Castellani: speaker for Gilead, AbbVie, Janssen, and MSD; Valérie Oules: speaker for Gilead, AbbVie, Janssen, MSD; Xavier Adhoute: speaker for Bayer.