
Abstract
Background:
Episodes of hepatic encephalopathy (HE) have been related to low survival rate. However, the relation between its clinical evolution and mortality has not been assessed.
Methods:
A retrospective analysis of 245 cirrhotic patients admitted for an acute episode of HE (⩾grade 2) or who developed an HE episode after an upper gastrointestinal bleeding (UGIB) event was performed to assess the relation between time in HE and transplant-free survival.
Results:
Median (IQR25–75) time in HE was 48 h (24–96 h) in the whole cohort. Patients who presented a longer time in HE (>48 h; n = 89) exhibited a lower transplant-free survival at 28 days (67.2% versus 88.9%, p < 0.001), 90 days (48.7% versus 73.8%, p < 0.001) and 365 days (30.3% versus 53.2%, p < 0.001), as compared to those with less time in HE (⩽48 h; n = 156). Survival rates remained significantly different, with lower percentages in the group with time in HE >48 h, when comparing patients according to baseline HE grade (2 versus ⩾3) or model for end-stage liver disease (MELD) function (⩽15 versus >15). Time in HE was also an independent risk factor for mortality at each time point, hazard ratio (HR) (95 CI%) 28 days 2.59 (1.39–4.84); 90 days 1.98 (1.28–3.1) and 365 days 1.5 (1.08–2.19).
Conclusions:
The duration of the acute HE episode determines survival in cirrhotic patients independently of liver function and baseline HE grade.
Introduction
Hepatic encephalopathy (HE) impacts on survival and could be an ominous event in critically ill cirrhotic patients. 1 The first epidemiological studies performed in cirrhotic patients with HE showed survival probabilities at 1 and 3 years of 42% and 23% respectively. 2 A recent study confirmed higher mortality rates at 28, 90 and 365 days in decompensated cirrhotic patients suffering from HE at hospital admission, when compared to decompensated cirrhotic patients without HE. 3
HE is not only a key factor in mortality, but also a main concern for public health, because it accounts for 100,000–115,000 yearly admissions in the USA and is associated with high resource utilization. 4 HE is also a main factor in quality of life and daily functioning of cirrhotic patients,5,6 and it has been associated with a higher number of road traffic accidents, 7 even in its minimal clinical spectrum. 8 In addition, the presence of acute-on-chronic liver failure (ACLF) at hospital admission involves a poor survival prognosis, but even in patients with ACLF the presence of HE at admission confers a worse vital prognosis. 3
Multiple drugs have been tested and are used in overt HE: non-absorbable disaccharides, antibiotics (rifaximin, paromomicin and neomicin), branched-chain amino acids (BCRAAs) and ammonia scavengers. In many of the efficacy studies of these drugs, the time that the patient remains in HE or the time to present an improvement in the HE grade have been used as relevant endpoints. Although the relevance of these parameters seems obvious, their association to survival has not been established.
In the present study, we aimed to assess whether there was an association between the duration of the acute HE episode and mortality.
Patients and methods
This is a retrospective analysis of patients who had been admitted with an HE episode grade 2 or above, or developed HE grade 2 or above during hospitalization, belonging to six cohorts of patients from two liver units (Hospital Vall d’Hebron, Barcelona and Unit for the Clinical Management of Digestive Diseases, Sevilla) (Figure 1).
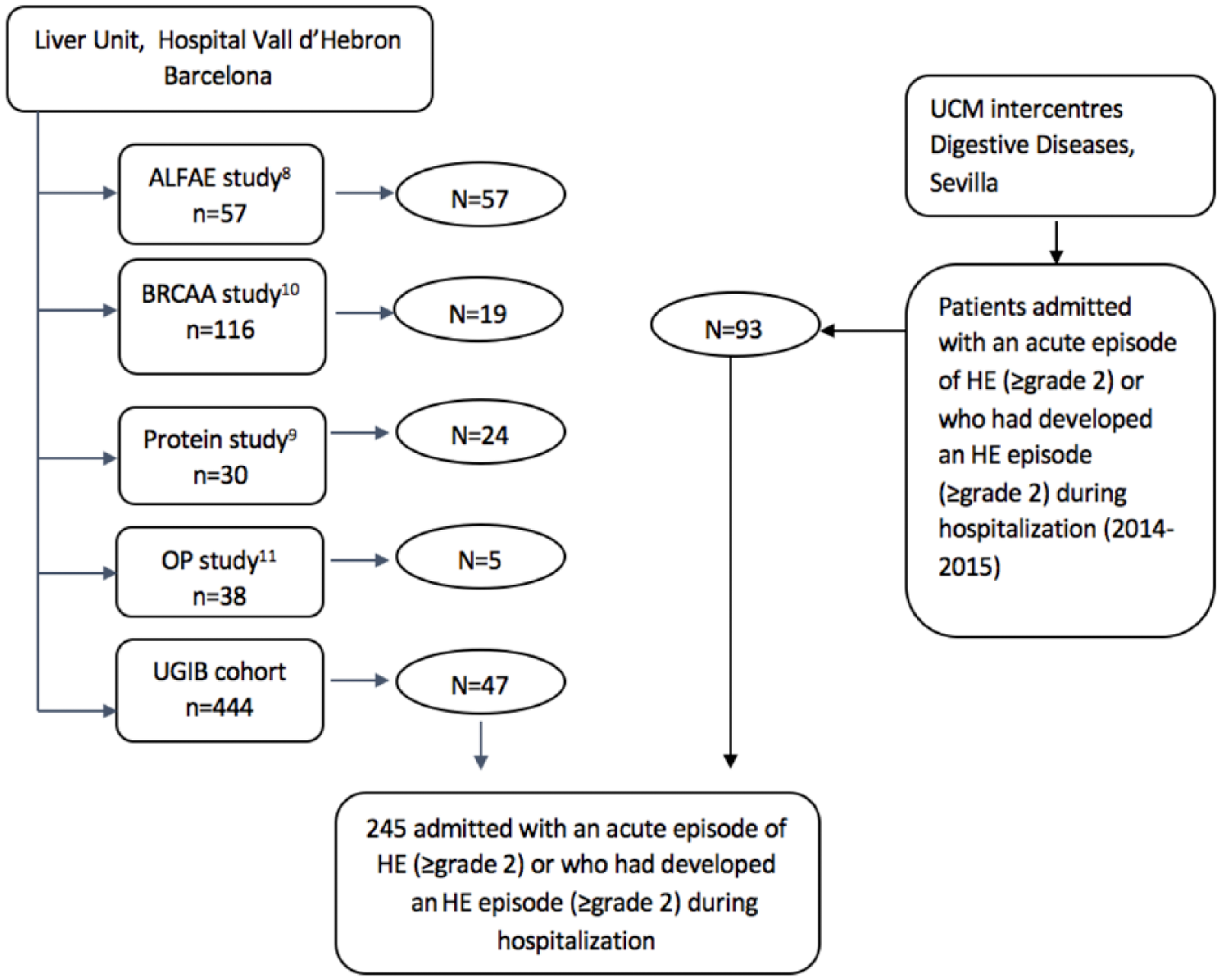
Patients flow chart.
Patient data from Barcelona were obtained from four randomized trials on different therapies for HE9–12 and from a prospective cohort of consecutive cirrhotic patients with acute variceal bleeding admitted to Hospital Vall d’Hebron (2004–2015) 13 (Supplementary Material 1). Patients from Sevilla were specifically recruited for this study by including all the consecutive cirrhotic patients admitted in the hospital during 2014 with an acute HE episode of grade ⩾2. The presence of HE was diagnosed as an impairment of cognition, consciousness or motor function in patients with cirrhosis after exclusion of other causes of mental disturbances. The severity of HE was assessed according to the West Haven scale. 14 The study was approved by the ethics committees of both hospitals (PR(AG)291/201); the need for informed consent was waived by the ethics committee.
Clinical parameters and definitions
At enrollment, the following data were collected: clinical history (demographic data, previous disease, previous episodes of acute decompensation), physical examination, laboratory measurements and events that might be potential precipitating factors of HE, such as diuretic use (within 3 months prior to enrollment), presence of bacterial infections, gastrointestinal hemorrhage or hyponatremia. Length of hospitalization and complications during hospitalization (infections, bleeding, hepatorenal syndrome, recurrence of HE episode during hospitalization and presence of ACLF) were also recorded.
The time that a patient remained in overt HE (grade ⩾2) was defined as time in HE. Resolution of HE was defined as an improvement in the HE grade to grade 1 or to the absence of HE, as defined in the clinical guidelines.15,16 Data were recorded in 12 h time frames. A time in HE of 48 h was chosen as a cut-off based on the median (IQR25–75) time of HE resolution among the whole cohort 48 h (24–96 h). A model for end-stage liver disease (MELD) cut-off of 15 was chosen in this study as an indicator of different liver disease severity. The cut-off was selected based on other studies showing a flat survival curve (with survival rates of 100% at 3 months) in patients with a MELD score below 15, while the survival curves started to decrease within patients with a MELD score >15 in a logarithmic manner. 17 Moreover, other studies have showed a significant correlation between observed and predicted mortality curves among patients with a MELD score between 10 and 19. 18 For Child–Pugh assessment only the hepatic synthetic and portal elements of Child–Pugh were used (modified Child–Pugh) due to the fact that all the patients included in the study presented with HE grade ⩾2 as per protocol. Three categories were assessed according to the punctuation category: A (4–6), B (7–9) and C (10–12). 19 For the survival analyses HE was divided into two categories: moderate HE (grade 2) and severe HE (grades 3 and 4). Mortality and liver transplantation at 28, 90 and 365 days of follow up and causes of death were also recorded.
Statistical analyses
Results are presented as frequencies and percentages for categorical variables, means and standard deviations for normal continuous variables and median, quartile 1 and 3 for not normal continuous variables. In all analyses, the significance level was set at p < 0.05. Survival at 28, 90 and 365 days was assessed with the Kaplan–Meier method and the log-rank Mantel–Cox test. For statistical analysis of survival, we used transplant-free survival (based on the consideration that transplantation at a given time clearly modifies the probability of death of a specific patient at each subsequent time point). Factors showing a clinically and statistically significant association to the outcome in univariate analyses (Mantel–Cox test) were selected for the initial models. The final models were fitted by using a step-wise forward method based on model likelihood ratios (Cox regression for survival analysis) with the same significance level (p < 0.05) for entering and dropping variables. The IBM SPSS Statistics version 20.0 was used for statistical calculation.
Results
A total of 245 patients were included (Figure 1): 146 patients (59.6%) with HE grade 2 and 99 patients (40.4%) with HE grade >2. Most patients were males with alcohol as the predominant etiology of cirrhosis, and within modified Child–Pugh class B; almost 85% of the patients had presented with previous decompensation (Table 1). The most frequent decompensation at admission was ascites, followed by bacterial infection. Only 15.7% of the patients presented with ACLF. Nearly 75% of the patients had used diuretics in the previous 3 months.
Baseline characteristics of patients included in the study.

ACLF, acute-on-chronic liver failure; HE, hepatic encephalopathy; HSR, hepatorenal syndrome; IQR, interquartile range; MELD, model for end-stage liver disease; SBP, spontaneous bacterial peritonitis; SD, standard deviation; UGIB, upper gastrointestinal bleeding.
♦Patients not recovering from the first HE episode were not included (n = 32).
p < 0.001 between HE grade 2 and 3/4.
∆ Child–Pugh was only calculated for patients with all the information available.
The median time that the patients stayed in overt HE (time in HE) was 48 h (24–96) (Table 1). Patients with HE grade 3/4 remained in HE for a longer time when compared to patients with HE grade 2.
Survival
The transplant-free survival for the whole cohort was 78.4% at 28 days, 61.6% at 90 days and 42% at 1 year. Patients who presented with HE grade 2 at admission exhibited higher survival rates than those with grades 3/4 at any time point: 28 days (84.4% versus 70.9%, p = 0.005), 90 days (70.0% versus 50.9%, p = 0.002) and 365 days (47.4% versus 35.5%, p = 0.027).
Patients who had longer than 48 h in HE exhibited a lower transplant-free survival rate as compared to those with a shorter time in HE (⩽48 h) at 28 days (67.2% versus 88.9%, p < 0.001), 90 days (48.7% versus 73.8, p < 0.001) and 365 days (30.3% versus 53.2%, p < 0.001) (Figure 2). Similarly, patients who had a time in HE higher than 24 h, 36 h or 72 h also exhibited a lower transplant-free survival rate as compared to those with a shorter time in HE (⩽24 h, ⩽36 h or ⩽72 h) (Supplementary Material 2).
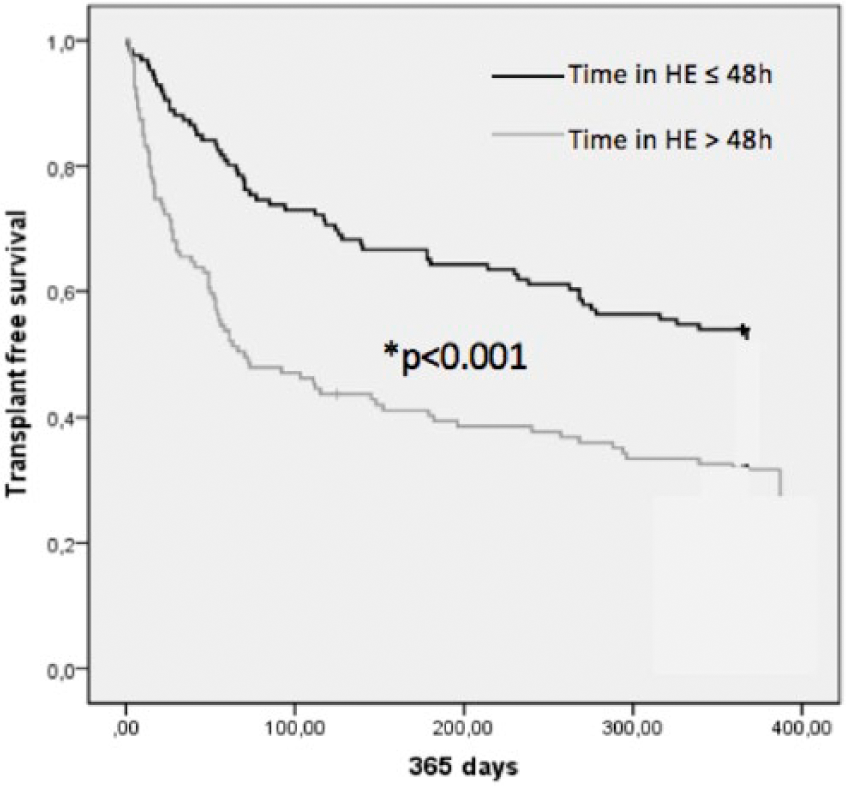
Transplant-free survival of patients included in the study in relation to time in HE. Patients with a time in HE >48 h versus those with time in HE ⩽48 h presented lower transplant-free survival rates at any time point with *p < 0.001 at 28, 90 and 365 days.
The effect on survival of the time in HE was maintained when patients were divided into subgroups of liver function according to MELD score. As seen in Figure 3(a), differences in survival were observed for all time points between patients with shorter or longer time in HE among the subgroup of patients with MELD ⩽15 and MELD >15. Remarkably the survival curves between patients with a MELD score ⩽15 and time in HE >48 h and those with MELD score >15 and time in HE ⩽48 h showed a similar survival rate distribution.
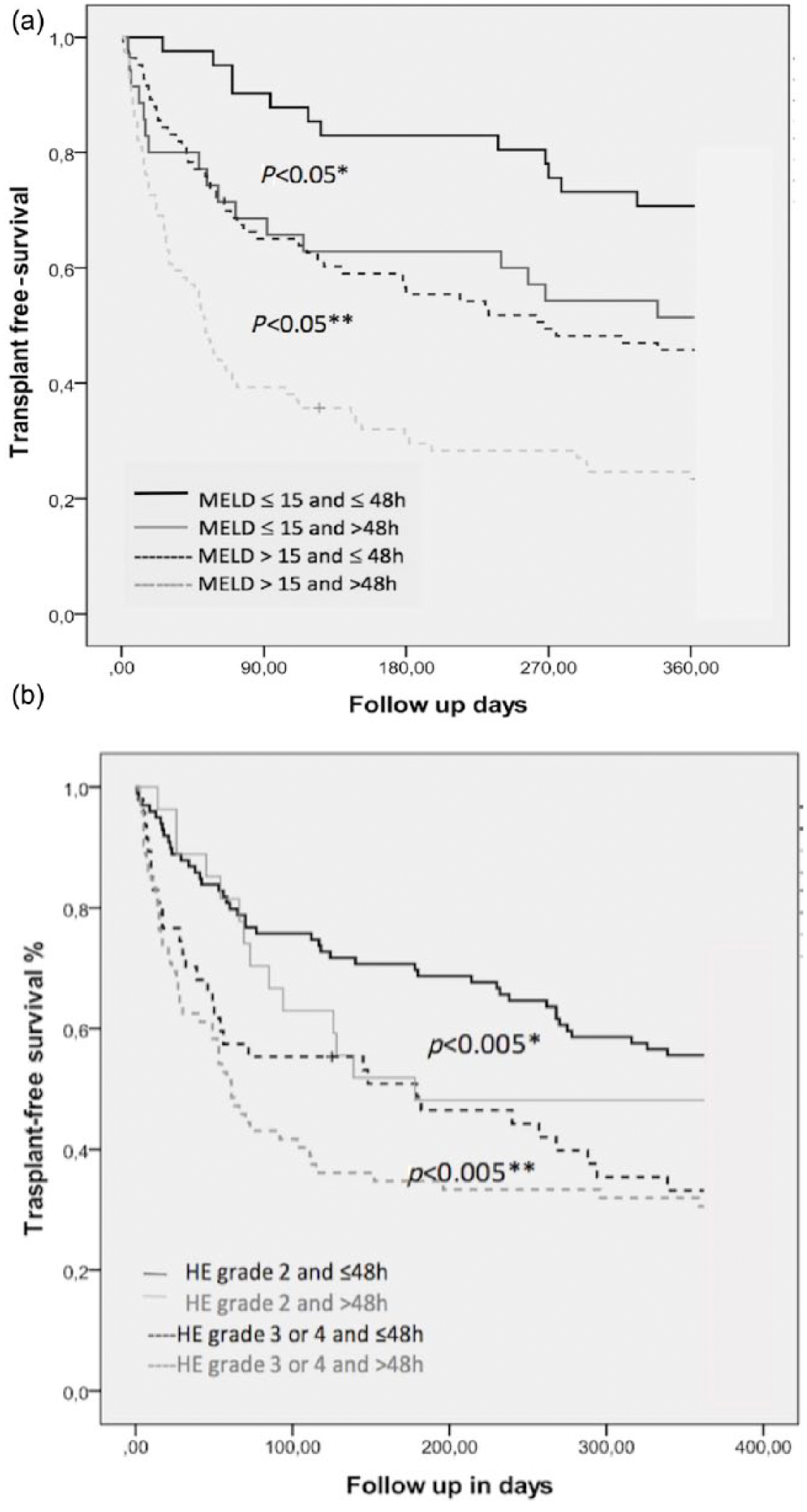
(a) Transplant-free survival of patients included in the study in relation to time in HE and MELD score; (b) transplant-free survival of patients included in the study in relation to time in HE and HE grade.
Similarly, as depicted in Figure 3(b), the effect on survival of the time in HE persisted when patients were classified in subgroups according to baseline HE grade. As observed, differences in survival were seen at all time points between patients with ⩽48 h and >48 h in HE among the subgroups with baseline HE grade 2 and with HE grades 3/4. Again, it is worth mentioning that the survival curves between patients with HE grades 3/4 and time in HE ⩽48 h and those with HE grades 2 and time in HE >48 h showed a similar pattern (Figure 3(b)).
HE recurrence during hospitalization occurred in 40 patients (16.3%). Although transplant-free survival rates were lower among patients with HE recurrence during hospitalization compared to patients without HE recurrence (28 days, 72.5% versus 9.5; 90 days, 57.5% versus 62.4%; and 365 days, 30% versus 44.4%), the differences did not reach statistical significance at any time point.
Risk factors for mortality at 28, 90 and 365 days were MELD score, presence of ACLF, HE degree and time in HE. Age was only a risk factor at 365 days. Only MELD score and time in HE remained significant in the multivariate analysis at any time point (Table 2). The main cause of death during follow up was cirrhosis-related complications (63%), being the most common HE (21.8%), followed by infections (14%); up to 20% died from extrahepatic causes and 13% of the patients underwent a liver transplant.
Risk factors for short-, medium- and long-term follow up in patients with HE grade ⩾2; multivariate analysis.

ACLF, acute-on-chronic liver failure; HE, hepatic encephalopathy.
Comparison of clinical characteristics between patients with a time in HE >48 h and ⩽48 h
In total, 106 patients recovered within the first 48 h, while up to 119 patients presented a time in HE longer than 48 h (Table 3). MELD score and percentage of Child–Pugh A, B and C patients did not differ across both groups; creatinine levels were slightly higher in the HE >48 h group. No sex, age or differences in the main cirrhosis etiologies differences were detected between both groups. Similar percentages of previous decompensations at admission were observed and up to 26% of patients in the HE >48 h group presented with ACLF (11 patients grade I, 10 grade II and 5 grade III), as compared to 10.3% in the other group (9 patients grade I, 2 grade II and 2 grade III) (p = 0.014). Remarkably, the use of rifaximin during the previous 3 months to admission was significantly higher among patients with a time in HE ⩽48 h (21.4%), as compared to patients with time in HE >48 h (10.9%), even though the proportion of previous HE events were similar between both groups. Up to 60.5% of the patients with a time in HE >48 h exhibited HE grades 3/4 at admission, while it was present in only 22% of the patients with a time in HE <48 h; although these differences are relevant, as showed in Figure 3(b), survival was influenced by time in HE independently of HE grade at admission.
Characteristics of patients by time in HE ⩽48 h or >48 h.
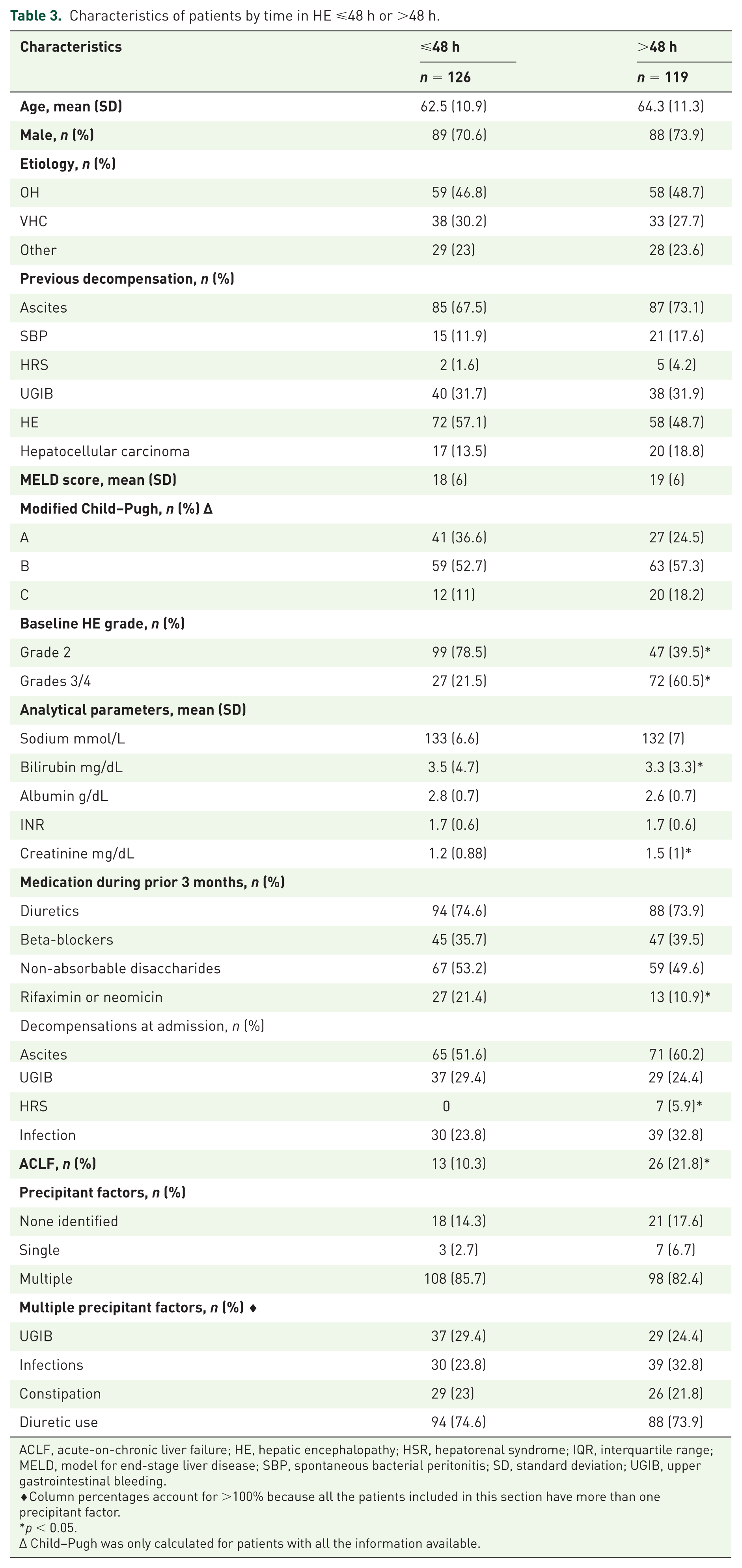
ACLF, acute-on-chronic liver failure; HE, hepatic encephalopathy; HSR, hepatorenal syndrome; IQR, interquartile range; MELD, model for end-stage liver disease; SBP, spontaneous bacterial peritonitis; SD, standard deviation; UGIB, upper gastrointestinal bleeding.
♦Column percentages account for >100% because all the patients included in this section have more than one precipitant factor.
p < 0.05.
∆ Child–Pugh was only calculated for patients with all the information available.
Discussion
The results of the present study indicate that the time that a cirrhotic patient remains in overt HE during an acute episode is a clinically relevant parameter with strong prognostic implications. This effect is equally observed when patients with different baseline HE grades (grade 2 versus grades 3/4) were analyzed separately. Indeed, patients with HE grade 2 who remained in HE for >48 h presented similar survival rates to patients with HE grades 3/4 and short durations of the HE episode (Figure 3(b)).
Perhaps more remarkable is the fact that the influence of time in HE on survival seems to be independent of the baseline liver function. This is highlighted by the results of the multivariate analysis, but especially by analyzing separately the effect of time in HE in the subgroups of patients with low (⩽15) and high MELD scores (>15). Again, it is worth emphasizing that patients with better liver function (MELD ⩽15) who remained in HE for >48 h showed almost equal survival curves to patients with worse liver function and a shorter time in HE (Figure 3(a)). In fact, the effect of time in HE >48 h on survival in the short, medium and long term is also present when we increase the MELD cut-off point to 21, a validate cut-off in patients with alcoholic hepatitis, 20 one of the deadliest complications in alcoholic cirrhotic patients. Once more, patients who remained in HE for >48 h exhibited higher mortality rates at any time point. Interestingly, patients with better liver function (MELD ⩽21) who remained in HE for >48 h showed almost equal survival curves to patients with worse liver function and a shorter time in HE (data not shown). This again supports the statement that time in HE is an independent mortality risk factor.
The appearance of HE during the course of the natural history of cirrhosis negatively impacts on the survival of patients. This is not only due to the mortality associated with the acute HE episode, but also because HE is an expression of a deteriorated liver function. Most clinicians would agree that the shorter the time the patient is in overt HE, the better; the longer the time the patient remains at a low level of consciousness, the higher the probabilities of serious complications (bronchoaspiration, infection, etc.). Although these are reasonable empirical assumptions, it has never been analyzed and proved that the length of time cirrhotic patients persists in overt HE has a direct impact on survival rates. From our data, it can be concluded that there is a 20% decrease in survival rates among patients who persist in HE for >48 h at short-, medium- and long-term follow up.
Our study also has other important implications for clinical trials assessing the effects of new drugs on HE. As already known, multiple drugs have been tested in clinical trials and are currently used for HE: non-absorbable disaccharides, 21 antibiotics (rifaximin, paromomicin and neomycin), 22 BCRAA, 23 and ammonia scavengers.12,24,25 The primary endpoint of the different intervention studies in HE has been variable. Some studies have utilized as the main endpoint surrogate analytical parameters, such as ammonia plasma levels.12,26,27 A few studies have included mortality as one of the secondary endpoints, but never as the primary endpoint.9,22,28 Finally, the most common primary endpoint evaluated in clinical trials of HE has been the reduction in the time to HE resolution or to HE improvement. This was used as a primary objective in the first HE clinical trial with lactulose 29 and it has been repeatedly utilized in most clinical trials in patients with overt HE, independently of the tested drugs.30–36 In this context, the data obtained from our study become highly relevant for establishing a direct relation with mortality, and suggest that any tested drug that significantly decreases the rate of patients with time in HE >48 h could have a potential impact on overall survival. Similarly, patients who presented a time in HE higher than 24 h, 36 h or 72 h also exhibited a lower transplant-free survival rate as compared to those with a shorter time in HE (⩽24 h, 36 h or 72 h)
It is important to highlight that the use of rifaximin during the previous 3 months to admission was significantly higher among patients with a time in HE ⩽48 h (21.4%), as compared to patients with time in HE >48 h (10.9%). This was partially explained by the fact that the use of rifaximin as a secondary HE prophylaxis was approved after 2010, 37 and up to 50% of the patients in our cohort were admitted before 2010. The use of rifaximin during the months prior to the HE episode might play a role in the duration of the HE episode, but unfortunately we do not have data regarding the compliance with medications prior to the inclusion in the different studies.
Our study has some limitations. The most important is probably the retrospective nature of the analysis, especially for the Barcelona patients. Although most of the Barcelona data originated from prospective clinical trials, ensuring the quality of the data, these trials were not designed to specifically evaluate time in overt HE. Consequently, unwanted bias or mistakes retrieving the data cannot be excluded. Also, the fact that the information about the time in HE was recorded in 12 h time frames, although it has facilitated the analysis, could have caused a loss of accuracy and, again, selection bias. Despite these limitations, we feel a strength of the study is the fact that the effect of time in overt HE on mortality seems to be consistently similar at every time point, in patients with different baseline HE grades, and in patients with different baseline liver function.
In summary, the present study indicates that the time that a cirrhotic patient remains in overt HE during an acute episode correlates with survival, and therefore it could be used as a surrogate for mortality in clinical trials of HE.
Footnotes
Funding
MST is a recipient of a Río Hortega grant from Instituto de Salud Carlos III, Spain. JG is a recipient of a Research Intensification grant from Instituto de Salud Carlos III, Spain. MVC is a recipient of a scholarship grant for study extension abroad, sponsored by the Spanish Association for the Study of the Liver. The study was partially funded by grants PI14/00331 and PI15/00066 from Instituto de Salud Carlos III, Spain and co-funded by European Union (ERDF/ESF, ‘Investing in your future’). CIBERehd is supported by Instituto de Salud Carlos III, Spain.
Conflict of interest statement
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.