
Abstract
Background:
The incidence, recurrence, and all-cause mortality rate for Clostridium difficile-associated diarrhea (CDAD) has increased markedly over the past 10 years despite treatment. Low vitamin D levels are known to impair immune responses to infection and are associated with increased mortality. We compared the role of patient comorbidity measured by the Charlson Comorbidity Index (CCI) with vitamin D levels to ascertain whether vitamin D levels were an independent variable affecting the outcome of CDAD or a marker of overall comorbidity.
Methods:
A prospective cohort study studied 62 patients hospitalized between 2008 and 2009 with manifestations of CDAD and a positive C. difficile toxin assay. All patients received standard antibiotics (metronidazole and/or vancomycin). Their status at 30-day follow up was classified as resolved or recurred/expired. Patients’ CCI was calculated using their medical history. Logistic regression analysis of variables including 25-hydroxyvitamin D, CCI, age, gender, white blood cell count (WBC), albumin and residence type were performed.
Results:
There were 62 patients (43.6% men, 56.4% women) with CDAD; mean age was 75 ± 17 years. At 30-day follow up, 28 (45.2%) expired, 10 (16.1%) had persistent or recurrent diarrhea and 24 (38.7%) resolved. Nonresolution was seen in 38 (61.3%). There was no significant association between 30-day resolution status and CCI, gender, WBC, albumin level or residence type. Two variables were found to be independent predictors of resolution of CDAD: normal vitamin D levels (p = 0.028) and age <70 years (p = 0.024). Subjects with low vitamin D were 4.75 times more likely to fail to resolve CDAD than subjects with normal Vitamin D.
Conclusion:
In this study, vitamin D level and age are independent predictors of CDAD resolution in hospitalized patients. Low vitamin D levels and age >70 years old are associated with increased likelihood of recurrence. Low vitamin D levels are not a marker of comorbidity or advanced age.
Keywords
Introduction
Clostridium difficile-associated diarrhea (CDAD) is the most common cause of infectious diarrhea associated with exposure to healthcare settings. Amongst hospitalized patients, CDAD leads to prolonged stays, increased morbidity and mortality and increased healthcare costs [McDonald et al. 2012]. In a recent US survey, there were 336,600 hospitalizations that involved a diagnosis of CDAD: nearly 1% of all hospital stays. In a time when the incidences of other healthcare-associated infections are diminishing, CDAD is increasing with only a recent leveling off [Lucado et al. 2012]. Expenditures have also risen, with the current cost for CDAD healthcare in the United States averaging US$3.2 billion annually [O’Brien et al. 2007]. Hospitalized patients with CDAD, independent of age or comorbidity, are also 2.74-fold more likely to die during their hospital stay than all other hospitalized patients [Wenisch et al. 2012].
Hypovitaminosis D is known to cause impaired innate and adaptive immune responses to infection [Hewison, 2012]. In a recent study, vitamin D deficiency was linked to adverse and more costly outcomes in veterans with C. difficile and methicillin-sensitive Staphylococcus aureus infections [Youssef et al. 2010]. Low vitamin D levels increases susceptibility to influenza [Cannell et al. 2006], tuberculosis [Arnedo-Pena et al. 2011] and human immunodeficiency virus acquisition [Sanchez de la Torre et al. 2008; Talat et al. 2010]. Hypovitaminosis D is also associated with autoimmune diseases—insulin-dependent diabetes mellitus, inflammatory bowel disease, multiple sclerosis and rheumatoid arthritis have all been implicated [Cantorna and Mahon, 2004]. Moreover, hypovitaminosis D has been associated with a higher risk of all-cause mortality in hospitalized patients [Melamed et al. 2008]. Previous reported risk factors that are associated with CDAD include severity of underlying illness, antibiotics usage, advanced age, prior hospitalization, usage of proton pump inhibitors, gastrointestinal surgery, use of feeding tubes and retirement home residence [Vesteinsdottir et al. 2012].
In view of the impact of hypovitaminosis D on the immune system, infectious disease and overall mortality, we sought to investigate the role of vitamin D in CDAD. In a prospective cohort study, we measured vitamin D levels in all hospitalized patients diagnosed with CDAD to assess the impact of low vitamin D levels in CDAD resolution. We further sought to isolate vitamin D as an independent variable in CDAD resolution by calculating the Charlson Comorbidity Index (CCI) in all patients.
Materials and methods
A prospective cohort study was performed on all patients hospitalized between May 2008 and June 2009, with manifestations of CDAD and a positive C. difficile toxin assay. All patients received standard antibiotic treatment with metronidazole and/or vancomycin. Systemic antibiotic usage after discharge was not recorded. Demographic variables such as gender, age (dichotomized to <70 years old or >70 years old), residence (nursing facility or home) were examined. Baseline values of 25-hydroxyvitamin D, white blood cell count (WBC) and albumin were also collected. 25-hydroxyvitamin D levels less than 21 ng/ml was considered to be low; while WBC greater than 20,000/µl was considered in the high range. Patients were followed at 30 days post-discharge by telephone survey. At the 30-day follow up, a patient was classified as having resolved, recurred or expired. A patient who had diarrhea at 30 days post-discharge or died, was considered ‘not resolved’.
To minimize comorbidity from obscuring the relationship between vitamin D and CDAD resolution and improve internal validity of the study, each patient’s CCI and age-adjusted CCI was calculated using their medical history. The CCI was developed in 1987 based on internal medicine patients admitted to a single New York hospital and their 1-year mortality rates. The index includes 19 medical conditions weighted as 1, 2, 3 or 6 (Table 1). The weight was assigned based on the magnitude of the adjusted relative risks each comorbidity held in a Cox proportional hazards regression model [Charlson et al. 1987]. CCI has been compared with six other indices of comorbidity showing concurrent validity, as well as predictive validity for length of stay, mortality, disability and readmissions [De Groot et al. 2003]. The weighted conditions provided a sum score to yield the total comorbidity score; which was adapted to account for increasing age. One point was further added for each ten year period, starting at the age of 50 years, and is added to previous comorbidity score.
List of comorbidities according to the Charlson Comorbidity Index score.

The primary outcome variable is the status of the CDAD patient at 30 days post-discharge. Patient outcome was classified into two groups: expired/recurred versus resolved. Expired was defined as mortality from any cause within the 30-day observation period. Differences between groups were assessed using the t-test or the Mann–Whitney test, as appropriate, for continuous variables. For categorical variables, the chi-squared test or Fisher’s exact test was used accordingly. A multivariate logistic regression analysis was carried out with 30-day status as the event of interest.
The following variables were used in the multivariate analysis: vitamin D status, gender, WBC (normal versus high), residence (nursing home versus home), age (years) and CCI. A backward elimination algorithm was applied in order to determine which factors were most associated with the 30-day status. From the final model, adjusted odds ratios were estimated along with the corresponding 95% confidence intervals.
Results
A total of 62 patients completed the study with the gender distribution of 43.6% males and 56.4% females. The mean age was 75 ± 17 years. Males were significantly younger than females (68.30 ± 17.61 versus 80.06 ± 15.36; p = 0.0023) (Table 2).
Patient characteristics. Data are presented as mean ± standard deviation or n (%).

CCI, Charlson Comorbidity Index; WBC, white blood cell count.
At 30-day follow up, 28 expired (45.2%), 10 (16.1%) had persistent or recurrent diarrhea and 24 (38.7%) resolved. In total 38 (61.3%) were not resolved. There was no significant association between 30-day resolution status and gender, WBC, type of residence and CCI. In addition, the mean albumin level in patients who resolved was 2.91 versus 2.54 in patients who did not resolve (p = 0.064), which did not reach statistical significance. However, there was a higher proportion of patients with low vitamin D levels who did not resolve as compared with those patients with normal vitamin D levels (71% versus 46%; p = 0.047).
Two variables were found to be independent predictors of resolution of CDAD, normal vitamin D levels (p = 0.028) and age (p = 0.024). Patients with low levels of vitamin D were 4.75 times more likely to recur or expire than patients with normal levels of Vitamin D (Table 3). In addition, with each additional year in age, patients were 1.06 times more likely to recur or expire (odds ratio [OR] = 1.06, 95% confidence interval [CI] 1.01–1.11; p < 0.024). More practically, the OR for a 10-year increment in age was 1.8. Consequently, the odds of recurrence or death increases 80% (100 × (1.8 – 1)) for every 10-year increase in age, assuming all other variables remain constant.
Logistic regression for 30-day status (recurred/expired versus resolved).
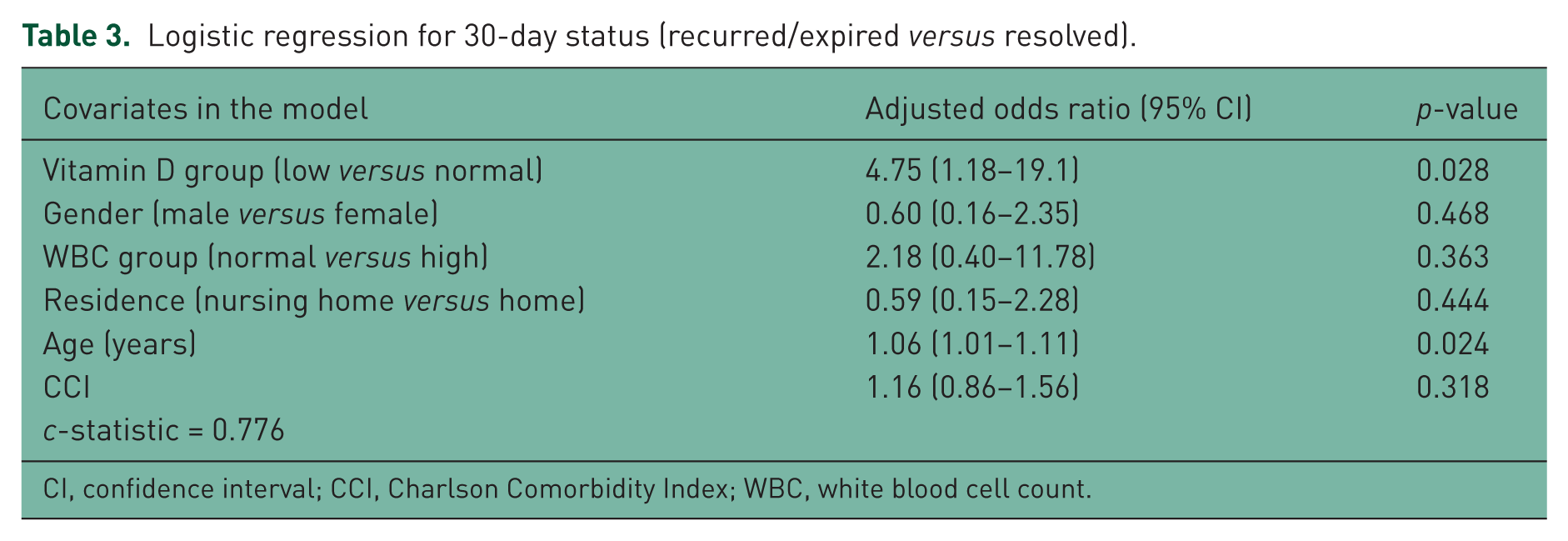
CI, confidence interval; CCI, Charlson Comorbidity Index; WBC, white blood cell count.
Using a backward elimination algorithm we arrived at a more parsimonious model with only vitamin D status and age in the model (Table 4), where the odds of recurrence or death was 5.6 times higher in subjects with low vitamin D levels than in subjects with normal vitamin D levels (OR = 5.6, 95% CI 1.5–21.1; p < 0.012) and for every 10-year increment in age, the odds of recurrence or death is 1.8 times higher (OR = 1.8, 95% CI 1.1–2.6; p < 0.008).
Logistic regression for 30-day status (recurred/expired versus resolved): reduced model after backward elimination.

CI, confidence interval.
Discussion
Our findings suggest that vitamin D level and age are independent predictors of CDAD resolution in hospitalized patients. We utilized the CCI to correct for comorbid conditions that may confound the relationship between vitamin D and CDAD resolution. In other words, low vitamin D is not simply a marker of comorbidity, but is in fact an independent predictor of poor outcomes in CDAD patients. Patients with hypovitaminosis D had a nearly five times greater likelihood of nonresolution of CDAD than patients with normal vitamin D levels. Older patients aged 70 years or higher, were also found to be less likely to have CDAD resolution.
There is a high rate of recurrent disease following treatment with metronidazole or vancomycin (20.2% and 18.4%, respectively) [Kelly and LaMont, 2008]. Utilization of either medication impairs resistance to colonization, thereby facilitating recurrent infections, which is seen within 4 weeks after therapy completion. Recurrence can be due to persistence of the strain responsible for the initial episode or reinfection with a different strain of C. difficile [Wilcox et al. 1998]. Host immunity plays a role, as there is a dramatic escalation of risk of recurrence in patients who have already had one recurrence. The recurrence risk rises from around 20% after an initial episode, to about 40% after a first recurrence and to over 60% with two or more recurrences [Kelly and LaMont, 2008]. Previous studies have identified various risk factors for recurrent disease; these include persistence of spores possibly in colonic diverticula [McFarland et al. 2002], continuation of systemic antibiotics [Alfa et al. 1999], lower reported quality-of-health [McFarland et al. 1999] and colonization with vancomycin-resistant enterococci [Choi et al. 2011]. This is the first study to date that has identified a link between low vitamin D levels and failure to resolve C. difficile enteritis. By assessing the CCI in all patients, we were also able to demonstrate that poor outcomes in patients with low vitamin D are not secondary to pre-existing comorbidity. Rather, vitamin D appears to be an independent factor, possibly relating to its role in host immunity [Hewison, 2012]. The only other independent predictor of poor outcome in this study was advanced age (>70 years old).
One of the limitations of this study is its relatively small sample size. In addition, patients were considered resolved based on their history obtained via a telephone survey, and no follow-up stool studies were performed. Another limitation is the high mortality rate in this cohort of hospitalized patients with multiple comorbidities. As the study interval was only 30 days, long-term antibiotic usage was not tracked. In addition, the number of patients on immunosuppressant drugs was too small to be included in this study. Furthermore, we categorized patients who died as nonresolution. This may have led to an overestimation of failure to resolve C. difficile as the exact cause of mortality in each patient is unknown. In fact, high all-cause mortality in hospitalized patients with low vitamin D levels have already been reported, and are likely due to factors other than the effects of low vitamin D levels on CDAD [Melamed et al. 2008]. Nevertheless, our data adds to a growing literature of the adverse outcomes of hypovitaminosis D in hospitalized patients with serious illnesses such as CDAD.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.