
Abstract
It is a strong and commonly held belief among nutrition clinicians that enteral nutrition is preferable to parenteral nutrition. We provide a narrative review of more recent studies and technical reviews comparing enteral nutrition with parenteral nutrition. Despite significant weaknesses in the existing data, current literature continues to support the use of enteral nutrition in patients requiring nutrition support, over parenteral nutrition.
Introduction
There is a strong consensus and a belief that a lack of controversy exists when comparing enteral nutrition (EN) with parenteral nutrition (PN), and most experts will report that EN is always preferred to PN. Our understanding of the causes of malnutrition and the role of artificial nutrition in patients with ongoing illness, as quite distinct from normal controls, has been evolving for more than 50 years [White et al. 2012]. But decisions about when to feed, how much to feed, and what to feed the undernourished ill are still primarily driven by guidelines based on observational data and expert opinion. Further, relatively few physicians involved in the decision making related to the provision of nutrition support have either advanced training or are up to date on current thinking and research in nutrition support. This results in the persistence of disproven and sometimes deleterious practices, such as favoring PN because of the ease with which it can now be provided.
This narrative review seeks to provide an objective overview of the data. The reader is cautioned that the authors hold strongly to the belief in the superiority of EN over PN. But we also recognize that the absence of very well designed, adequately powered, prospective, randomized, controlled studies, as well as significant changes in clinical practices related to and improving the safety of providing EN and PN, make possible the reversal of this fervently held opinion in the future. In the recent Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition guidelines for nutrition support of the critically ill, for example, 85% of the guidelines were level C or below [McClave et al. 2009].
Because safety, delivery methods, indications, and calorie calculations have changed so drastically over the past decades for both EN and PN [Casaer et al. 2011; Ho et al. 2006; Poulard et al. 2010; Slagt et al. 2004], we have elected to focus more heavily on recent studies. Pancreatitis, surgery, and critical illness are reviewed since most recent studies focus on these patient populations. Certain studies are discussed to illustrate the flaws within them, and the difficulty interpreting the available data. Our searches included PubMed, the Cochrane Library, and our personal files, as well as using references found in review articles to construct this review.
Theoretical and basic science considerations
Proponents for the use of PN will point out that EN delivers calories much less reliably than PN, suggesting this is deleterious. There is no question that chronic starvation will cause harm. But there have been consistently better outcomes in the patients who receive EN (Table 1).
Examples of theoretical reasons for benefits of enteral nutrition.
There are a large number of animal studies demonstrating physiological differences between animals receiving EN versus PN. These have led to the conclusion that food in the gut has an important role in preserving normal physiology, especially that related to immune function and systemic inflammation. It is postulated that PN is less favorable because patients not only lack the benefits from food in the gut, but that PN may also induce deleterious changes in physiology. Research in this area has elucidated a number of important pathways in immunology and systemic inflammation. As a result, there is growing evidence that septic shock syndrome may not be due to bacteremia, but rather due to an interaction between activated pathogenic microorganisms in the gut and the mucosal cells to which they bind. These cells in turn secrete the inflammatory mediators responsible for the syndrome [Alverdy et al. 2003]. Some other interesting examples of animal studies follow.
Kudsk and colleagues provide data that mice have a significant decrease in production of pulmonary immunoglobulin A when on PN versus EN. Further, mice immunized against influenza and placed on PN have a 60% rate of viremia when exposed to influenza virus. Immunized mice, initially on PN and then returned to oral diet, had zero viremia on exposure [Kudsk et al. 1996]. Human clinical data suggested that there is a protective effect on the lung when patients receive EN, compared with nothing, early after surgery. In some reviews of studies of early postoperative feeding, there is a trend toward a reduction in pneumonia despite a concurrent trend toward an increase in vomiting [Lewis et al. 2001].
Omata and colleagues showed that mice on PN had fewer hepatic mononuclear cells, decreased expression of lipopolysaccharide receptors, and decreased survival after intraperitoneal injection of Pseudomonas. Resumption of an oral diet reversed both the immune alterations and the decrease in survival [Omata et al. 2009].
In an experimental burn model in guinea pigs, Saito and colleagues found that those fed enterally had better nitrogen balance and preservation of weight, lower plasma stress hormone levels, and greater mucosal weight and thickness [Saito et al. 1987]. Human studies have shown a reduction in jejunal villous height in normal volunteers placed on PN and nil by mouth for 2 weeks [Buchman et al. 1995]. In a study of critically ill patients, intestinal mucosa was atrophic and leakier than in normal volunteers after 4 days without nourishment [Hernandez et al. 1999]. Mucosal leakage of bacterial antigens has been examined as a cause for hepatic fibrosis in hepatic cirrhosis, for the increased inflammatory state in the obese, and as an alternative to the mucosal adherence theory of septic shock syndrome mentioned above.
Scientific constraints
The meaningful comparison of EN and PN is difficult. There are physiological differences between enteral and parenteral delivery of nutrients for which control is challenging. It is virtually impossible to blind a nutrition support study. Appropriate nutritional clinical outcomes are mortality, morbidity/quality of life, and cost of care [Koretz, 2005; Seres, 2005], which require large studies for adequate power. Easy to measure surrogates, such as serum proteins and anthropometrics, are no longer considered reliable indicators of adequacy of nourishment in the ill. These surrogates are excellent predictors of outcome. However, systemic inflammation rather than artificial nourishment is the major determinate of changes in these surrogates [Koretz, 2005; Seres, 2005].
For one therapy to be considered more ‘beneficial’ than another, it must be first established that one or the other has benefit compared with no intervention. Otherwise, findings of differences may only indicate that one intervention is less detrimental than the other. Nutrition outcomes studies are notoriously difficult to perform; there are no expensive drugs creating funding pathways, and as mentioned, the numbers of patients required to adequately power studies of outcome differences is quite large. The result is a large number of low-quality underpowered studies. Further, institutional review boards are loath to allow continued lack of nourishment in patients with preexisting malnutrition. Therefore, most studies comparing artificial nutrition with no intervention, the only true controlled trial, exclude patients most likely to benefit: those with malnutrition. In the aggregate, and using strict evidence-based analysis, we have yet to truly prove when it is that artificial nutrition has clinical outcomes benefits over no intervention [Koretz et al. 2001, 2007].
The assertion that EN is ‘safer’ than PN requires data on the complication rates associated with both intravenous catheter as well as feeding device insertion. In an earlier analysis, Lipman commented that there are multiple potential complications resulting from placement of access for EN, including nasopulmonary intubation, esophageal stricture and perforation, intestinal obstruction or perforation, abdominal wall migration of tubes, and bowel necrosis and death associated with surgical jejunostomies [Lipman, 1988]. He concluded that, in the absence of documented evidence demonstrating lower EN complication rates compared with PN, EN cannot be said to be safer than PN [Lipman, 1998]. In a subsequent review, McClave and Chang reported that the overall complication rate for percutaneous endoscopic gastrostomy tube placement ranged from 4.9% to 10.8%, but complications were more common in patients who had malnutrition or advanced cancer [McClave and Chang, 2003]. These complications may be infrequent and not lead to high mortality, but without comparison data, the possibility that their morbidity may exceed that of central catheters and PN must be considered. Lipman observed that there were no deaths from catheter infections, but severe morbidity from enterostomy insertion in his institution [Lipman, 1998]. Further, there are no recent data, as far as the authors are aware, that reevaluates complication rates from these procedures.
EN is variably defined, but in general, it provides nourishment into the gut, and may include diet, oral supplementation, and feeding via a tube. For this analysis, the studies reported include patients being fed by tube, except when noted otherwise.
PN includes nourishment by central and peripheral veins. Only studies providing PN via a central venous catheter (central PN or CPN) were included. The terminology ‘total’ PN (TPN) is often used to connote CPN, but this can be misleading. PN provided by a peripheral vein, so called peripheral PN (PPN), can provide total nutrient needs if the patient can tolerate the volume required. Since the route, and not the adequacy of nourishment, was the defining quality for inclusion of studies in this report, all PN referred to is CPN. Studies using PPN are unusual and none were recent or deemed of the required quality for inclusion.
Enteral nutrition and parenteral nutrition: recent developments
There have been significant improvements in the care of patients receiving EN and PN. New analyses are required to understand the impact of these on complication rates in both PN and EN. Safe practice guidelines for PN have been published [Mirtallo et al. 2004], but adherence is poor [Boullata et al. 2012; Seres et al. 2006]. Safety interventions have resulted in significantly reduced infection rates for central venous catheters [Pronovost, 2008], and the acceptable rate is now zero in hospitalized patients [Kuhn, 2008]. This might, in theory, improve the safety of PN, since an increase in infections in patients receiving PN is the most common difference cited between PN and EN [Klein and Koretz, 1994; Lipman, 1998]. Conversely, Casaer and colleagues have recently published a large, randomized multicenter study in which early initiation of PN was compared with delayed (1 week) initiation when EN was insufficient in critically ill patients [Casaer et al. 2011]. They report a 6.3% likelihood of earlier discharge from the ICU [hazard ratio 1.06; 95% confidence interval (CI) 1.00–1.13; p = 0.04] and from the hospital (hazard ratio 1.06; 95% CI 1.00–1.13; p = 0.04), with fewer infections in the late-initiation group (22.8% versus 26.2%, p = 0.008), 3 days less dialysis (p = 0.008), and a reduced cost for the hospitalization of approximately US$1600 (p = 0.04)[Casaer et al. 2011].
However, improvements in safety and conditions in which use of EN is accepted, as well as improved ease of access, have significantly broadened the definition of a ‘functioning gut’ into which EN can be infused. Protocols are being refined to improve safety and tolerance [Heyland et al. 2002]. Small bowel access for patients with gastric dysfunction may now be performed blindly at the bedside [Slagt et al. 2004]. Endoscopic placement of percutaneous jejunostomies, percutaneous dual tube gastrojejunostomies, and nasojejunal tubes has become commonplace with good safety records [Freeman and Delegge, 2009]. Dual port nasogastrojejunal tubes, which drain the stomach and feed into the jejunum, are an option for patients with pancreatitis and duodenal obstruction due to compression from a phlegmon [O’Keefe et al. 2012] or with other types of gastric dysfunction.
Jejunal feeding, which had initially been thought to reduce aspiration, is likely not necessary in many critically ill patients [Ho et al. 2006], making enteral access much easier. Vomiting and aspiration have long been a concern, without foundation in data, for tube-fed critically ill patients. Significantly higher gastric residual volumes (GRVs) are now accepted [Montejo et al. 2010]. Some authors have recommended against their use entirely. Poulard and colleagues found similar outcomes and higher feed volume delivery when they compared patients before (n = 102) and after (n = 103) they ceased checking GRVs in mechanically ventilated patients in a mixed medical–surgical intensive care unit (ICU) [Poulard et al. 2010]. Intolerance (high GRV and vomiting in control group, vomiting in intervention group) was much lower once GRVs were no longer checked (26% post versus 46% pre, p = 0.004). The rate of vomiting alone was no different in the two groups (26% post versus 25% pre, p = 0.34). Ventilator-associated pneumonia occurred with the same frequency in the two groups (18% post versus 20% pre, p = 0.86). There was also a significantly larger volume of feeding delivered to the patients after GRV testing was stopped [1489 ml, interquartile range (IQR) 1349–1647 post versus 1381, IQR 1151–1591 pre; p = 0.002) [Poulard et al. 2010]. It should be noted that the rates of both vomiting and pneumonia in these patients are quite high relative to our experience.
Other conditions, which were traditional indications for PN, have been reported to be amenable to EN. For example, anastomotic leaks with severe intraperitoneal sepsis have now been successfully treated with stents and an oral diet resumed shortly after [Babor et al. 2009]. Others have reported successful management of patients with anastomotic leaks after gastrectomy for cancer using feeding via fluoroscopically placed nasointestinal tube [Akashi et al. 2012]. There have been several reports of select patients with chyle leak being managed with EN [Smoke and Delegge, 2008]. Further, it has been suggested that for patients with chyle leaks, low long-chain fat nutrition is attempted first and then PN started if the leak fails to close [de Gier et al. 1996]. However, there are too few patients reported to analyze outcomes in these patients [Smoke and Delegge, 2008].
Enteral nutrition versus parenteral nutrition in pancreatitis
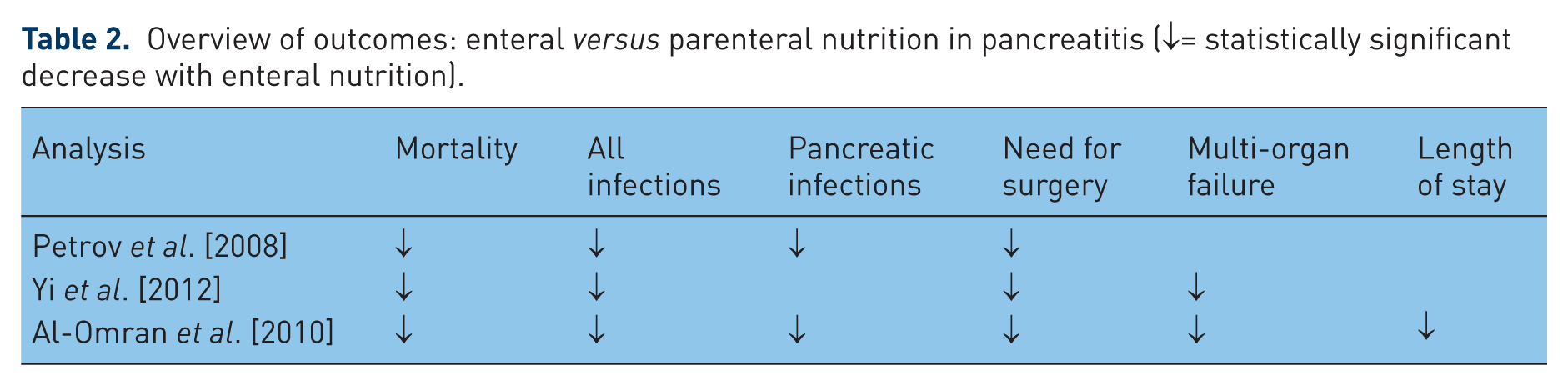
EN has been favored for some time for patients with pancreatitis requiring some form of nutrition support. Four systematic reviews with meta-analyses of randomized trials comparing EN with PN in patients with pancreatitis have been published since 2008. All find in favor of EN [Al-Omran et al. 2010; Petrov et al. 2008; Petrov and Whelan, 2010; Yi et al. 2012]. Three focus solely on severe acute pancreatitis [Petrov et al. 2008; Petrov and Whelan, 2010; Yi et al. 2012], and the fourth, from the Cochrane Collaborative by Al-Omran, on pancreatitis in general [Al-Omran et al. 2010]. Two of the reports on severe pancreatitis, each with five studies included, had the same first author, Petrov, and differed by one paper, but had different focuses [Petrov et al. 2008; Petrov and Whelan, 2010]. The more recent analysis by Yi and colleagues included eight studies, and added two more recent studies not included in either Petrov analysis [Yi et al. 2012]. The Cochrane analysis [Al-Omran et al. 2010] also included eight studies, but only five were common to the prior analyses. All of the 11 evaluated studies were technically flawed (Table 2).
Overview of outcomes: enteral versus parenteral nutrition in pancreatitis (↓= statistically significant decrease with enteral nutrition).
In the first Petrov analysis (EN = 95 patients, PN = 107), the authors report statistically significantly fewer infectious complications in EN patients [22% versus 43%; relative risk (RR) 0.47; 95% CI 0.28–0.77; p < 0.001], pancreatic infections (RR 0.48; 95% CI 0.26–0.91; p = 0.02), need for surgery (RR 0.37; 95% CI 0.21–0.65; p = 0.001), and mortality (4% versus 16%; RR 0.32; 95% CI 0.11–0.98; p = 0.03)[Petrov et al. 2008]. In his second analysis, which included 92 patients receiving PN and 82 on EN, Petrov focused only on complications attributable to each nutrition modality [Petrov and Whelan, 2010]. In that report, patients receiving EN had more diarrhea [23% versus 7%; odds ratio (OR) 0.2; 95% CI 0.09–0.43; p < 0.001], patients receiving PN had more hyperglycemia (23% versus 11%; OR 2.59; 95% CI 1.13–5.94; p = 0.03), but no outcomes were reported [Petrov and Whelan, 2010].
In the subsequent analysis, Yi and colleagues included a significantly larger patient pool (184 EN, 197 PN), and found patients receiving EN to have markedly lower mortality (8.2% versus 24.3%; p = 0.001), infectious complications (26% versus 56%; p = 0.02), organ failure (16% versus 47%; p = 0.02), and need for surgery (19% versus 53%; p = 0.003) [Yi et al. 2012].
Finally, Al-Omran and colleagues found a marked reduction in death in a total of 348 subjects (RR 0.50; 95% CI 0.28–0.91), multiple organ failure (RR 0.55; 95% CI 0.37–0.81), systemic infection (RR 0.39; 95% CI 0.23–0.65), need for surgery (RR 0.44; 95% CI 0.29–0.67), local septic complications (RR 0.74; 95% CI 0.40–1.35), and length of stay (reduced by 2.37 days; 95% CI −7.18 to 2.44) for patients receiving EN. In a subgroup analysis of patients with severe pancreatitis, the risk of death (RR 0.18; 95% CI 0.06–0.58) and multiple organ failure (RR 0.46; 95% CI 0.16–1.29) was even more dramatically decreased [Al-Omran et al. 2010].
In summary, the weight of the evidence strongly favors EN over PN for patients with pancreatitis who require artificial nutrition, with less mortality, fewer infections, less need for surgery, a lower incidence of multiple organ failure, and shorter length of stay in patients receiving EN versus those receiving PN.
Enteral nutrition versus parenteral nutrition in surgical patients
After pancreaticoduodenectomy
Because of the high incidence of postoperative gastric dysfunction in patients undergoing pancreaticoduodenectomy (whipple) for cancer of the pancreas, feeding enterostomies are often placed intraoperatively. There are limited data of poor quality to drive recommendations for preemptive tube placement in this population. In a retrospective analysis which included 1873 patients in the California Cancer Registry from 1994 to 2003, Yermilov and colleagues found an association between the severity of the score on a comorbidity index and whether patients received PN [Yermilov et al. 2009]. Patients who received PN (14% of patients) also had a longer length of stay. However, patients who receive PN at the discretion of their clinician (as opposed to via randomization) are usually sicker to begin with, and sicker patients have longer lengths of stay. Similarly, patients in this cohort receiving feeding jejunostomies at the time of surgery were more likely to be sicker or have a more advanced cancer stage. There were 56 patients who had insertion of feeding jejunostomies who then received PN and were excluded in the statistics. This suggests an approximate 11% failure rate for enteral feeding. This would also bring the incidence of patients requiring PN to 17%. It is not reported how many of the 23% of patients who had placement of jejeunostomies at the time of surgery actually required their use. But at worst, if all of the patients who had jejunostomies placed required their use, a maximum of 40% of all patients received nutrition support. At best, only 17% needed nutrition support if none of the jejunostomies were required. Further, the ‘need’ for nutrition support was inversely related to the number of cases done in each institution [Yermilov et al. 2009], suggesting a lack of uniformity of indications for insertion.
In an historical control study, Georgakis and colleagues report the outcomes prior to (n = 25) and after (n = 34) stopping a policy of universal placement of surgical feeding gastrojejunostomies at the time of pancreaticoduodenectomy [Georgakis et al. 2012]. They report no change in outcomes, other than a significant decrease in total complications (56% versus 35%; p = 0.09) and length of stay (14 days versus 11 days; p = 0.09) once all patients stopped automatically receiving the feeding tubes. Further, the need for PN was not different in the two groups. This is an admittedly underpowered study, but speaks to the possibility that insertion of feeding tubes may not be benign, and should not be assumed safe unless studied properly [Georgakis et al. 2012].
In contrast, Liu and colleagues report the results of a prospective randomized clinical trial in which 60 patients were randomized to receive a jejunostomy and early enteral feeding versus PN. Patients received the nutritional modality for a minimum of 6 days. They found no difference in incidence of intra-abdominal infections, liver dysfunction, biliary fistulas, or lung infections between the groups. In enterally fed patients, however, there were significantly fewer patients with upper gastrointestinal hemorrhage (nine PN versus one EN; p = 0.021), delayed gastric emptying (six PN versus zero EN; p = 0.039), and pancreatic fistulas (eight PN versus one EN; p = 0.039). There was no difference in hospital length of stay, and there were no deaths in either group [Liu et al. 2011].
In another small study by Park and colleagues (38 patients randomized), patients were fed either parenterally or enterally via nasojejunal tube beginning on postoperative day 1 and until oral intake was more than 800 kcal. Patients receiving early EN had earlier bowel movements (2.5 days; p = 0.041), were on a regular diet sooner (0.7 days; p = 0.020), and had regained their perioperative weight loss by day 21. Patients who received PN continued to lose weight for 90 days postoperatively [Park et al. 2012].
In the aggregate, there are insufficient data to drive evidence-based recommendations specifically for patients undergoing pancreaticoduodenectomy. There are observational data suggesting that there may be aggregate risk associated with universal placement of feeding enterostomies in all patients undergoing this procedure. In our institution, an attempt was made to find characteristics that would predict which patients would need jejunostomies, but no statistically significant relationships were found (Chabot, 2012, personal communication).
Surgery of the head, neck, and esophagus
In a prospective randomized clinical trial, Ryu and colleagues assigned 81 patients undergoing laryngeal and pharyngeal cancer surgery in Korea to receive either EN via nasogastric tube or PN postoperatively. Only patients who required support for at least 1 week were included in the analysis. Patients receiving EN had a nonsignificant increase in incidence of pneumonia (9.8% versus 0.0%; p = 0.06) but all recovered well. There was one episode of line sepsis in the PN group. Other than cost (estimated savings comparing product and equipment of US$12/day, plus US$20 per insertion; statistical analysis not provided), there were no other significant differences between the groups [Ryu et al. 2009]. In studies such as this, with a small number of patients, short duration of therapy, and relative good health of the patients, it is not unexpected for differences to be undetectable.
In another small study of 30 patients randomized to EN or PN for 7 days after esophagectomy, Seike and colleagues found no difference in leak rate, inflammatory markers, or albumin [Seike et al. 2011]. However, in a larger (154 patients) randomized trial, Fujita and colleagues found a significantly lower rate of total life-threatening complications in those receiving EN via nasojejunal tube (30.6% PN versus 15.7% EN; p = 0.02) [Fujita et al. 2012]. It is not clear how patients were randomized, and the description of the PN is also confusing and may in fact have been peripheral. In addition, a power analysis is not discussed. Regardless, there were trends toward fewer episodes of anastomotic leak (19.3% PN versus 10.5% EN; p = 17) and pneumonia (11.3% PN versus 5.2% EN; p = 0.26). There was also a significant improvement in the ability to complete the clinical management plan in EN patients (63.6% PN versus 77.6% EN; p = 0.03) and a reduction in hospital length of stay (19 days PN versus 16 days EN; p = 0.04) [Fujita et al. 2012].
General surgery
The benefit of EN over PN in general surgery patients has long been recognized. In a 1992 meta-analysis, Moore and colleagues report on 230 patients randomized to EN or PN. There were significantly fewer septic complications in the EN patients (16% EN versus 35% PN; p = 0.01) and significantly more hyperglycemia in the PN patients (p < 0.05) [Moore et al. 1992]. It should be noted that the majority of the patients included in this analysis had never been published in peer-reviewed journals, and it appears that the authors incorporated data from two additional studies into a meta-analysis to allow for data from a multicenter study to have statistically significant results.
In a study by Braga and colleagues, 257 patients were randomized to receive EN or PN postoperatively after undergoing surgery for cancer of the upper gastrointestinal tract, including stomach, pancreas, and esophagus. EN was started 6 h after surgery and PN on postoperative day 1. There were no differences in any outcomes measured, which included many serum markers and clinical complications. There was, however, a fourfold cost for PN compared with EN (US$90.60/day for PN, US$25/day for EN; p < 0.001) [Braga et al. 2001].
In a follow-up study, which may be the best designed study of its kind, with appropriate randomization and power, 317 patients with preexisiting malnutrition (≥10% weight loss) were randomized to EN or PN following gastrointestinal resection for cancer. Surgery included upper and lower gastrointestinal procedures. In the EN group, 34 patients (21%) were intolerant of the goal feed rate, and of these, 14 were switched to PN. Adverse minor events, such as abdominal distention, cramps, diarrhea, and vomiting were significantly higher in the EN group (35% EN versus 14% PN; p < 0.0001). However, there were statistically significant reductions in infectious complications (16% EN versus 27% PN; p = 0.018) and overall complications (34% EN versus 49% PN; p = 0.005) in the EN group [Bozzetti et al. 2001].
In a recent ‘best practice’, structured protocol review, Wheble and colleagues reviewed seven evaluable studies. They report that there were many technical problems with the quality of all of the studies, but at worst early EN after gastrointestinal surgery is a ‘suitable alternative’ to PN, appears to reduce length of hospital stay and time to resumption of normal bowel function relative to PN, and is far less expensive. They conclude that EN ‘should be considered as the preferred method for delivery of postoperative nutrition’ [Wheble et al. 2012].
Trauma
EN, particularly when started early, has long been promoted as the preferred route in patients who have sustained severe trauma and undergo surgery. The trauma group at the University of Washington in Seattle published one of the first randomized trials comparing EN with PN in 1986. They found that average daily calorie intake, nitrogen balance, and complication rates were comparable between the two groups (46 total patients). Both groups had jejunostomy and central venous access placed [Adams et al. 1986]. In 1992, the trauma group at the University of Tennessee, Memphis performed a larger study in which all 98 patients again received jejunostomies during surgery for blunt and penetrating abdominal trauma, regardless of whether they were randomized to EN or PN. Patients randomized to EN had less pneumonia (11.8% EN versus 31% PN; p < 0.02), significantly fewer intraabdominal abscesses (1.9% EN versus 13.3% PN; p < 0.04), a lower incidence of line-related sepsis (1.9% EN versus 13.3% PN; p < 0.05), a decreased rate of infections overall (0.4 infections/patient EN versus 1.2 infections/patient PN; p = 0.03), and fewer infections per infected patient (1.0 EN versus 1.6 PN; p < 0.01) [Kudsk et al. 1992].
More recently, a multicenter (eight centers) group reported on a large retrospective cohort study of patients who sustained severe blunt trauma and compared those receiving EN with those receiving early supplemental PN when intolerant to EN. There was a significantly higher infection rate in the supplemental PN group. The groups, however, were clinically quite different. The group intolerant to EN and receiving early PN were sicker based on having received many more units of blood (2300 ml versus 1500 ml; p < 0.001), having higher abdominal abbreviated injury scores (189 versus 52; p = 0.008), and a greater need for laparotomy (191 versus 56 patients; p = 0.001). Strangely, they also had lower Acute Physiology and Chronic Health Evaluation II scores (28 versus 33; p < 0.001) [Sena et al. 2008]. With this lack of uniformity of the clinical states of the comparison groups, it is likely that selection bias is compounding the outcomes of this observation.
In conclusion, in a variety of groups of surgical patients, EN has been shown to be superior to PN, and should be the first line of intervention when surgical patients require nutrition support. Wholesale concerns about anastomotic leakage due to feeding are unfounded, although surgeon’s discretion may require a tenuous anastomosis to be rested in selected cases. The number of postoperative conditions in which EN has been shown to be preferred is growing, and the data supporting the expanding interest in feeding early are increasing. For example, our Department of Urology is currently conducting a multicenter study of early feeding (as soon as the patient wants to eat, usually within 24 h) versus delayed feeding (after bowel sounds and flatus, usually 3–5 days) after radical cystectomy and ilial conduit [Deibert, 2011].
Critical illness
An excellent systematic review with meta-analysis was performed by Gramlich and colleagues on 13 qualifying studies of mixed critically ill patients. They found a significant decrease in infectious complications in patients receiving EN versus PN (RR 0.64; 95% CI 0.47–0.87; p = 0.004). There was no difference in mortality, days on ventilator, or length of hospital stay. Four of the studies reported decreased cost, but this was not analyzed for statistical significance [Gramlich et al. 2004]. A second analysis that year reviewed five studies in which EN was compared with a combination of EN and PN. PN was added to EN to insure a desired level of calorie delivery, or EN was added to PN to attenuate the perceived deleterious effects of PN. Most of the patients were well nourished. The authors found no difference in infectious complications or hospital stay, and suggest that the addition of PN in this population is unnecessary [Dhaliwal et al. 2004].
Two recent studies have improved our understanding of the utility of these feeding modalities in the ICU. One trial, by Casaer and colleagues, was discussed earlier in this paper. In this study, 2640 patients were randomized to receive either PN within 48 h of ICU admission (early PN), or after 8 days, if EN was not delivering adequate calories. Early EN was started in both groups. In the early PN group, PN provided calories in addition to EN to reach calorie goal within 3 days of ICU admission. To review, there were fewer infections and decreased cholestasis, fewer patients requiring more than 2 days of mechanical ventilation, and fewer days of renal replacement therapy, with reduced overall costs in the patients for whom PN was delayed [Casaer et al. 2011]. In the EDEN trial, patients were randomized within 48 h of ICU admission to receive either low-volume ‘trophic’ enteral feeds or full ‘goal’ feeds for the first week. There were no differences in outcomes between the groups, and the only significant difference was an increase in gastrointestinal intolerance in the early full feed group [National Heart, Lung and Blood Institute Acute Respiratory Distress Syndrome Clinical Trials Network et al. 2012].
In summary, there appears to be evidence that EN is preferred to PN in patients in ICUs, but that achieving goal feed rate, or goal calories, is not urgent, at least for the first week, and may be detrimental if accomplished by addition of PN.
Conclusions
Nutrition support research is often difficult to interpret due to the challenges achieving adequate study size and quality. However, in a variety of patient populations, the preponderance of data supports the benefits of choosing EN over PN when patients require nutrition support (Table 3). Physicians involved in decision making related to nutrition support should be aware of current research and clinical guidelines, and more physicians should seek advanced training in nutrition support.
Common and consistent outcomes: enteral nutrition advantageous compared with parenteral nutrition.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
D. Seres received research grant funding, unrestricted educational grant funding, and honoraria from Abbott Nutrition for work unrelated to this article. The other authors have no conflicts to declare.