
Abstract
Introduction
Many of the gastrointestinal cancers are diagnosed at an advanced stage, necessitating major surgery that is associated with significant morbidity and mortality. The outcome of such cases is suboptimal due to local or distant metastases. Superficial cancers involving the mucosa are unlikely to cause nodal or distant spread and these cases could be managed endoscopically. Endoscopic mucosal resection was pioneered in Japan [Soetikno et al. 2003] for the management of early gastric cancer. This has gained wider acceptance as a therapeutic option for various gastrointestinal lesions around the globe. The indications have expanded to include treatment of Barrett’s dysplasia, oesophageal squamous dysplasia, small bowel and colorectal adenomas and early cancers. Endoscopic mucosal resection (EMR) also has the advantage of providing an accurate local staging of the disease compared with ablative therapies such as argon plasma coagulation (APC), photodynamic therapy or radiofrequency ablation (RFA). However, this technique needs expertise and adequate training is essential to provide a safe and effective procedure.
Morphological classification of superficial neoplasms
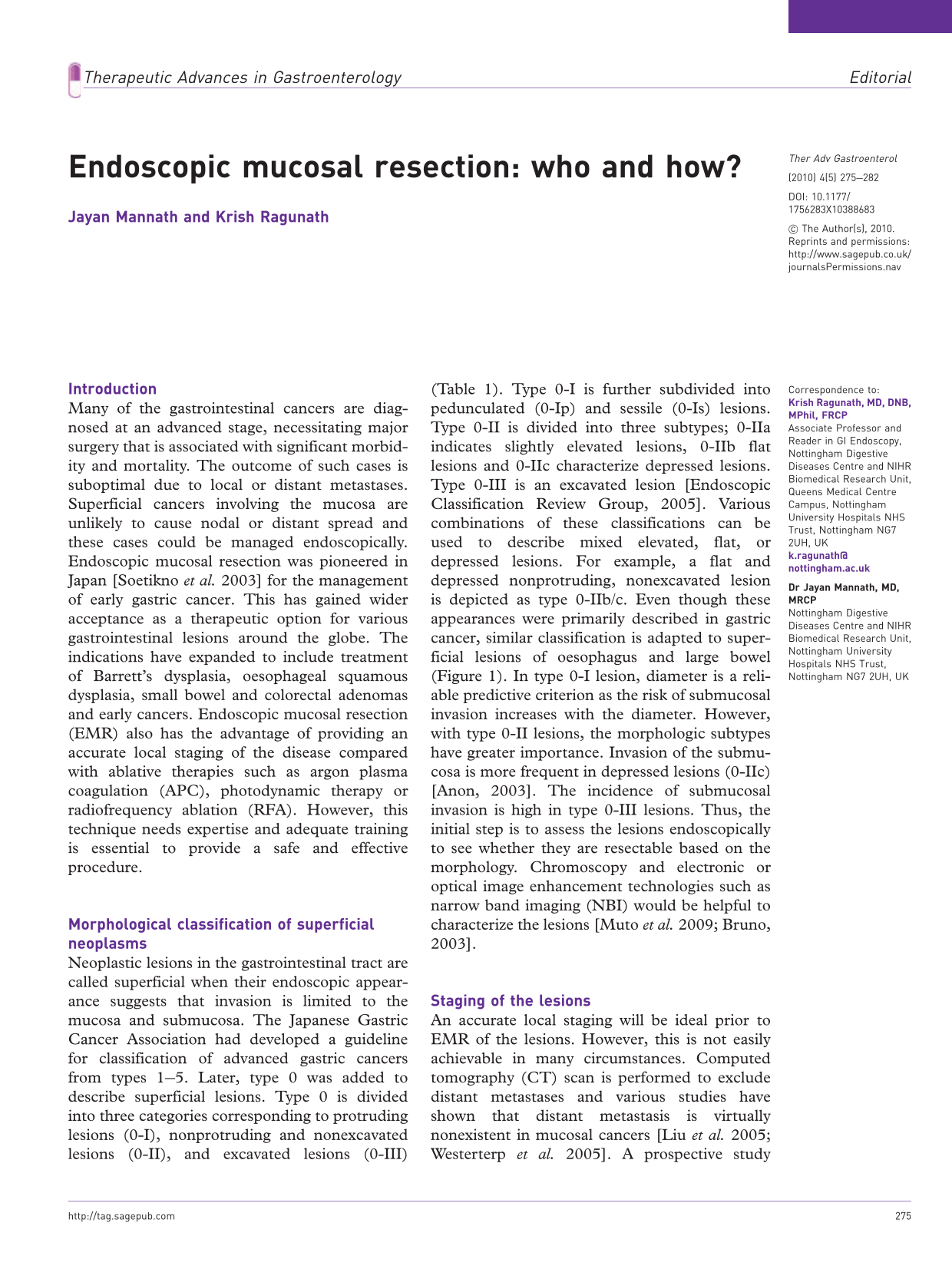
Neoplastic lesions in the gastrointestinal tract are called superficial when their endoscopic appearance suggests that invasion is limited to the mucosa and submucosa. The Japanese Gastric Cancer Association had developed a guideline for classification of advanced gastric cancers from types 1–5. Later, type 0 was added to describe superficial lesions. Type 0 is divided into three categories corresponding to protruding lesions (0-I), nonprotruding and nonexcavated lesions (0-II), and excavated lesions (0-III) (Table 1). Type 0-I is further subdivided into pedunculated (0-Ip) and sessile (0-Is) lesions. Type 0-II is divided into three subtypes; 0-IIa indicates slightly elevated lesions, 0-IIb flat lesions and 0-IIc characterize depressed lesions. Type 0-III is an excavated lesion [Endoscopic Classification Review Group, 2005]. Various combinations of these classifications can be used to describe mixed elevated, flat, or depressed lesions. For example, a flat and depressed nonprotruding, nonexcavated lesion is depicted as type 0-IIb/c. Even though these appearances were primarily described in gastric cancer, similar classification is adapted to superficial lesions of oesophagus and large bowel (Figure 1). In type 0-I lesion, diameter is a reliable predictive criterion as the risk of submucosal invasion increases with the diameter. However, with type 0-II lesions, the morphologic subtypes have greater importance. Invasion of the submucosa is more frequent in depressed lesions (0-IIc) [Anon, 2003]. The incidence of submucosal invasion is high in type 0-III lesions. Thus, the initial step is to assess the lesions endoscopically to see whether they are resectable based on the morphology. Chromoscopy and electronic or optical image enhancement technologies such as narrow band imaging (NBI) would be helpful to characterize the lesions [Muto et al. 2009; Bruno, 2003].
Endoscopic appearance of superficial neoplasms of the gastrointestinal tract; protruding type, pedunculated (0`Ip) and sessile (0-Is); nonprotruding and nonexcavated types, slightly elevated (0-IIa), completely flat (0-IIb) or slightly depressed (0-IIc); excavated type (0-III). (Reproduced with permission from Endoscopic Classification Review Group [2005].) Updated Paris classification of superficial gastrointestinal lesions.

Staging of the lesions
An accurate local staging will be ideal prior to EMR of the lesions. However, this is not easily achievable in many circumstances. Computed tomography (CT) scan is performed to exclude distant metastases and various studies have shown that distant metastasis is virtually nonexistent in mucosal cancers [Liu et al. 2005; Westerterp et al. 2005]. A prospective study in 100 patients with Barrett’s early cancer showed that CT had no influence on the TNM classification [Pech et al. 2006]. However, the risk of metastasis increases with submucosal invasion and in these cases CT is warranted.
Endoscopic ultrasound (EUS) is a very accurate tool for T and N staging of advanced oesophageal cancer. However its value in early neoplasia is questionable. The standard resolution EUS is not sufficient to distinguish superficial mucosal tumours from deep invading tumours [Rosch, 1995]. However, EUS is helpful in N staging and the accuracy is improved significantly (90%) by the addition of fine needle aspiration (FNA) [Klapman et al. 2005]. A retrospective study on the role of high-resolution endoscopy (HRE) and EUS in 50 patients with Barrett’s early neoplasia found that Paris 0-IIa or 0-IIb lesions are associated with mucosal disease (83–100%) as compared with Paris 0-IIc lesions (66%) where the chances of submucosal invasion is more likely [Thomas et al. 2010]. Another prospective study compared HRE with high-resolution EUS in early oesophageal cancers. The results of this study demonstrated that the overall diagnostic accuracy of HRE and high-resolution EUS was high (around 80%), with no significant differences between the two techniques. However, the diagnostic accuracy was not satisfactory, especially in differentiating mucosal from submucosal disease [May et al. 2004]. A mini probe EUS with frequencies up to 20–30 MHz is necessary to differentiate mucosal and submucosal layers and even with this technique the results are not entirely satisfactory. For gastric carcinomas, the accuracy of detecting sm1 invasion was 65–79% [Ohashi et al. 1999; Yanai et al. 1997].
Histological assessment
One of the most important predictors of lymph node metastasis is the depth of infiltration of the lesion. Mucosal lesions are subdivided into T1m1, where the disease is limited to the superficial epithelial layer, T1m2 where the disease involves the lamina propria and T1m3 that extends and involves the muscularis mucosa. The submucosal involvement is similarly subdivided into T1sm1, T1sm2 and T1sm3 as evidenced by involvement of the superficial third, middle third and deepest third of the submucosa. The incidence of lymph node metastasis is negligible in mucosal involvement (T1m1–m3) and therefore these lesions are amenable to endoscopic curative management, whereas those with submucosal involvement raises the possibility of lymph node involvement, ranging from 0-8% in T1sm1 to 26–67% in T1sm2–3 lesions [Liu et al. 2005; Westerterp et al. 2005]. Therefore, deep submucosal invasion is considered as a definite indication for surgery and EMR helps in accurate local staging.
Techniques of endoscopic mucosal resection
The EMR techniques can be broadly divided into suck and cut (suction) or lift and cut (nonsuction) techniques. However in certain cases both techniques are used together. In the lift and cut technique, a submucosal injection is used to separate the muscularis propria from the lesion and this will reduce the chances of perforation. In cases of invasive lesions, a nonlifting sign appears which clearly gives the indication to the operator about the possibility of deeper invasion of the lesion and thus the unsuitability of performing EMR. Colonic EMR is often performed by a nonsuction method and a snare is used to resect the polyp after submucosal injection.
Various solutions are used for submucosal injection. Normal saline is the most widely used agent, but it is absorbed quickly. To overcome this, other agents such as hypertonic saline, 50% dextrose, sodium hyaluronate, 4% succinylated gelatine, etc., are often used [Fujishiro et al. 2004]. Injections are performed using an injection needle at one or multiple sites around the lesion. Recently, a needleless injection using an automated pump has been made commercially available (ERBE, Germany).
The suction technique using a multiband mucosectomy (MBM) device (Cook Medical, Ireland) is commonly used in Barrett’s dysplasia and this technique does not need submucosal injection [Peters et al. 2007]. A pseudopolyp is formed by band ligation, which is then resected with a snare. However, in cases of the EMR cap technique (Olympus, Japan), submucosal injection is used and the lesion is sucked into the cap and resected using a prelooped snare [Gotoda, 2007; Inoue et al. 1993].
Indications for curative endoscopic mucosal resection in early gastrointestinal cancers.

Oesophagus
Barrett’s oesophagus
EMR could be offered as a therapeutic option in patients presenting with focal high-grade dysplasia (HGD) and mucosal cancer. Those with submucosal invasion, vascular or lymphatic invasion should be referred for oesophagectomy. However, low-risk submucosal invasion (T1sm1) is considered to be appropriate for endotherapy in certain centres [Manner et al. 2008]. This needs to be tailored according to the local guidelines and multidisciplinary opinion. EMR is considered to be therapeutic and curative when R0 resection is achieved. A complete resection of lateral margins is histologically difficult to assess, especially in cases of piecemeal resection. This is usually achieved by marking the dysplastic area using APC probe or the tip of the snare prior to resection and making sure that all of the marked areas are included in the resection. Follow-up endoscopies are performed to closely examine the edges of the previously resected area to exclude residual dysplasia.
A large series published by the Wiesbaden group showed a complete remission of Barrett’s cancer in 95% of patients treated with EMR alone at 5-year follow up. A significant proportion of patients (20%) developed metachronous lesions during follow up, which were all managed endoscopically. The calculated 5-year survival rate was 84% [Pech et al. 2008]. Stepwise radical endoscopic resection (SRER) to remove the entire segment of dysplastic Barrett’s was reported in another study. In 169 patients treated, complete eradication of neoplasia and intestinal metaplasia was achieved in 95% and 80%, respectively, at a median follow up of 32 months. However, a significant proportion of patients (50%) developed dysphagia secondary to stricture [Pouw et al. 2010]. Considering the higher rate of complications, SRER could not be recommended in all patients, except in those with short segment dysplastic Barrett’s oesophagus. EMR of Barrett’s dysplasia could be performed using an EMR-cap technique or MBM device (Figure 2).
Endoscopic mucosal resection of Barrett’s early cancer. A Paris 0-IIa/c lesion is seen extending between 4 o’clock to 10 o’clock (a). The neoplastic area is marked using the tip of a snare (b). A piecemeal endoscopic resection is performed by multiband mucosectomy device (suck and ligate) technique (c). The resected area is seen clear of all initial markings (d). The specimens are pinned down to a cork for histopathological assessment (e).
Squamous dysplasia and cancer
Oesophageal squamous dysplasia and cancer are reported to show synchronous and metachronous lesions [Urabe et al. 2009]. Early lesions limited to the mucosa are amenable for endoscopic resection and studies have shown a 5-year survival rate of up to 95% [Inoue, 1998; Takeshita et al. 1997]. The incidence of lymph node metastases is negligible in m1 and m2 mucosal cancers and EMR is usually recommended for squamous cell carcinoma of the oesophagus confined to the lamina propria. An earlier prospective study compared the outcome of patients with muscularis mucosal and superficial submucosal invasion treated by EMR. The overall 5-year survival rates were no different compared with surgery in 26 patients [Shimizu et al. 2002]. Another study from Europe included 39 patients with superficial squamous cancers and the curative rates following EMR were around 90% [Pech et al. 2004]. A recent study from Japan compared endoscopic submucosal dissection (ESD) with EMR in 168 lesions and found that the curative rates were better with ESD compared with EMR. Nevertheless, the EMR cap technique was associated with 71% curative resections [Ishihara et al. 2008].
As a general rule, oesophageal cancers of diameter less than 2 cm, those involving less than one third of the circumference of the oesophageal wall and lesions limited to the mucosa of the oesophagus could be managed by EMR with a curative intent.
Stomach
EMR is widely used for treatment of early gastric cancer (EGC) in Japan as an alternative to surgery. The primary characteristics of EGC that are amenable to EMR include elevated lesions less than 2 cm in size, depressed lesions less than 1 cm in size without ulceration, well or moderately differentiated adenocarcinoma of intestinal type and absence of lymph node metastasis on pretreatment staging studies. ESD is a novel technique that has been introduced as a means to extend endoscopists’ capabilities to resect larger tumours and obtain more reliable pathologic specimens [Gotoda et al. 2006]. Various types of endoscopic electrosurgical knives are used to incise and remove large neoplastic lesions en bloc by this technique. A meta-analysis of 15 studies found that ESD, compared with EMR, had higher en bloc and curative resections rates (OR 13.9 and 3.5, respectively), as well as lower rates of local recurrence (OR 0.09) [Cao et al. 2009]. The risk of lymph node metastasis is about 0.4% for differentiated cancers. Undifferentiated mucosal cancers should not be treated by EMR, as the risk of lymph node metastasis rises to 4% [Conio et al. 2006]. In one series of 308 patients, EMR successfully eradicated the cancer in 85% of cases. The complete endoscopic resection rate was lower in type 0-IIa lesions larger than 2 cm and with type 0-IIc lesions that were either larger than 1 cm or associated with undifferentiated adenocarcinoma. Commendably, the 5-year survival was 86%, a rate which is similar to results reported with aggressive surgical approaches [Takekoshi et al. 1994]. In patients with small and differentiated mucosal gastric cancers, excellent prognosis was noted with en bloc EMR. In 131 patients, the disease specific 10-year survival was 99% and overall survival rates of 64% [Uedo et al. 2006]. A smaller study from the West included 39 patients with well or moderately differentiated EGC less than 3 cm in size, who underwent EMR, showed no tumour-related deaths during a mean 5-year follow up. However, there was major complications in 15% cases which were all managed endoscopically [Manner et al. 2009].
Duodenum
EMR could be used to remove peri-ampullary or duodenal adenomas, neuro-endocrine tumours and subepithelial stromal tumours. Endoscopic snare papillectomy is increasingly performed with curative intent for benign ampullary lesions. A recent study reported on EMR of laterally spreading tumours involving the ampulla. Ten patients underwent a combined EMR and papillectomy and one patient had recurrence at 3 months. Bleeding occurred in 30% cases and cholecystitis in 10% [Hopper et al. 2010]. A single-centre study in 59 patients, who underwent EMR of the nonampullary lesions, showed that successful resection was accomplished in 93% of cases on the initial attempt. However, recurrence was noted in 37% cases. Polyps >2 cm in size were associated with higher rates of adenoma and a higher incidence of recurrence [Abbass et al. 2010]. A recent series including 5-year data on EMR of large nonampullary lesions showed a recurrence rate of 24%, but there were no significant complications [Alexander et al. 2009].
Colorectum
EMR is particularly useful in managing large sessile and flat lesions of colorectum. Polyps greater than 2 cm in size may be resected piecemeal to avoid perforation. However, there are concerns regarding inadequate histological assessment and higher rates of recurrence following piecemeal resections. In 148 cases of large and giant polyps, EMR was performed en bloc in 44% cases and piecemeal in the rest. The recurrence rate was 4.2 % after a mean follow up of 30 months. The incidence of major complications was low in this series [Luigiano et al. 2009]. A second study included 186 endoscopically resected polyps between 3 and 13 cm in maximum diameter. Of 141 sessile polyps excised, two patients required surgery for procedural bleeding and one for delayed perforation in the caecum. During a mean follow up of 40 months, benign recurrences were observed in only 3% of patients [Doniec et al. 2003]. A recent meta-analysis which included 25 studies, however, showed lower pooled rates of complete curative en bloc resections at 59% [Puli et al. 2009]. Our experience (unpublished data) suggests that the incidence of polyp recurrence after en bloc resection is 60% less compared with piecemeal resection and additional use of APC did not improve the recurrence rates. However, an earlier randomized trial showed that polyp recurrence after complete piecemeal resection of large polyps is reduced significantly with the use of APC. In cases of incomplete resection, APC did not show any significant advantage [Brooker et al. 2002].
Complications
Bleeding and perforation are the major complications associated with EMR. In cases of oesophageal EMR, no difference in complications was observed when the EMR cap technique is compared with the ligation and cut technique. In 100 cases of EMR, only two patients developed minor bleeding and there were no perforations [May et al. 2003]. A circumferential mucosal defect involving over three quarters the circumference of the oesophagus after EMR was significantly associated with the subsequent development of oesophageal stricture [Katada et al. 2003]. Bleeding is the most common complication occurring in up to 7–8% of patients undergoing standard EMR or ESD for EGC. Perforations are uncommon in gastric EMR compared with ESD (4%) [Coda et al. 2007]. High doses of proton pump inhibitors are usually given for 4–8 weeks to facilitate mucosal healing following upper gastrointestinal EMR. Patients are usually allowed only clear fluids for 24 hours, followed by soft diet for 3 days.
Injection of adequate amounts of submucosal fluid is of paramount importance to avoid perforations in the colon, especially in right-sided lesions. A recent series of colonic EMR in 182 lesions showed a perforation rate of 1% and bleeding in 12% cases [Ferrara et al. 2010]. More frequent and minor complications include pain and postpolypectomy syndrome.
Conclusion
EMR is an important advance in the field of therapeutic endoscopy and has already been accepted as a minimally invasive alternative to surgery in mucosal lesions affecting the upper and lower gastrointestinal tract. The largest experience is predominantly from the Japanese endoscopists, but the indications have been expanded to accommodate the predominantly Western diseases such as Barrett’s oesophagus. EUS can be useful to assess the nodal staging of early cancers; however, its role in differentiating mucosal and submucosal cancers is questionable. Endoscopic morphological appearance is a useful guide to assess lesions amenable for EMR. These procedures involve a high risk of complications and should be performed by experienced and trained endoscopists.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.