
Abstract
Abdominal pain is a common reason for patients presenting to primary care and has a wide range of differentials. It can be acute or chronic, with the latter being defined as lasting over 3 months. A myriad of conditions can cause acute abdominal pain, ranging from life-threatening to self-limiting. Common causes of acute abdominal pain include differentials from the gastrointestinal, urological, gynaecological, genitourinary, and vascular systems. This requires clinicians to have a breadth of knowledge to safely manage these patients. The differential diagnoses need to be established through a thorough history and physical examination, ultimately aiding the decision between management in primary versus secondary care. This article will highlight features within the history and examination required to distinguish the causes of acute abdominal pain and some to aid decisions on management, whether in primary care or needing referral to secondary care. The article will provide a brief overview of common causes of acute pain by location in the abdomen.
Clinical case scenario
A 26-year-old man, who previously has been fit and well, presents to the GP with a 2-day history of gradually worsening periumbilical pain that migrated to the right iliac fossa on the morning of presentation. It is debilitating and worsened by movement and coughing. He feels generally unwell and has had episodes of nausea and vomiting along with anorexia. On examination, he is flushed with pyrexia of 38.1°C, tachycardia, blood pressure (BP) 118/72 mm Hg, oxygen saturation of 96%, and respiratory rate of 24/ minute. His abdomen is generally tender, but soft in the right lower quadrant with maximal pain at McBurney’s point. Rosving’s, psoas and obturator signs are also positive. Acute non-perforated appendicitis is suspected and urgent hospital admission arranged. A week later, a discharge letter confirms the clinical diagnosis of appendicitis, with computed tomography (CT) showing inflammation but no perforation. While waiting for theatre, he suddenly deteriorated with worsening abdominal pain and signs of sepsis. Laparotomy revealed a perforated appendix. He makes a good recovery with intravenous antibiotics over the next week.
Pathophysiology of pain
To understand the symptoms of our patients, it is important to understand the physiology involved in the feeling of pain. Pain occurs when a pain signal is transmitted from the periphery to the central nervous system (Steeds, 2016). Pain fibres synapse with neurones from the spinal cord, where reticular tracts convey this message to the brain, which is then processed by the thalamus and communicated to the cortex (Steeds, 2016).
Abdominal pain can be divided into several types, including visceral, somatic, referred, and psychogenic. Visceral pain originates from the abdominal viscera, which is innervated by autonomic nerves that are triggered mainly by inflammation, distention, or muscular contraction. Typically, this pain is dull and poorly localised. Somatic pain is derived from the parietal peritoneum and is innervated by somatic nerves responding to inflammation; bacterial or chemical. This pain is sharp, easily located, and often aggravated by coughing or moving, causing patients to want to lie very still. Referred pain is felt distantly from its source. It is caused by visceral organs sharing pathways with peripheral nerves in the spinal cord. Often, this pain is felt near the surface of the body, with a common example being gallbladder pain referred to the right shoulder (Bates and Plevris, 2013). Different types of pain are shown in Table 1
Different types of pain.
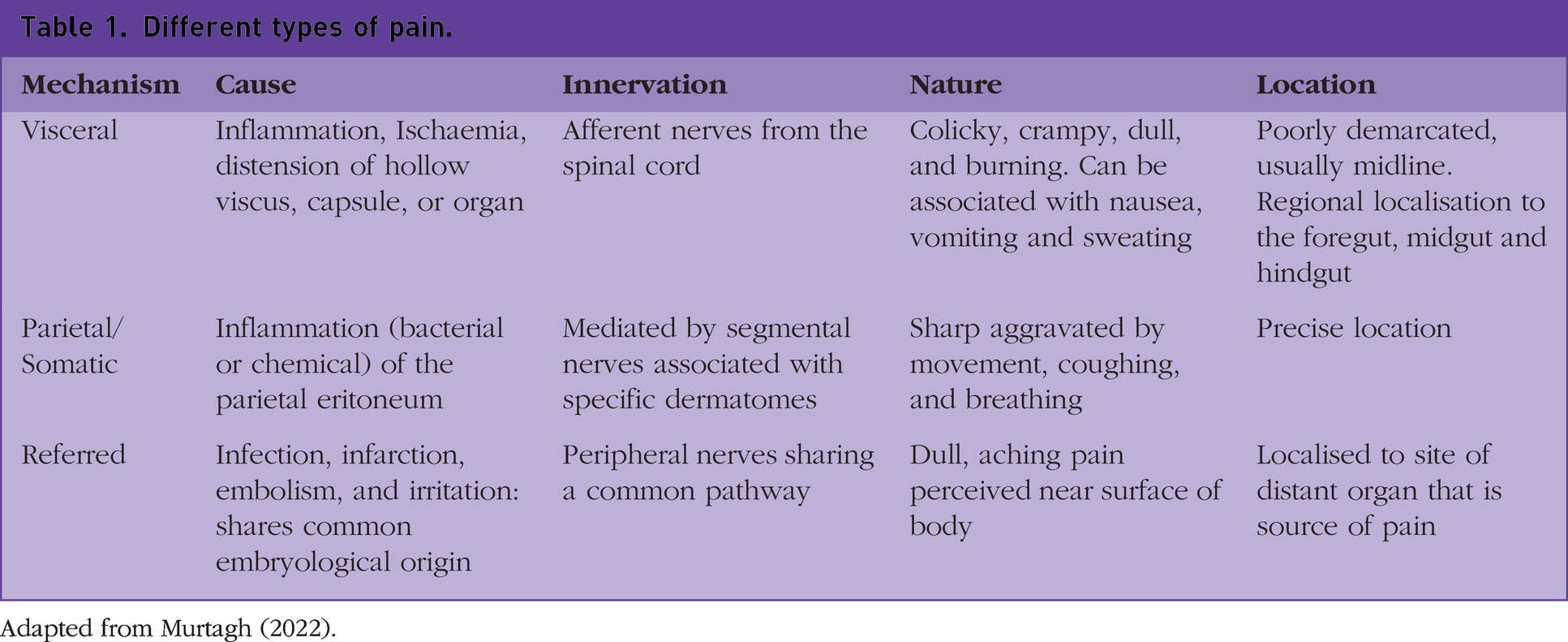
Adapted from Murtagh (2022).
In medicine, we understand that painful stimuli are likely a result of internal or external tissue damage. However, Steeds (2016) argues that pain can be subjective; pain is frequently reported by patients in the absence of any pathophysiological cause, leading to the suspicion of a psychological element. As clinicians, we should always accept that a patient is feeling pain, regardless of a lack of pathophysiological findings (Steeds, 2016). This is particularly important in general practice, where no cause is identified for approximately a third of all patients complaining of abdominal pain, and they are labelled as having 'functional' or non-specific abdominal pain (Price et al., 2022).
Site and characteristics of abdominal pain
The location of abdominal pain typically reflects the anatomical site of the organ or underlying structure. An example is cholecystitis presenting with right upper quadrant (RUQ) pain. As a rule, upper abdominal pain is usually caused by problems in the upper gastrointestinal (GI) tract and lower abdominal pain with the lower GI tract and pelvic organs. However, potentially serious causes, including bowel obstruction, mesenteric ischemia, and a perforated viscus, can be vague and poorly localised. Important ‘extra-abdominal’ pathologies such as acute coronary syndrome and diabetic ketoacidosis also present with abdominal pain, thus requiring good clinical acumen to not miss significant illness. Radiation of pain can suggest certain pathologies, such as pancreatitis radiating to the back and kidney disease radiating to the scrotum. Figure 1 illustrates the causes of abdominal pain by nine regions.
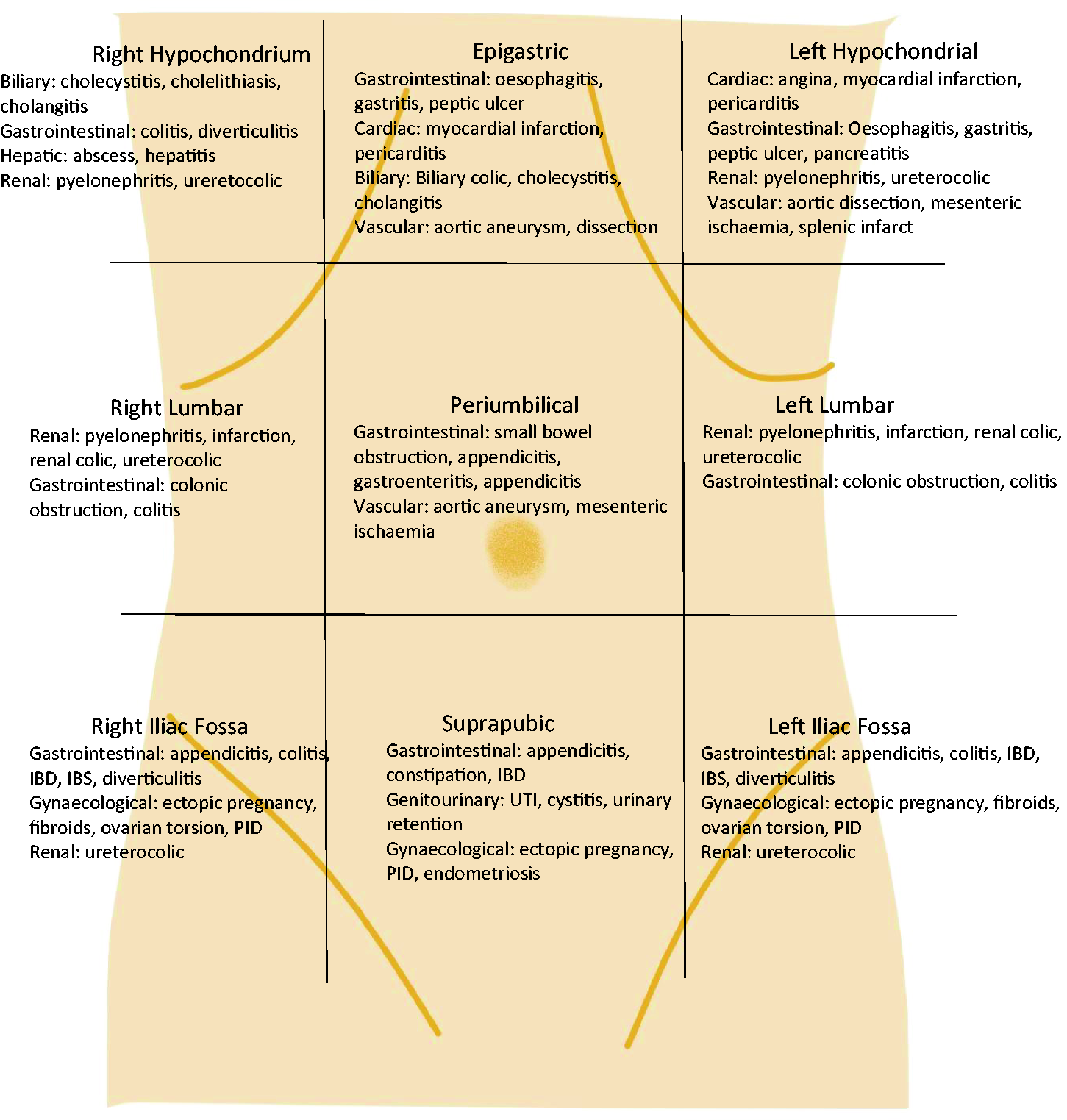
Sites of abdominal pain.
Determining the character of pain is a useful clue, whether it is sharp, dull, or colicky in nature. Sharp pain usually indicates that the parietal peritoneum is irritated, whereas dull pain is typical of visceral pain. Colicky pain is described as sharp pain that peaks and subsides. Location can help determine the cause, with ureteric stones if ‘loin to groin’, biliary colic in RUQ, or periumbilical in small bowel obstruction (SBO).
History
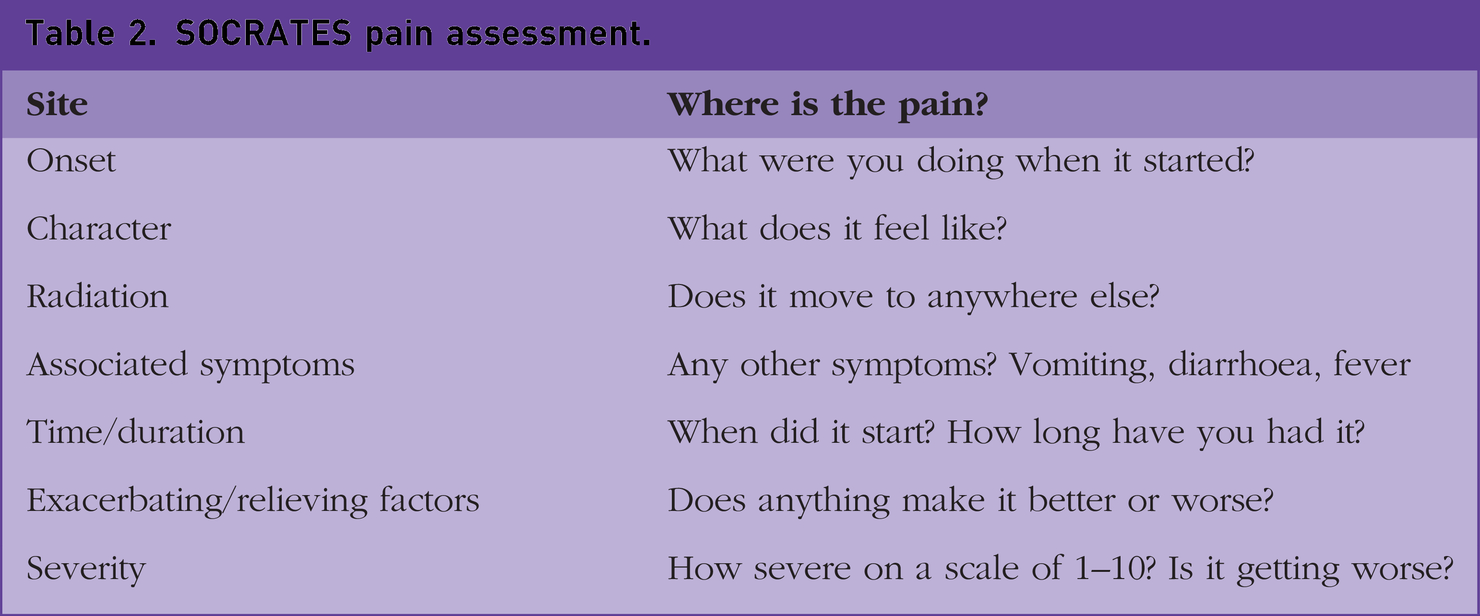
A detailed and thorough history is vital for developing accurate differential diagnoses and excluding red flags that would indicate urgent or immediate referral to secondary care. Important indicators for immediate referral to secondary care include increasing severity of pain, peritonism, vomiting, haemodynamic instability, signs of bowel obstruction, and GI bleeding. Characteristics such as onset and timing of pain are important to establish. Sudden onset is more likely to indicate perforation. Diverticulitis can typically cause persistent pain, whereas intermittent pain can be caused by bowel obstruction. Timing in relation to food intake can be important. For example, mesenteric ischaemia is typically worse after eating, whereas duodenal ulcer pain can be initially relieved before worsening with time. It is also important to determine associated features such as fever and rigors, relation to bowel movements and menstrual cycle. A change in bowel movements such as mucus, blood, diarrhoea, or hard stool can help diagnosis, with failure to pass stool or flatus being an important indicator of obstruction. A history of previous abdominal surgery is a particular risk factor for obstruction from development of adhesions. Anorexia is common among numerous pathologies, with changes in urination, such as pain or colour, being indicators of genitourinary disease. Determination of pregnancy in women is of vital importance, for example to rule out potentially life-threatening ectopic pregnancies. A detailed social history, particularly travel and sexual history, is important for infectious causes. Using mnemonics such as SOCRATES for abdominal pain assessment can be helpful. See Table 2. Important information selected from the history can be seen in Table 3.
SOCRATES pain assessment.
Features of the abdominal pain history.
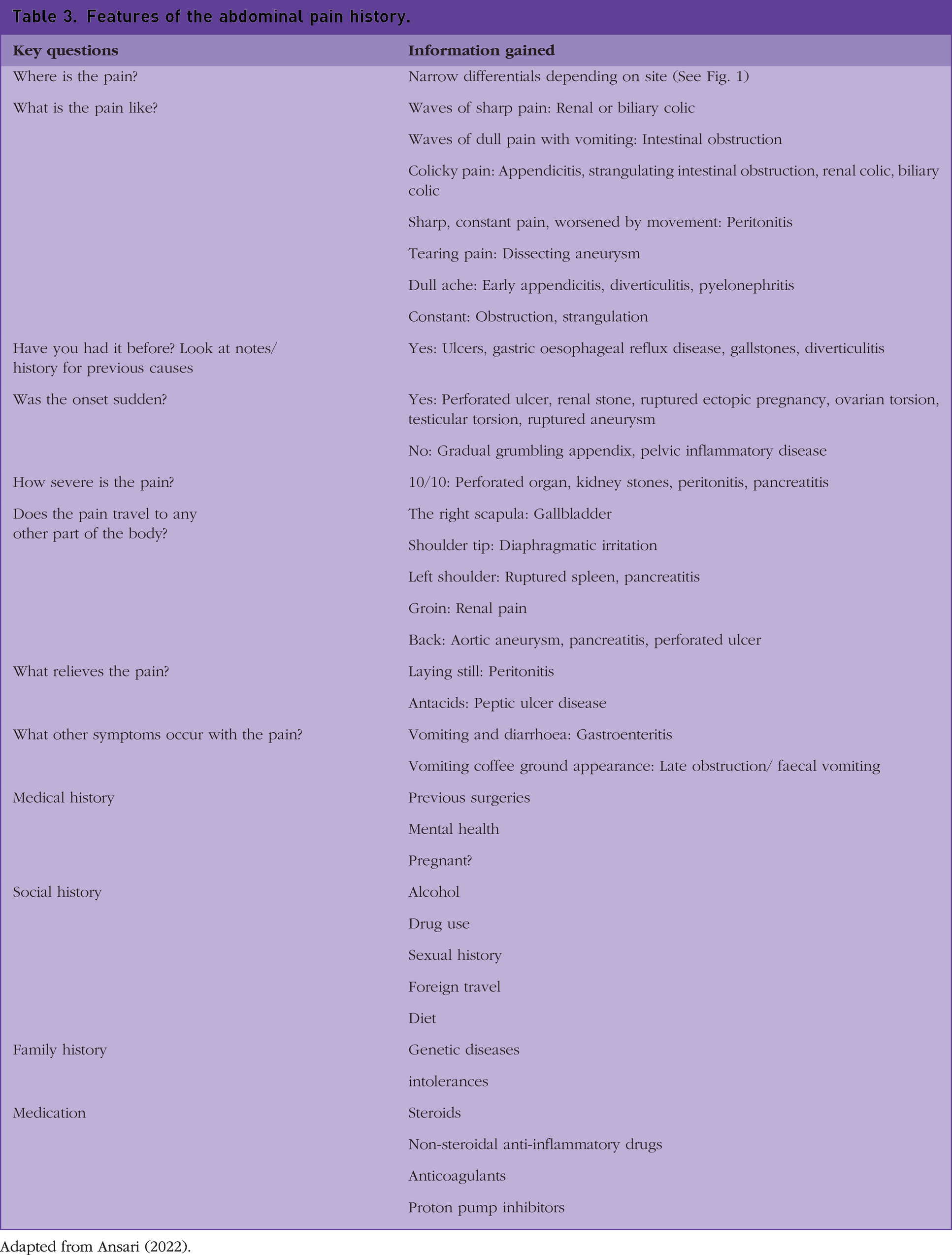
Adapted from Ansari (2022).
Examination
Observing a patient move from the waiting area to your room can be telling. A comfortable, happy patient rarely has a life-threatening problem.
Basic observations should be performed, including blood pressure, temperature, pulse, respiratory rate, and oxygen saturation. A pregnancy test should be performed for all women of childbearing age before referral to secondary care. Clinical examination, including inspection, palpation, percussion, and auscultation, should enable the clinician to confirm or discard the suspected diagnosis made from thorough history taking.
Thorough physical examination of the abdomen will help elicit signs that point towards a diagnosis and the severity of the condition. Abdominal inspection comes first. Abdominal distension can indicate bowel obstruction, hernias, ascites, hepatomegaly, splenomegaly, constipation, or pregnancy. Inspecting for skin changes can reveal certain pathologies, such as bruising in the periumbilical or flank area (Grey Turner’s sign or Cullen’s sign, respectively) indicating haemorrhagic pancreatitis. Careful palpation of the abdomen is essential to determine the location of pain, abdominal masses, and potential irreducible hernias. Palpation is also a sensitive test for peritonitis, which looks for guarding or rebound tenderness. If there is a history of GI bleeding or bowel obstruction, a digital rectal examination should be performed to inspect for blood or faecal material. Percussion can help distinguish between types of abdominal distension, being tympanic for gas or dull with intra-abdominal fluid such as ascites or blood. Finally, the abdomen must be auscultated for at least a minute to gauge the presence and character of any bowel sounds. High-pitched ‘tinkling’ bowel sounds indicate bowel obstruction, whereas the absence of bowel sounds indicates paralytic ileus. Pelvic examination is indicated in women when the pain is in the lower abdomen and can identify pathologies such as ovarian torsion and pelvic inflammatory disease (PID). Examination of the groin can reveal hernias. The scrotum must be examined to exclude testicular torsion and epididymitis, which can often cause abdominal pain.
When to refer to secondary care
It is often the responsibility of the GP to decide whether to treat patients in the community or to refer to secondary care. It is important to identify clinical features that indicate potentially significant and life-threatening pathologies requiring immediate hospital admission, via ambulance if necessary. See Box 1 for red flag findings. There are also some specific conditions that need to be referred to secondary care, even if the patient looks well at the time of consultation. Examples include ectopic pregnancy, appendicitis, pancreatitis, ureteric colic, acute cholecystitis, biliary sepsis, and bowel obstruction. Patients presenting with severe acute abdominal pain of unknown cause, with or without any of the red flag signs, should also be admitted. If history and examination indicate a diagnosis manageable in the community, this can be suggested with appropriate safety netting and medication. Red flag examination findings. Signs of peritonism – rebound tenderness, guarding Signs of sepsis/shock – tachycardia, hypotension, and fever GI haemorrhage Impaired consciousness Abdominal distension Absent bowel sounds Failure to pass flatus
Investigations
Further investigation of abdominal pain in primary care includes blood tests, urine samples, faecal samples, and scans (National Institute for Health and Care Excellence (NICE) 2013; NICE, 2017; Ringel-Kulka and Ringer, 2021). These can be ordered initially in primary care depending on the suspected diagnosis. A broad panel of generic tests, such as full blood count, urea and electrolytes, liver function tests (LFTs) and C-reactive protein, are a useful start. Cultures of urine and stool should be sent if an infectious cause is suspected to aid choice of antibiotic. More specific tests such as a coeliac screen or calprotectin, indicating inflammatory bowel disease, should be sent if indicated (NICE 2021a; Ringel-Kulka and Ringer, 2021). Referring for an ultrasound scan (USS) is appropriate when gynaecological issues are suspected, but it can also be useful in other abdominal pathologies such as hernias (NICE, 2011). Endoscopic procedures are indicated for concerns regarding GI cancer, particularly with concurrent anaemia. Urea breath tests are useful for dyspeptic patients to exclude Helicobacter pylori infection. CT is usually a secondary care investigation and can help distinguish between many GI, urological, gynaecological, and vascular disorders (NICE, 2021b).
With a complete history, thorough examination, and appropriate investigation, a diagnosis can usually be reached. Common differential diagnoses and the respective organ systems are shown in Table 4.
Differentials of abdominal pain.
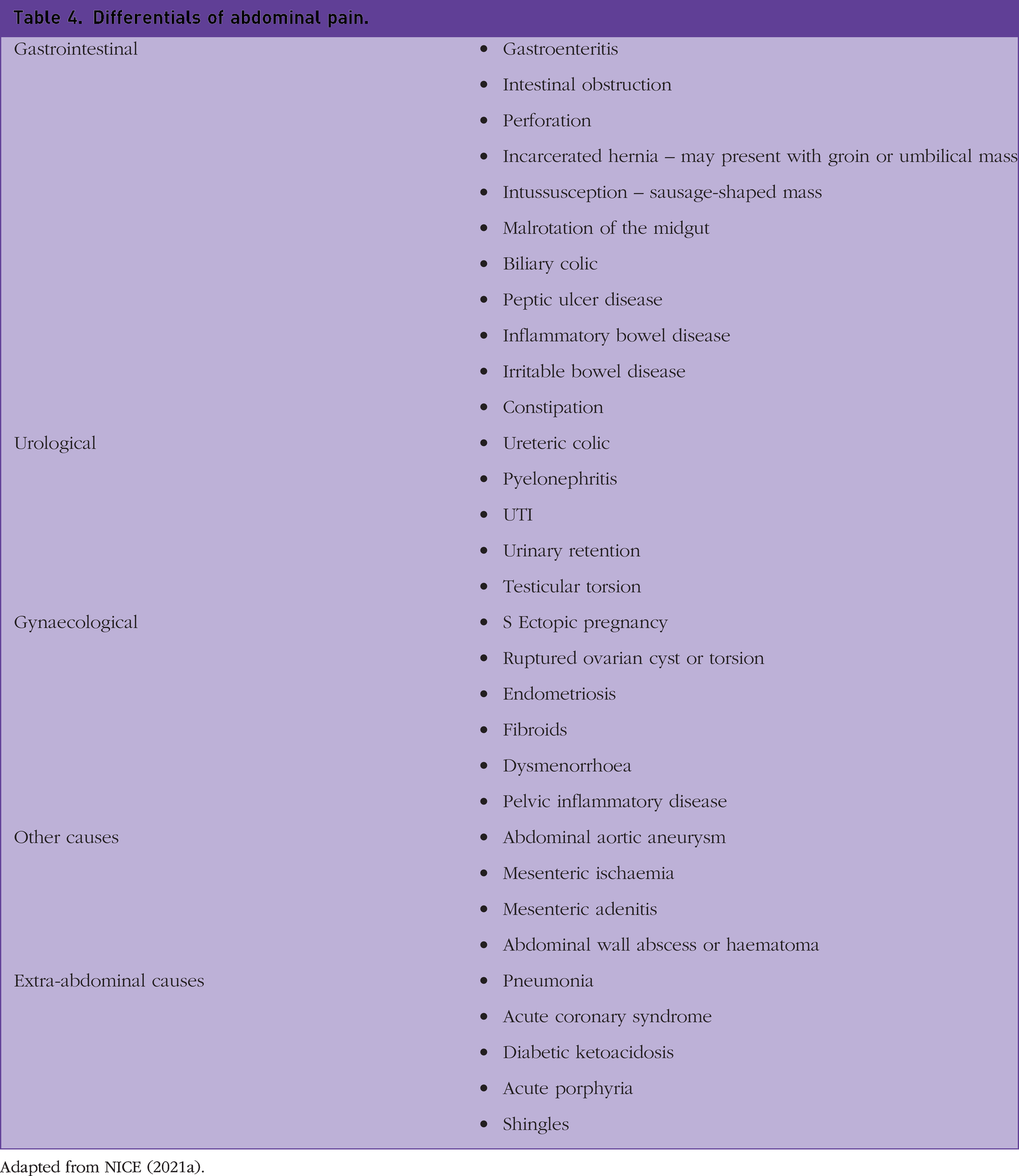
Adapted from NICE (2021a).
Common presentations by location
Epigastric pain
Epigastric pain that comes on suddenly and radiates to the back suggests acute pancreatitis. This pain is usually severe, can worsen on movement or postprandial, and may be relieved once in the foetal position (NICE, 2021c). Accompanying symptoms include nausea and vomiting. A history of alcohol abuse and gallstones are risk factors. Patients should be examined for signs of shock and systemic illness; tachycardia, tachypnoea, fever, and hypotension (NICE, 2021c). Any patient suspected to have acute pancreatitis should be admitted for further management. Further investigations in primary care are not warranted and may delay admission (NICE, 2021).
A history of the use of non-steroidal anti-inflammatory drugs (NSAIDS) or of steroid use to combat epigastric pain, particularly nocturnal and related to meals, points towards peptic ulcer disease. This can usually be managed initially in primary care with proton pump inhibitors, H. Pylori eradication if present and lifestyle advice. However, if there are signs of overt GI haemorrhage then immediate referral to secondary care is appropriate. Sudden onset severe upper abdominal pain with a history of peptic ulcer disease and signs of peritonism should raise the suspicion of perforation and prompt immediate admission for surgical management.
Upper quadrant or hypochondrial pain
Right hypochondrial or RUQ pain is felt in the right upper area of the abdomen and is often caused by biliary tract pathology. Patients presenting with severe postprandial RUQ pain of sudden onset may have biliary colic due to cholelithiasis. This pain may also be associated with nausea and vomiting, anorexia, and fever in the presence of infection indicating cholecystitis. More than 90% of patients with acute cholecystitis have gallstones (NICE, 2021d). Examination should look for signs of sepsis, such as tachycardia (heart rate >100), hypotension (systolic BP <90 mm Hg), rigors, and shortness of breath. On examination, RUQ pain and guarding may be notable, including possible gallbladder distention, which can sometimes be palpable in those with cholecystitis (NICE, 2021d). Murphy’s sign may be elicited with palpation of the liver edge, asking the patient to inhale. The detection of acute pain associated with this indicates cholecystitis.
Another complication of cholelithiasis is acute cholangitis, which typically presents with Charcot’s triad of biliary pain, jaundice and fever. It is also likely to be accompanied by derangement of LFTs and increased inflammatory markers in the presence of infection. Suspicion of cholecystitis or cholangitis warrants referral to a hospital where confirmatory investigations, including an USS, can be performed. Patients often require IV antibiotics, fluid resuscitation and definitive management, including endoscopic retrograde cholangiopancreatography and cholecystectomy. RUQ pain can also be caused by renal and colonic diseases, including malignancy and obstruction.
Causes of left upper quadrant (LUQ) or hypochondrial pain are typically similar to conditions discussed in epigastric and RUQ pain, such as pancreatitis and renal disease. However, disorders of the spleen need to be excluded because they carry a significant morbidity. Splenic infarction typically causes LUQ pain, nausea, vomiting, and fever, whereas splenic rupture following trauma can cause LUQ pain and haemodynamic instability.
Flank/lumbar pain
A common cause of flank pain is renal or ureteric colic (NICE, 2020). Pain often starts in the flank and radiates to the labia in women and the testicles in men. Pain is commonly associated with nausea and vomiting, and a urine dipstick often reveals haematuria (NICE, 2020). Hospital admission should be arranged for those who have signs of sepsis and those who are at a high risk for acute kidney injury; chronic kidney disease, nephrectomy, and transplant patients. Urgent imaging should be performed within 24 hours, which can either be a non-contrast CT scan or USS for pregnant women to confirm diagnosis and exclude hydronephrosis. CT and USS would also detect an abdominal aortic aneurysm, which can mimic renal colic pain. Smaller stones <5 mm with minimal symptoms, a watch and wait approach with analgesia to enable it to pass is common. Severe pain with larger renal or ureteric stones usually warrants expulsive therapy or surgical intervention (NICE, 2019). NSAIDS should be offered as the first line for pain relief unless contraindicated. Ongoing treatment in primary care involves appropriate diet and lifestyle advice to reduce the chances of recurrence. This can include:
Increasing fluid intake, adding lemon to drinking water Avoid carbonated drinks Reduce salt intake Reduce calcium intake Eating a balanced diet and maintaining a healthy weight; a primary care dietician may help with this advice
Infectious causes, including pyelonephritis and psoas abscess, are other causes of flank pain. Pyelonephritis can be a complication of frequent or untreated urinary tract infections and presents with systemic illness, such as fever and vomiting, along with pain and dysuria. Urinalysis will typically show pyuria and haematuria with positive cultures typically for bacteria such as Escherichia coli. Treatment is usually in the hospital with intravenous antibiotics. It is important to remember that men with a urinary tract infection warrant further investigation to exclude anatomical or pathological abnormalities.
Periumbilical pain
Gastroenteritis is a common cause of abdominal pain in primary care. It is typically periumbilical, although it can be diffuse in nature. It can be caused by viral, bacterial, or parasitic infection and often causes abdominal pain with fever, vomiting, and diarrhoea (Snyder and Hyun, 2023). Most cases are viral, transient, and self-limiting in nature (NICE, 2022). Examination involves looking for signs of severe dehydration and exploring the differential diagnosis. Further investigations will vary but could include stool culture and sensitivity testing. Management includes encouraging fluid intake, advising infection control measures for the household, and safety netting when to seek urgent advice (NICE 2022). SBO is an important differential of pain in this area and requires an urgent referral if suspected. Patients typically have severe colicky pain, vomiting, absent bowel movements and flatus. There are often signs of systemic illness and severe dehydration, with examination revealing high pitched ‘tinkling’ bowel sounds and a distended tender abdomen. CT will confirm the diagnosis with treatment including IV resuscitation and nasogastric decompression, although surgical management is often necessary (Ten Broek et al., 2018).
Acute mesenteric ischaemia often presents as central periumbilical pain. However, it can vary depending on the segment of bowel affected. Patients often describe intense abdominal pain, especially after eating, vomiting, and bloody diarrhoea. Admission to the hospital is required with CT evidence of ischaemic gut prompting surgical intervention, including embolectomy and bowel resection. Ruptured abdominal aortic aneurysm is a true emergency and will rarely be seen in primary care because of its acuity. However, occasionally patients present with generalised central discomfort and a pulsatile mass requiring urgent hospital referral for assessment.
Iliac fossa pain
Right iliac fossa (RIF) pain is felt in the lower right quadrant. Abdominal pain in this area or pain that has migrated to this area from the umbilicus may indicate acute appendicitis (NICE, 2021e). Typical symptoms of acute appendicitis include initial periumbilical pain migrating to the RIF over a period of 24–48 hours, exacerbated by movement and coughing (NICE, 2021e). Associated symptoms include anorexia, fever, vomiting, and constipation. On examination, there are many signs that can indicate appendicitis:
McBurney’s point: This point is one-third of the distance from the anterior superior iliac spine to the umbilicus. This point in the lower right quadrant is where tenderness is maximal in the case of acute appendicitis Rovsing’s sign: Palpation of the left iliac fossa causes pain in the RIF. This indicates appendicitis Psoas sign: Abdominal pain on hip flexion, indicative of appendicitis/abscess Obturator sign: Indicates appendicitis; internal rotation of the right thigh causes pain in the right lower quadrant Rebound tenderness: Deep, compressive palpation that is released quickly, causing sharp pain, indicative of local peritonitis from appendicitis
Look out for signs that the patient is systemically unwell; they may be haemodynamically compromised and dehydrated, as indicated by dry mucus membranes and prolonged capillary refill time (NICE, 2021e). There are also many atypical presentations of acute appendicitis, including non-specific abdominal pain, suprapubic pain, and no pain (usually in elderly patients) (NICE, 2021e).
Children can present with lower right quadrant pain on coughing. Abdominal examination may reveal a mass or signs of peritonism, suggesting an abscess of the appendix or perforation. In primary care, if you suspect acute appendicitis arrange emergency hospital admission without delay (NICE, 2021e). Classically, suspected appendicitis is diagnosed by CT or USS, and the diagnosis is confirmed by laparoscopic appendectomy. There has, however, been a shift towards conservative hospital management with antibiotics in non-perforated appendicitis in recent years.
Acute diverticulitis usually presents in the left iliac fossa (LIF), typically in patients with a history of diverticulosis with longstanding pain and irregular bowel habits. Constant abdominal pain, including a change in bowel habit and rectal bleeding or mucus, is indicative (NICE, 2019). Patients are also often systemically unwell with fever, rigors, and haemodynamic disturbance. Examples of complications can be found in Table 5. For patients presenting with suspected acute diverticulitis in primary care, clinicians should consider secondary care referral for same -day assessment, including blood tests and imaging, particularly to exclude signs of perforation (NICE, 2019). Treatment is usually with intravenous antibiotics and surgery if there is evidence of peritonism. Patients with mild disease who are generally well may be treated at home with oral antibiotics, analgesia, antispasmodics, and a low-residue diet, but must be appropriately safety netted with advice to attend the emergency department (ED) if symptoms worsen.
Complications of diverticulitis.
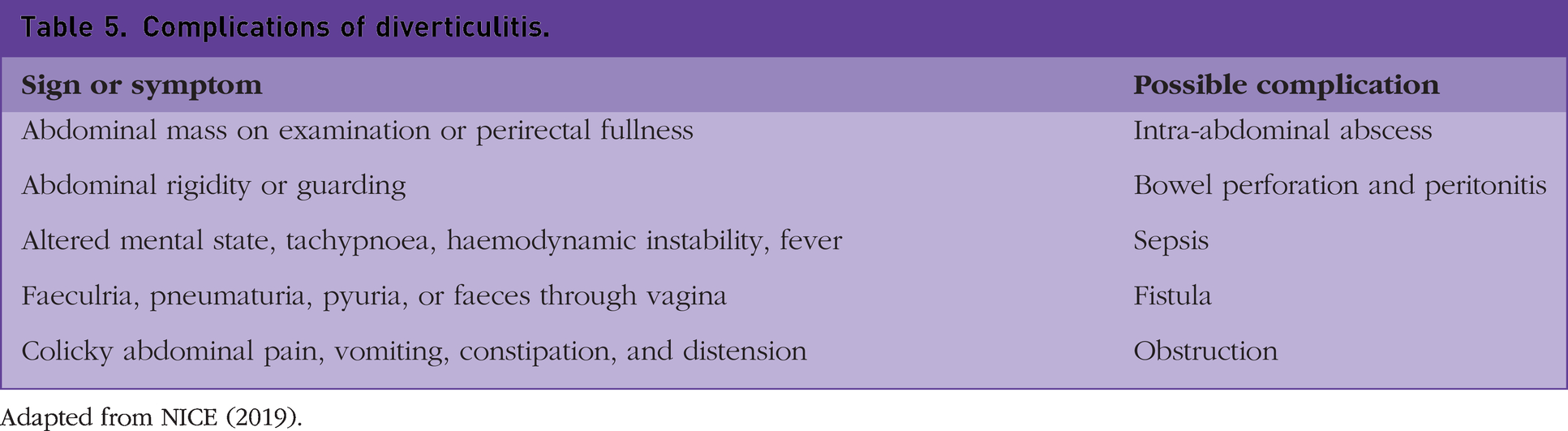
Adapted from NICE (2019).
In women, pregnancy tests should be performed to exclude ectopic pregnancy. If there is abdominal pain with a positive pregnancy test, ectopic pregnancy must be considered and investigated. Ovarian torsion and a ruptured ovarian cyst typically cause sudden onset severe unilateral pain with signs of peritonitis associated with haemorrhage (Snyder and Hyun, 2023). An USS is the investigation of choice, and will guide further management in the hospital. Vaginal discharge and new sexual partners may indicate a sexually transmitted infection such as chlamydia that can lead to PID, which can present similarly (NICE, 2021). Safety netting is very important; thoroughly advise the patient on which symptoms to be aware of and when to go to the ED.
Suprapubic pain
Suprapubic pain is typically caused by urinary tract infections (UTI), however, it can also be caused by various gynaecological and colonic conditions, such as PID and diverticulitis. Dysuria, nocturia, and cloudy urine are common indicators of an UTI (Little et al., 2010). Elderly patients can often have new -onset confusion. Urine dipsticks are often positive for nitrites, leukocytes, and blood and should indicate empirical antibiotics based on local protocols. Cultures are helpful in finding the causative organism and antibiotic choice; however, ∼90% are caused by E.coli (Stamm and Hooton, 1993). Acute urinary retention, commonly due to prostate enlargement, causes severe pain and must be relieved to avoid hydronephrosis and kidney injury.
Generalised abdominal pain
Peritonitis is inflammation of the peritoneum and can be localised or generalised in nature. It can be caused by any abdominal pathology, but typically from bowel obstruction and perforation, leading to the leakage of bacteria and toxins into the abdominal cavity. This causes large fluid shifts and metabolic disturbances, leading to hypovolaemia, acidosis, and electrolyte derangement. Peritonitis carries high morbidity and mortality; therefore, any patient suspected should be promptly referred to the ED. Typical clinical signs include severe abdominal pain, guarding, and rebound tenderness alongside features of a systemic inflammatory response, such as tachycardia, hypotension, tachypnoea, and fever.
Large bowel obstruction can cause generalised pain due to distension and is associated with failure to pass stool or flatus. Patients will usually have marked distension, tenderness, and an empty rectum on the PR exam. It is typically caused by colonic malignancy in ∼60%, but also commonly by strictures and volvulus, particularly in the elderly (Griffiths and Glancy 2020). Treatment is usually surgical with removal or the obstructing lesion, so if suspected needs referral to secondary care.
Inflammatory bowel disease should be considered in young patients (aged 20–40 years) who have a history of recurrent abdominal pain, diarrhoea, and blood or mucus in their stools. The initial work-up in primary care could include a full blood profile to look for any signs of anaemia, dehydration, inflammation and vitamin deficiencies. Stool cultures should be sent to exclude an infectious cause. Faecal calprotectin, if raised, would indicate colonic inflammation, and ultimately warrant secondary care investigation and further management. Flare-ups can be managed in the community if mild; however, significant illness requires admission. See Box 2 for indicators of severity. Indicators of severe flare-up requiring admission. Severe abdominal pain and tenderness Severe diarrhoea >8/day with blood Weight loss and dehydration Fever Tachycardia
Non-specific abdominal pain (NSAP) leads to up to 40% of admissions and is defined by examination and investigations revealing no organic cause for symptoms experienced (Irvin, 1989). Irritable bowel syndrome (IBS) is the most common cause of NSAP, and although a benign condition, it can cause significant distress for patients. Patients experience altered bowel habits, episodic crampy pain, and distension. The Rome IV criteria used to help reach a diagnosis. It is important to thoroughly examine and investigate patients to exclude other pathologies, referring them to secondary care if any concerns. Treatment can include lifestyle and diet modifications, such as low FODMAP diet and exercise. Pharmacological therapies such as laxatives, secretagogues, and antispasmodics also play a role. IBS, along with other causes of NSAP, have strong links with previous physical abuse, sexual abuse, and mental health issues, so a focus should also be on psychological and well-being support.
Conclusion
Abdominal pain is a common, complex diagnostic conundrum for GPs. The decision to admit or not admit is the most pressing and presents a major juxtaposition. The risks of not often referring outweigh the decision to watch and wait and save hospital workload. However, thorough history and examination will help clinicians manage the complex decision making involved in assessing these patients.
Key points
Abdominal pain is a common presentation in general practice
Causes of abdominal pain are very varied as are the different clinical presentations
A basic understanding of the physiology of different types and origin of pain can help in diagnosis of the different pathologies
Careful history, examination, and appropriate investigations are key to reaching a diagnosis
It is important to recognise life-threatening abdominal pathology for urgent referral
Accurate, prompt diagnosis can improve patient outcomes, including symptoms, morbidity and mortality