
Abstract
Migraine typically causes an intense, throbbing, unilateral headache. The exact cause is not known, but involves vascular, chemical and neurological factors. Migraine headache may be preceded by an aura of visual disturbance, weakness/numbness or dysphasia. Nausea, vomiting, photo- and phono-sensitivity often accompany the headache. In most cases, people have episodic attacks of migraine, however, a small proportion of sufferers develop chronic migraine with headaches occurring up to daily. This article will focus on the management of migraine in those aged 12 years and over, including management of acute attacks and chronic migraine. The differential diagnosis will be discussed and red flags that point to alternative diagnoses will be highlighted.
Clinical case scenario 1.
A 35-year-old woman books an urgent appointment with you. She does not have a history of headaches, but earlier that day she had a shimmering visual image, which moved across her vision over about 20 minutes, followed by a severe headache and vomiting. She has taken some ibuprofen, which has taken the edge off the pain, but it is still there. She is worried it is something serious such as a brain tumour.
How do you assess her and reassure her (and yourself) that nothing serious is underlying her symptoms?
Types of migraine: Definitions
Migraine without aura
The National Institute for Health and Care Excellence (NICE) defines migraine without aura as follows (NICE, 2022):
Migraine without aura can be diagnosed in a person presenting with at least five attacks fulfilling the following criteria:
Headache lasting 4–72 hours in adults or 2–72 hours in adolescents Headache with at least two of the following characteristics: Unilateral location (more commonly bilateral in children) Pulsating quality – may be described as ‘throbbing' or ‘banging' Moderate or severe pain intensity Aggravation by, or causing avoidance of, routine activities of daily life (for example, walking or climbing stairs) Headache with associated symptoms including at least one of: Nausea and/or vomiting Photophobia (sensitivity to light) and phonophobia (sensitivity to sound) Headache must not be better accounted for by another diagnosis
Aura
The International Headache Society (IHS) definition of migraine aura is ‘Early symptoms of an attack of migraine with aura, believed to be the manifestations of focal cerebral dysfunction. The aura typically lasts 20-30 minutes and precedes the headache’ (IHS, 2018). Aura can occur without a following headache, which often occurs in older people, and is termed acephalgic migraine.
Migraine with aura
A more detailed definition of migraine with aura is present in the NICE migraine guidelines (NICE, 2022).
Migraine with aura can be diagnosed in a person presenting with at least two attacks fulfilling the following criteria:
One or more typical fully reversible aura symptoms including: ○ Visual symptoms such as zigzag lines and/or scotoma - visual aura is the most common type of aura ○ Sensory symptoms such as unilateral pins and needles or numbness ○ Speech and/or language symptoms such as dysphasia At least three of the following: ○ At least one aura symptom spreads gradually over at least 5 minutes ○ Two or more aura symptoms occur in succession ○ Each individual aura symptom lasts 5–60 minutes ○ At least one aura symptom is unilateral ○ At least one aura symptom is positive ○ The aura is accompanied, or followed within 60 minutes, by headache Headache must not be better accounted for by another diagnosis
Visual aura is the most common type or aura, occurring in 90% of patients who experience migraine with aura (IHS, 2018). A common description of visual aura is of a fortification spectrum: a zigzag figure near the point of fixation that may gradually spread right or left and assume a laterally convex shape with an angulated scintillating edge, leaving absolute or variable degrees of relative scotoma in its wake (Fig. 1) (IHS, 2018).
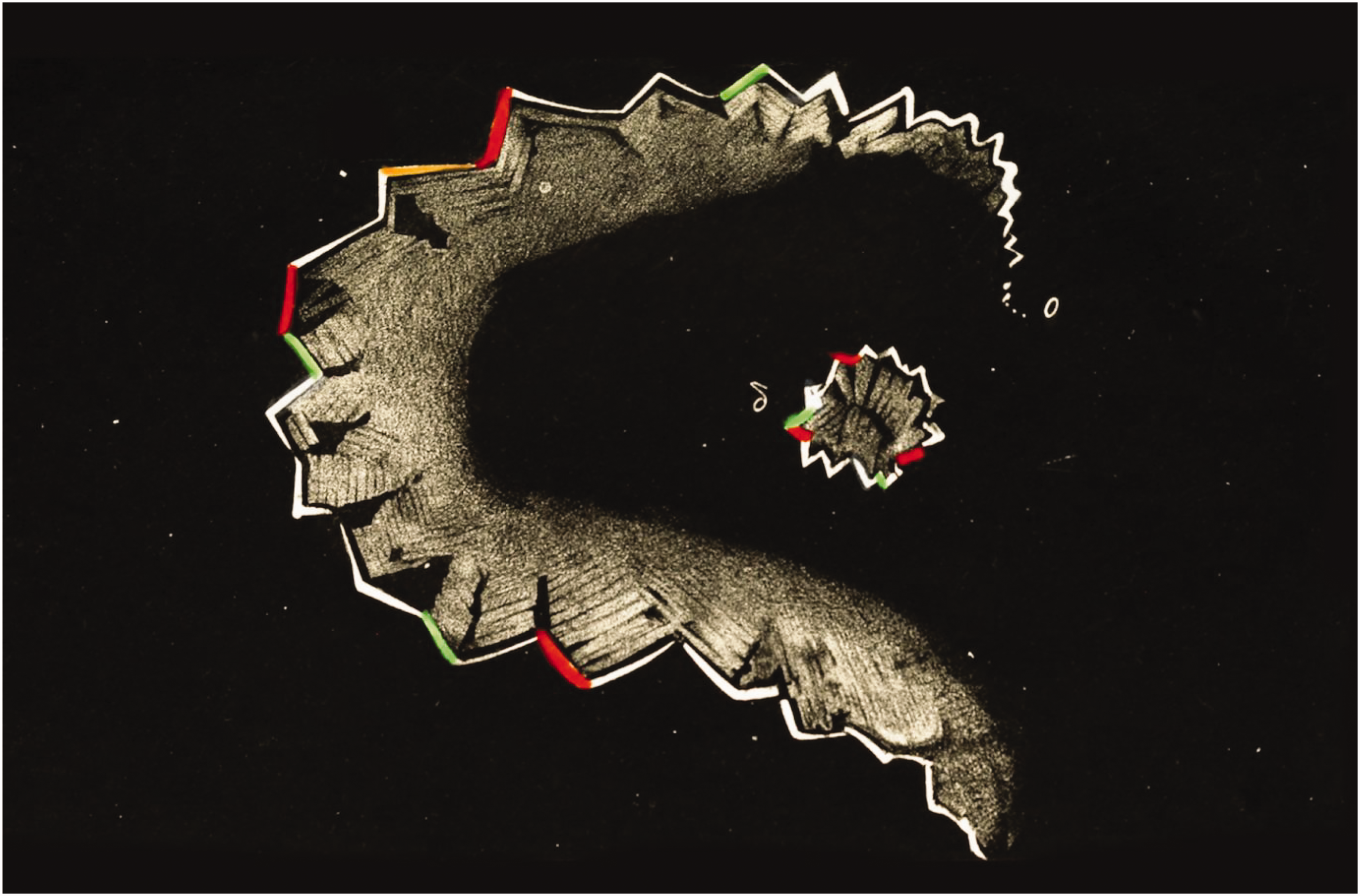
Hubert Airy's 1870 visualization of the scintillating scotoma of his migraine.
Sometimes the aura lacks the positive symptoms of fortification spectra or a shimmering-edged scotoma and is an experience of the visual loss evolving in a similar way.
The next most common type of aura is sensory, such as experiencing pins and needles, which are unilateral and migrate over a similar time period, often leaving a feeling of numbness behind. Sensory symptoms can affect one side of the body, face or tongue. Sometimes the positive features are lacking and numbness is the only symptom experienced.
Probably the least common type of aura is speech-related with aphasia or dysphasia. A famous case is shown on the YouTube video of an American news reporter who developed dysphasia on air, leading to viewers thinking she was having a stroke; this was diagnosed as migraine with aura. It can be seen at: Reporter Serene Branson: Not a Stroke Just a Migraine (02.18.11) – YouTube (see references). This illustrates that the rarer auras can be alarming.
Episodic migraine
Episodic migraine is where the attacks of migraine do not fulfil the definition for chronic migraine, i.e. migraine occurring on fewer than 15 days per month (NICE, 2022).
Chronic migraine
Chronic migraine is defined when there are headaches that occur on 15 or more days per month for more than 3 months, which, on at least 8 days per month, have the features of migraine headache (IHS, 2018).
Menstrual migraine
Menstrual-related migraine should be suspected in women and girls who experience migraine peri-menstrually, occurring between 2 days before and 3 days after the start of menstruation for at least two out of three consecutive menstrual cycles (NICE, 2022).
Phases of migraine
The natural progression of migraine may include a prodrome, followed by the aura then headache and, finally, a post-dromal period. Prodromal symptoms include fatigue, hunger, sleep disturbance, poor concentration, neck stiffness, and yawning and may occur for up to 48 hours before the onset of other symptoms of migraine (NICE, 2022). Post-dromal symptoms include fatigue and elated or depressed mood and may occur after resolution of the headache and can last for up to 48 hours (NICE, 2022).
Management of a patient presenting with acute migraine
When a patient presents with possible acute migraine, it is important to carry out a systematic clinical assessment to determine whether migraine is likely and that the symptoms are not better explained by another diagnosis. The first presentation of migraine, particularly if there is an aura, can be frightening for patients. Since national guidelines remind us to refer patients with possible stroke to the emergency services, this can mean that patients with first episodes of migraine may have the diagnosis made in the emergency department (ED) or in a stroke unit. In some cases, referral to secondary care is best, but here is an approach to clinical assessment to try to determine whether the diagnosis is migraine or if the clinician needs to refer on.
History
A description of the initial symptoms and of the evolution of symptoms is needed to determine if any neurological symptoms described have the evolution and resolution suggestive of a migrainous aura or are of sudden onset and/or are not resolving and so are suggestive of a transient ischaemic attack or stroke.
Does the headache sound like a migrainous headache as defined above? In addition, are there any risk factors for migraine, including medication (e.g. the combined oral contraceptive pill [cOCP]), a family history of migraine, or a history of recurrent tummy ache and vomiting in childhood (sometimes called ‘abdominal migraine’)?
Were there any triggering factors or any trauma? Triggers for migraine can also be a clue such as in menstrual migraine, sleep deprivation, stress and sometimes foods, typically thought to be chocolate and cheese, although food as a trigger is less common than supposed. It can be confusing as the prodrome can lead to hunger and consumption of, for example, chocolate, which then gets blamed for the migraine.
In the over 50s, ask about symptoms of giant cell arteritis (GCA) including temporal headache, jaw claudication and pelvic girdle and shoulder girdle ache and stiffness. Checking for ear, nose and throat (ENT) symptoms, such as sinus pain/nasal blockage can be useful. Considering potential red flags can guide history taking (Box 1). Red flags in the acute history. Visual symptoms or weakness/numbness or speech disturbance lasting longer than an hour raise the suspicion for stroke, even in the young. Positive visual phenomena can occur with occipital strokes. If there have been progressive neurological symptoms with headache then this may indicate an intracranial tumour. Thunderclap headache (sudden onset, severe headache reaching maximal intensity within 60 seconds, and often accompanied by nausea/vomiting and neurological symptoms) could indicate subarachnoid haemorrhage. Neck pain or stiffness may raise suspicion for meningitis or subarachnoid haemorrhage (although sometimes there can be an element of neck ache in migraine). Positional worsening, ie worse on bending forward, may indicate sinus pain or raised intracranial pressure, but can occur with migraine. A history of cancer, clotting problems or combined oral contraceptive pill use can increase the likelihood of cerebral venous sinus thrombosis. Recent trauma (remember subdural haematomas in the elderly, which can present acutely or sometimes weeks after the event).
Examination
How much examination is necessary? The diagnosis will be strongly suspected from the history alone, but in terms of examination some things are felt to be important, either to rule out serious differential diagnoses or because it is expected that the general practitioner (GP) will do them. The scope of examination will be dependent on the patient's age and whether there any persisting symptoms, which then will point to were to concentrate the examination. Otherwise, time is better spent taking the history, especially since the clinician will have observed the gait of the patient and how they move during the consultation.
Taking the blood pressure is sensible (in practice, to rule out malignant hypertension and pre-eclampsia in pregnant women). The patient’s temperature should be checked if infection is suspected.
Fundoscopy can be very reassuring to the clinician if they are able to see clear optic disc margins and central retinal vein pulsation. It is important to practise fundoscopy to enable the clinician to be competent at recognising these features; otherwise, there may be false reassurance. Normal fundoscopy makes raised intracranial pressure unlikely. If there was a visual aura, particularly if it is persisting, then examination of the visual fields in both eyes is needed to check for a homonymous hemianopia/quadrantanopia.
In someone over 50, palpation of the temporal arteries is extremely important. If ENT symptoms suggest this, then palpation of the sinuses and nose may be relevant to check for sinus congestion or infection. If there is suspicion that the headache may arise from cervical spondylosis/osteoarthritis of the neck, then examination of the neck is indicated. Red flags on examination are shown in Box 2. Red flags on examination. Neck stiffness – think of subarachnoid haemorrhage or meningitis. Temporal artery tenderness or thickened non-pulsatile temporal arteries – consider giant cell arteritis Arterial blood pressure of 180/120 or higher – consider malignant hypertension or pre-eclampsia in pregnant women Papilloedema – consider an intracranial tumour, cerebral venous sinus thrombosis, or idiopathic intracranial hypertension
Differential diagnosis of acute migraine
A fairly comprehensive list of the possible alternative diagnoses which, in most cases, a comprehensive history and targeted examination will rule out is presented in Box 3. Differential diagnosis of acute migraine.
Tension headache Trigeminal autonomic cephalgia - eg cluster headache
Transient ischaemic attack/stroke – can be difficult to distinguish in aura phase Subarachnoid haemorrhage Giant cell arteritis Malignant hypertension Infection – meningitis/brain abscess Cerebral venous sinus thrombosis Carbon monoxide poisoning Dental problems Sinus issues Ocular issues - eg closed angle glaucoma Other intracranial bleeds - eg subdural haematoma Brain tumour/raised intracranial pressure Idiopathic intracranial hypertension
Many patients with secondary headache, i.e. headaches due to an underlying cause, will need same-day referral to secondary care, if not immediately to the ED. If GCA is suspected then the clinician must undertake immediate blood testing (full blood count, erythrocyte sedimentation rate and C-reactive protein) and commence oral prednisolone pending the results.
If a dental problem is suspected, the patient needs to see their own dentist as an emergency. If they do not have a dentist or cannot access one, then 111 can arrange an emergency dental appointment for them. GPs should only manage dental problems if they have the competencies to do so.
For a first episode of migraine, particularly if there was a very abrupt onset of headache, then the clinician may be concerned about a subarachnoid haemorrhage (SAH). The Ottawa SAH rule can be of benefit in the assessment of patients with suspected SAH (Box 4). If one or more features are present, this is an indication for investigation (i.e. GP referral to ED). This tool is 100% sensitive with a specificity of 22% in the validation cohort used, so no cases of SAH were missed (Foley et al., 2021). This rule helps avoid over investigation of low-risk patients and avoids missing the diagnosis when applied correctly. Ottawa subarachnoid haemorrhage rule.
Age 40 years plus Neck pain/stiffness Witnessed loss of consciousness Onset during exertion Thunderclap headache Limited neck flexion on examination Source: Foley et al., 2021.
Treatment of acute migraine
NICE recommends the use of simple analgesic drugs (paracetamol, ibuprofen or aspirin), a triptan, or a combination of a triptan with a non-steroidal anti-inflammatory drug for the treatment of headache in acute migraine (NICE, 2022). In 12 to 17-year-olds, a nasal triptan (unlicensed unless sumatriptan is used) is recommended rather than an oral triptan. Aspirin should not be given under the age of 16 (risk of Reye's syndrome).
Addition of an anti-emetic, even in the absence of nausea/vomiting, can be considered, being mindful of age appropriateness. Metoclopramide is effective and also has a direct anti-migraine action, but should not be offered to girls and young women (it is hard to find strict guidance but use over 35-years-old seems pragmatic), due to the risk of dystonic reactions, such as oculogyric crises. Metoclopramide enhances gastric emptying, which is slowed due to the acute migraine, enabling better absorption of the analgesics. Prochlorperazine is a suitable alternative, although possibly less effective.
These medications are best taken at the first onset of headache and may be repeated if the headache is persisting.
Management of a patient presenting with chronic migraine
History
As for the acute presentation, take a detailed history. If a headache diary has not been used already, start one, as this will help to establish the diagnosis, monitor analgesic use and monitor effectiveness of treatment. The National Migraine Centre has one which is available on the internet: (www.nationalmigrainecentre.org.uk/headache-diary/).
Clarify what, if any, analgesics are being taken and how frequently. What is the impact of the migraines? Are there any predisposing factors such as inadequate sleep, stress or poor eyesight? Check they are not on predisposing medications, such as the cOCP. Are they up-to-date with their eye tests? It is debatable to what extent chronic migraine is linked with ophthalmological or visual issues, but a normal eye examination by an optician is reassuring and occasionally an underlying cause, such as the need for glasses, may be found.
Sleep apnoea can be a factor underlying chronic headache. It is worth carrying out an assessment for this if someone has a history of excessive daytime sleepiness and/or a history of snoring.
On review of the symptoms, ensure there are none of the red flags or atypical features summarised in Box 1. It is also important to clarify that the patient's symptoms resolve between episodes, otherwise look for other pointers which may indicate a different cause of chronic daily headache, for example raised intracranial pressure or medication overuse headaches (MOH).
Clinical case scenario 2.
A 45-year-old woman presents in tears. For the last year she has had almost daily headaches, some of which are like the migraines she used to get around her period with nausea and one-sided throbbing. She is taking paracetamol and ibuprofen nearly every day but with little effect. It is ruining her life.
How do you proceed?
Examination
As for examining some with acute migraine, check the blood pressure, perform fundoscopy and examine anything appropriate from the history. Remember to assess for signs of GCA in the over 50s.
Imaging of patients with migraine in primary care
There is debate about the merits and disadvantages of brain imaging in primary care. Studies have principally looked at computed tomography. Magnetic resonance imaging (MRI) does not use ionising radiation, so this should be the modality to consider. Some areas now have direct GP access to MRI.
Good’s guidelines for neuroimaging in headache (Good, 2019) is an excellent review of the issues around imaging and gives useful guidance for when to image. The guidelines advise that imaging is not indicated in patients with a clear history of uncomplicated migraine without red flag features for potential secondary headache and who have a normal neurological examination. This is because there is only an approximate 0.2% prevalence of significant intracranial abnormalities found on imaging in such patients.
The guidelines also state that clinicians should be aware that imaging can identify incidental neurological abnormalities, which may result in patient anxiety. Establishing advice and guidance mechanisms with local neurologists is vital in managing these cases.
The guidelines above looked at the evidence for reassurance provided by brain imaging for chronic daily headache. In summary, at 3 months after normal brain imaging, anxiety levels were lower. However, this improvement was lost by 12 months, although those that were imaged consulted less during this time period.
Therefore, ideally imaging should not be carried out solely for the purpose of reassurance, given the risk of picking up an incidental abnormality. This risk should be discussed with patients who request imaging, so that an informed decision can be made whether to go ahead with it.
New onset headache in the over 50s, especially if there are focal symptoms, is an indication for imaging. This is because there is an increased risk of malignancies in this group (Kernick et al., 2008).
Treatment of chronic migraine
First, lifestyle advice can be helpful. This can include avoiding any known triggers, staying hydrated, limiting caffeine and alcohol intake, taking regular exercise, keeping to a healthy weight and getting regular sleep (Exeter Headache Clinic, 2019; NHS, 2022; The Migraine Trust, 2021).
Second, if there is an element of MOH, discuss stopping the analgesics for at least 1 month. NICE advises stopping triptans, ergotamines and simple analgesics abruptly. Explanation is the key here, because the headaches will usually get worse (possibly together with other withdrawal symptoms) before they get better. Timing of this step is important according to what is going on in their life currently (so not just before an important work or family event, for example). Improvement of the headaches usually starts 1-2 weeks after withdrawal and improvement can take up to 2-3 months (NICE, 2022).
Third, consider prophylactic treatment, mindful that there need to consider realistic expectations (NICE, 2021). A good response to prophylactic treatment is considered to be a 50% reduction in the frequency and severity of episodes (hence, the importance of a headache diary so this can be assessed). All medications can cause side effects so there needs to be a discussion with the patient about this affect, emphasising that these will often settle in time. It is important that the dose of each drug be titrated gradually, every 2 weeks or so, until the maximum tolerated dose is reached. Most drugs will require patients to be treated for at least 8 weeks at the maximum tolerated dose before response to the drug can be assessed (Hovaguimian and Roth, 2022).
The first line prophylactic treatment is propranolol (avoid in asthma, bradycardia and peripheral vascular disease) – see NICE (2022) for advice on other beta blockers where propranolol is not suitable. The second line drug is topiramate, but it should be avoided if there are any plans for pregnancy and if the patient is a woman of women of childbearing age then highly effective contraception is needed, as it is teratogenic. Bear in mind that it can cause hepatic enzyme induction and lessen the contraceptive effectiveness of some hormonal contraception (including the cOCP, progestogen-only pill and the progestogen-containing implant). Other options are amitriptyline (or nortriptyline if amitriptyline is too sedating) and pizotifen (limited evidence but licensed). Oral vitamin B2 (riboflavin) 400 mg/day helps some individuals. This can be purchased over-the-counter. Common side effects of riboflavin are yellow urine and sometimes diarrhoea. Do not offer gabapentin or pregabalin for migraine prophylaxis.
If three or more trials of prophylactic agents (at effective doses for long enough) fail then consider referral to a specialist for consideration of botulinum toxin type A or calcitonin gene-related peptide (CGRP) inhibitors (anti-CGRP monoclonal antibodies), which have recently been approved and made available for eligible patients in secondary care. It is important in the referral letter to list what drugs have been previously tried, at what maximum dose and for how long. Also, ask the patient to fill out headache diaries before they are seen as these will be required before the above can be prescribed.
Whichever prophylactic agent is used, consider gradually weaning down and stopping it after 6-12 months if the migraines have resolved, this can be successful in many patients. However, this step is often forgotten in primary care.
Management of menstrual migraine and factors for girls/women with migraine
In women with predictable cyclical migraine, there are some special considerations. The cOCP contains oestrogen, which increases the risk of stroke and this should be avoided in women with migraine, certainly if there is migraine with aura. Referencing the United Kingdom Medical Eligibility for Contraception (UKMEC) guidance (Faculty of Sexual and Reproductive Healthcare, 2016), migraine with aura is UKMEC 4 (use gives an unacceptable level of risk) and without aura is UKMEC 3 (the risks generally outweigh the benefits), but if there was migraine with aura more than 5 years ago this is UKMEC 3. The progestogen-only pill (usually desogestrel) or a long-acting reversible contraceptive is preferable.
As with all migraine, give MOH avoidance advice and check for any triggers or red flags. With purely menstrual migraine, NICE (2022) suggests the following options: frovatriptan 2.5 mg twice daily on the days migraine is expected or from 2 days before until 3 days after bleeding starts; or zolmitriptan (2.5 mg twice or three times daily) on the days migraine is expected or from 2 days before until 3 days after bleeding starts.
Conclusions
In assessing a patient with migraine, a structured approach is extremely helpful. Learning fundoscopy and being comfortable undertaking this technique is vital for a thorough assessment of both acute and chronic headache.
Using a headache diary early on is particularly useful to establish the frequency, use of medications and for monitoring progress with treatments. If preventative treatments are used, it is important to use each one in turn (unless inappropriate for an individual), ensuring that an effective dose is used for long enough. This may mean the maximum dose tolerated by an individual for 3 months and ensuring it is documented clearly in the notes. Gathering this information is vital as it will be needed for any secondary care referral for specialist treatment.
Key points
In all presentations of headache, fundoscopy is mandatory New onset headache, especially with focal symptoms, in the over 50-year age group is an indication for imaging Consider giant cell arteritis in the over 50-year age group Avoid prescribing the combined oral contraceptive pill in women with migraine (UKMEC 3 or 4 depending on aura or not) Medication overuse headache is common Follow the guidance on preventative treatments using each medication chosen at the maximum tolerated dose for at least 8 weeks before deciding it is ineffective and moving on to the next step