
Abstract
During ice hockey, pucks travel at high speeds and have the potential to cause substantial injury. The neck and torso are vulnerable locations where protective materials could mitigate impacts and reduce injury. Currently, neck guards are tested solely for cut protection, while no known standards exist for chest protection. To assess products and materials, a novel test surrogate was required with realistic body geometry (for product mounting) and stiffness (reflecting body compliance). The neck and clavicle were instrumented, and hockey puck impacts were applied to each in an unpadded condition, as well as with eight foams and three commercial neck guards in place. Protection of each material was quantified as the reduction in force relative to the unpadded condition. The greatest force reduction with a foam was 42%–46% (neck-clavicle), supporting its potential use in equipment. Only one of the commercial neck guards provided impact resistance (39% force reduction, vs 4%–6% in the others). Without injury tolerance data for the neck, it is unknown if the materials would have prevented injury; none reduced load below the reported fracture tolerance of the clavicle. This test surrogate and investigation may inform the future development of standards for improved hockey equipment design and evaluation.
Introduction
Ice hockey (or simply hockey) is a popular sport played worldwide, with players regularly reaching skating speeds of 9–11 m/s (20–25 mi/h) and ice-cold vulcanized rubber pucks reaching velocities over 45 m/s (100 mi/h) at elite levels.1,2 At these rates, mild to severe injury can easily occur from a variety of sources and affect numerous anatomical locations. The majority of hockey-related injuries occur to the head, neck, and shoulder region (50.6% of reported injuries), with body-to-body (27.2%), stick-to-body (21.1%), and direct puck collision (12.3%) representing the primary sources of injury. 3 Removal of intentional body-to-body contact within Alberta and British Columbia minor hockey reduced concussion and injury rates by 62%, while similar rule changes in US high school hockey resulted in a 40% reduction in reported injury rates.4,5 With more widespread policy changes regarding body checking anticipated, and stick-to-body contact currently prohibited, injury resulting from a direct puck impact may become more critical to address for amateur and youth hockey players.
Direct puck impacts occur frequently throughout the course of a hockey game due to players either accidentally or intentionally placing themselves within the line of fire from a shot toward their net. In the 2023–2024 National Hockey League (NHL) season, 39,406 shots (∼30 shots/game) were blocked by non-goalie players (i.e. forwards and defencemen). 6 This total does not include when a player accidentally blocks a shot from their teammate; as such, the number of players struck with a puck is likely higher than reported. Hockey puck strikes induce a focal load with high impact energy over a small impact duration, capable of producing serious and/or fatal injuries depending on impact location and quality of equipment. 7 Puck impacts to the head, neck, and precordium (due to risk of commotio cordis) represent the most critical impact locations (potentially Abbreviated Injury Scale (AIS) 5+), while impacts to the clavicle, sternum, ribs, and extremities pose a risk of contusion and fractures for a player.
It is currently unknown how effective hockey equipment is at protecting players from direct puck impacts to the neck or chest. Hockey equipment test standards are limited to helmets, their various forms of facial protection (e.g. visor, cage, etc.), and neck guards due to the associated potential serious health outcomes.8–10 Chest protection (commonly referred to as shoulder pads) has received minimal attention in the literature, with their effectiveness in reducing injury not being reported.11,12 Governing hockey organizations, such as Hockey Canada, are responsible for outlining any additional mandatory protective equipment to be used during competition, including chest protection, though how hockey organizations determine what is considered safe equipment is not currently public knowledge. 13 This lack of equipment standardization leaves the remainder of a player’s body potentially vulnerable to injury as, apart from helmets and facial protection, current equipment is not required to attenuate hockey puck impacts (as no known test standard exists).
Current commercial neck guards must adhere to the Bureau de Normalisation du Quebec (BNQ) 9415-370 safety standard, which states that all neck guards must effectively minimize the risk of direct laceration from a skate blade to the neck. 10 The standard does not address impact resistance. The consequences of puck impacts to the neck have been well documented in the literature and media. A Quebec minor hockey player died recently (2023) due to a direct puck blow to the neck despite wearing a BNQ-certified neck guard. A previous study also reported five cases of direct puck strikes to the neck resulting in death. 14 The cause of death in each case was due to dissection or rupture of either the carotid or vertebral artery from a slapshot or a deflected shot. Another study outlined four cases of laryngeal fracture among hockey players, one of which resulted in a player requiring emergency intubation due to severe respiratory distress, and two required surgical repair. 15 Though not common, direct puck impacts pose an extremely serious risk to players of all ages; thus, including impact resistance in neck guard standards may provide critical protection.
Hockey puck impacts to the chest can also produce serious and/or fatal injury, including commotio cordis. Commotio cordis, described as sudden cardiac death due to induced ventricular fibrillation, is caused by a blunt impact to the chest at a specific time in the heart’s electric cycle, disrupting its natural rhythm, 16 and 8% of all reported commotio cordis cases have occurred during organized hockey (while the individual was wearing shoulder pads). 17 The only known standard for evaluating the protection a chest protector provides against commotio cordis was developed by the National Operating Committee on Standards for Athletic Equipment (NOCSAE) for baseball and lacrosse, though it has not been adapted for hockey. 16
Puck impacts to the chest can also cause injury to the ribs, sternum, and clavicle. Though substantially less severe than commotio cordis, injury to these regions can be debilitating and costly for the affected individual. Fractures of the clavicle, a common location in hockey, 18 can have significant health and economic burdens associated with them, including medical costs and loss of work that can reach upwards of $18,000 USD/patient. 19 With the return-to-play time for clavicular fractures averaging 9.1 weeks in hockey, injured players are additionally burdened with being unavailable for a large portion of their season. 20 Though less common than clavicular injuries, severe rib and sternal fractures can damage the vital organs they protect (e.g. punctured lung).
Adequate assessment of hockey neck and chest protection requires the use of a test platform that accurately models the mechanical stiffness of a specific anatomical location at a given loading rate of interest, while also providing high repeatability to ensure consistent results. 21 Use of accurate anatomical stiffness ensures the protection provided by padding is not over- or under-estimated. Multiple chest surrogates currently exist, including the Hybrid III (Humanetics, Farmington Hills, Michigan, USA) Anthropomorphic Test Device (ATD), THOR ATD (Humanetics, Farmington Hills, Michigan, USA), and the NOCSAE commotio cordis test surrogate. ATDs have been investigated for their use under baseball and lacrosse ball impacts, but greatly overestimated impact forces (at a range of speeds), suggesting they would likely be inaccurate for hockey puck loading conditions as well, 22 while also not having the required instrumentation in the regions of interest. The NOCSAE commotio cordis test surrogate effectively predicts the risk of commotio cordis from baseball and lacrosse ball impacts between 13.4 and 22.4 m/s (30–50 mi/h), though it is not known if the surrogate is effective at modeling impacts from a hockey puck.16,22 Development of a hockey-specific test surrogate would facilitate performance analyses of hockey equipment in response to direct hockey puck impact.
The purpose of this study was to develop a novel test surrogate to model the neck, clavicle, sternum, and ribs in response to hockey puck loading conditions for assessment of chest and neck impact protection in hockey. The second objective was to impact an assortment of padding options, including commercial hockey neck guards, under hockey puck-like conditions to quantify the range of protection provided by existing materials and verify surrogate functionality.
Methods
Test surrogate
To determine the target stiffness values for the anatomical regions of interest, a review of dynamic impact literature was performed for the neck, clavicle, sternum, and lower ribs (Table 1). Blunt impacts (in the anterior-posterior (A-P) direction) were the focus, as these were considered most relevant. All clavicular, sternal, and rib studies identified were performed at automotive loading rates or lower (<10 m/s); as no studies could be found at loading rates expected in amateur to elite level of play (19–45 m/s, or 42–100 mi/h). 23 Automotive loading rates have been found to be similar to an adult beginner woman player’s wrist shot velocity, suggesting it may be an effective comparison for introductory levels of play. 24 Most data available were in vivo, providing sub-injurious stiffness values, though four post-mortem studies were found that reported the stiffness of the sternum at fracture. From these data, the clavicle target stiffness was defined as 185.3 N/mm, and the sternum and the rib were 168.3 and 173.6 N/mm, respectively.
Dynamic blunt loading literature for the clavicle, sternum, and ribs.
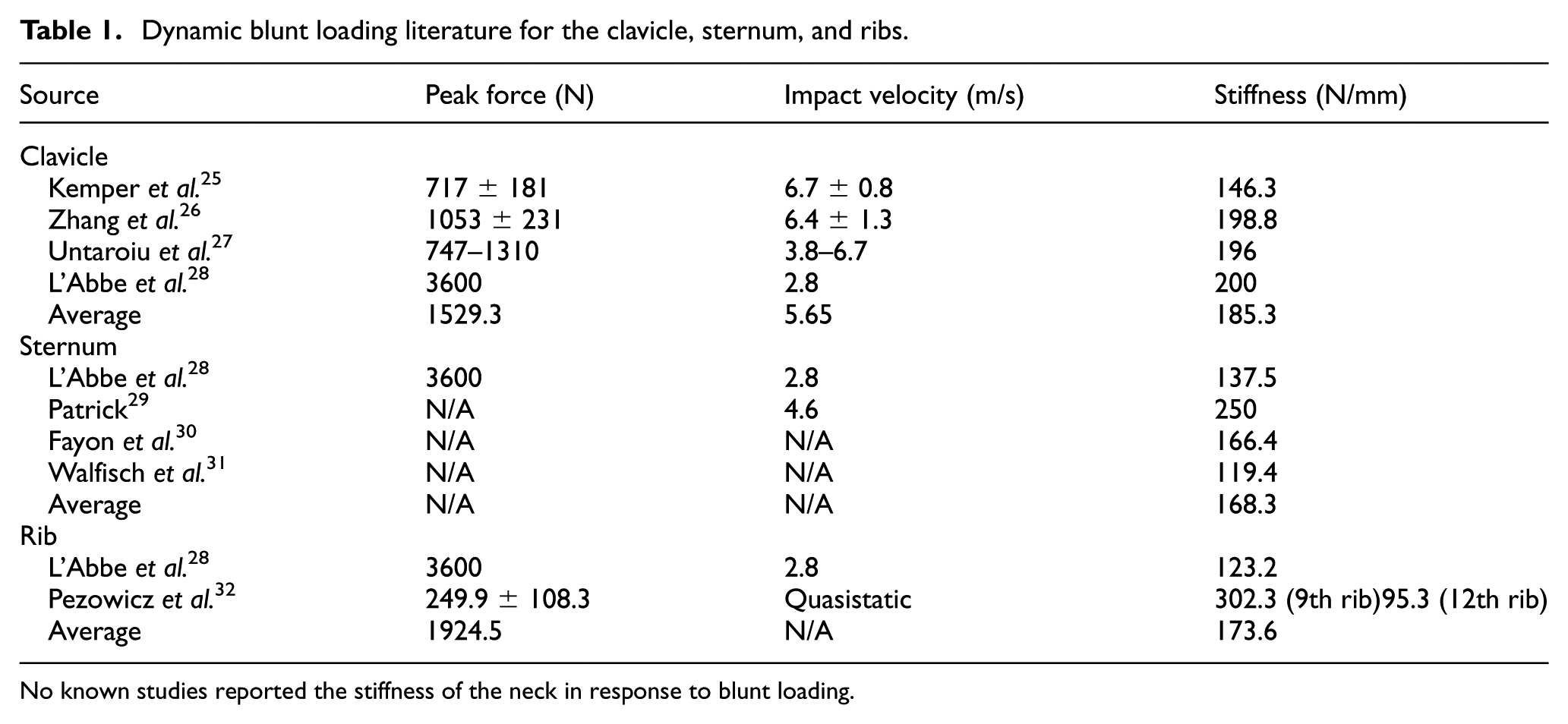
No known studies reported the stiffness of the neck in response to blunt loading.
Literature surrounding the stiffness of the neck in response to blunt A-P loading did not appear to exist at the time of this study. To address this lack of information, a finite element (FE) simulation was performed to estimate the stiffness of the neck when impacted by a hockey puck using LS-DYNA (Ansys, Inc., Canonsburg, PA, USA) v12.1 symmetric multiprocessing solver (SMP), with data collected at 67 kHz. The THUMS AM50 V6.1 (Toyota Central R&D Labs, Inc., Nagakute, Japan) human body model (HBM) was impacted using a rigid cylinder with a diameter of 7.62-cm (3″), thickness of 2.54-cm (1″), and a weight of 156-g (5.5-oz), the dimensions of a regulation hockey puck. 33 The impactor was prescribed an initial velocity of 20.6 m/s (46 mi/h), to mimic a shot from a recreational player; the target level of play for this study. 23 Full post-impact translation and rotation were permitted to match the real-world scenario. Due to the seated position of the HBM, the head and neck posture were not neutral. The impactor position was modified by angling the puck at 24.8° to the horizon to load the hyoid bone in the altered HBM posture. The hyoid bone was targeted as it is a commonly injured structure within the neck. Stiffness was calculated by taking the slope of the force-deformation response once neck loading began, with a node on the surface of the neck in contact with the puck being selected for the deformation time history. Some initial loading remained due to the puck contacting a portion of the chin area; thus, stiffness was calculated only when loading was purely upon the structures of the neck (Figure 1(b)). A resultant stiffness of 131.3 N/mm was identified.
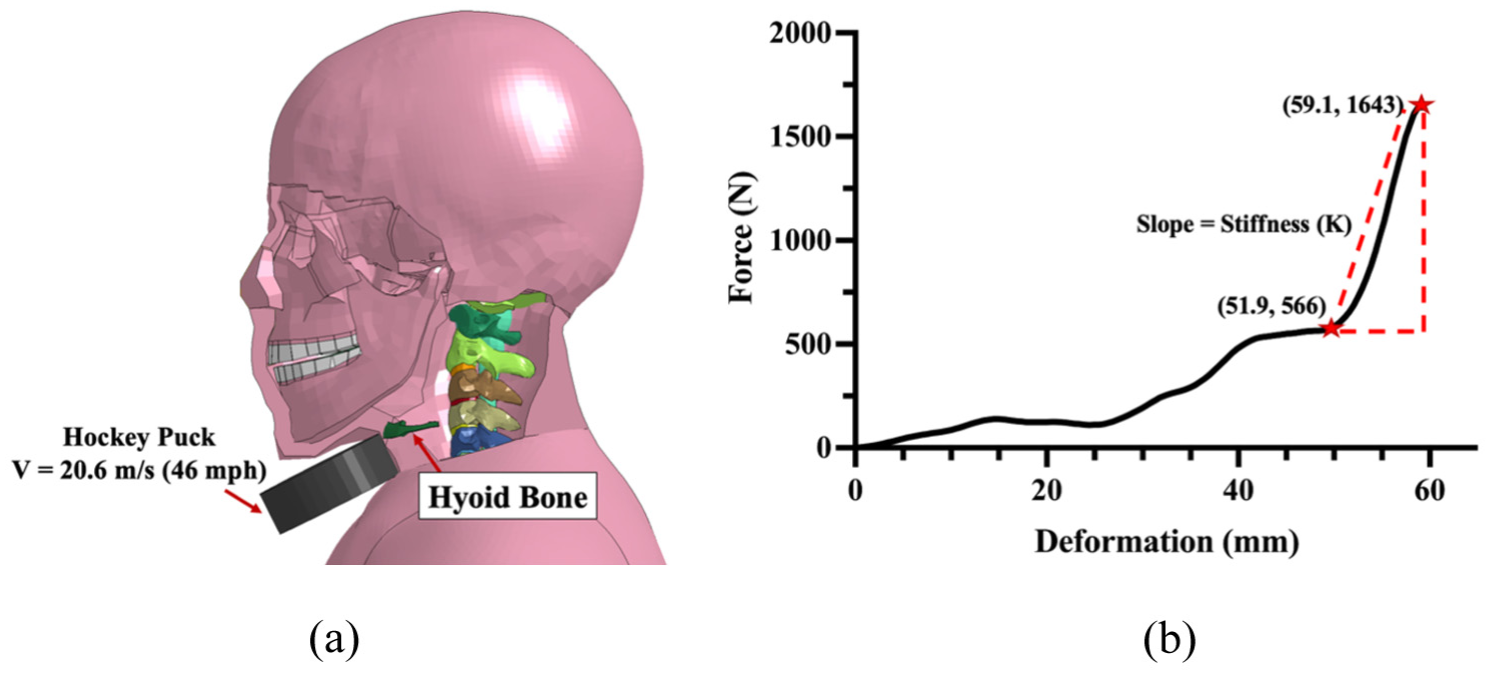
(a) Initial loading of the hyoid bone when impacted by a hockey puck at 20.6 m/s (46 mi/h) and (b) force-deformation curve during loading of the neck. Force and deformation were measured from the impactor’s first contact with the neck soft tissue, neglecting the loading from contact with the chin area.
Each anatomical location’s stiffness was represented using a chrome-silicone compression spring (McMaster-Carr, Elmhurst, Illinois, USA), selected to be within 10% of the target, as springs with exact target stiffnesses could not be found, while still being well within the variance observed in human studies.34,35 The selected spring stiffnesses were 177 N/mm for the clavicle, 160 N/mm for the sternum and rib, and 124 N/mm for the neck. Compression springs were housed in a 4.6-cm (1.6″) diameter polyvinyl chloride (PVC) tube to ensure normal compression and reduce any unintended bending of the spring (Figure 2(a) and (b)). A smooth stainless-steel rod, an acetal bushing, and a 3.8-cm (1.5″) aluminum washer were used to minimize friction. A male mannequin body (Eddie’s Hang-Up Display Ltd., Vancouver, British Columbia, Canada) was used as the frontal impacting surface (Figure 2(c)) to provide realistic anatomical geometry and to allow commercial products to be worn as intended during testing.
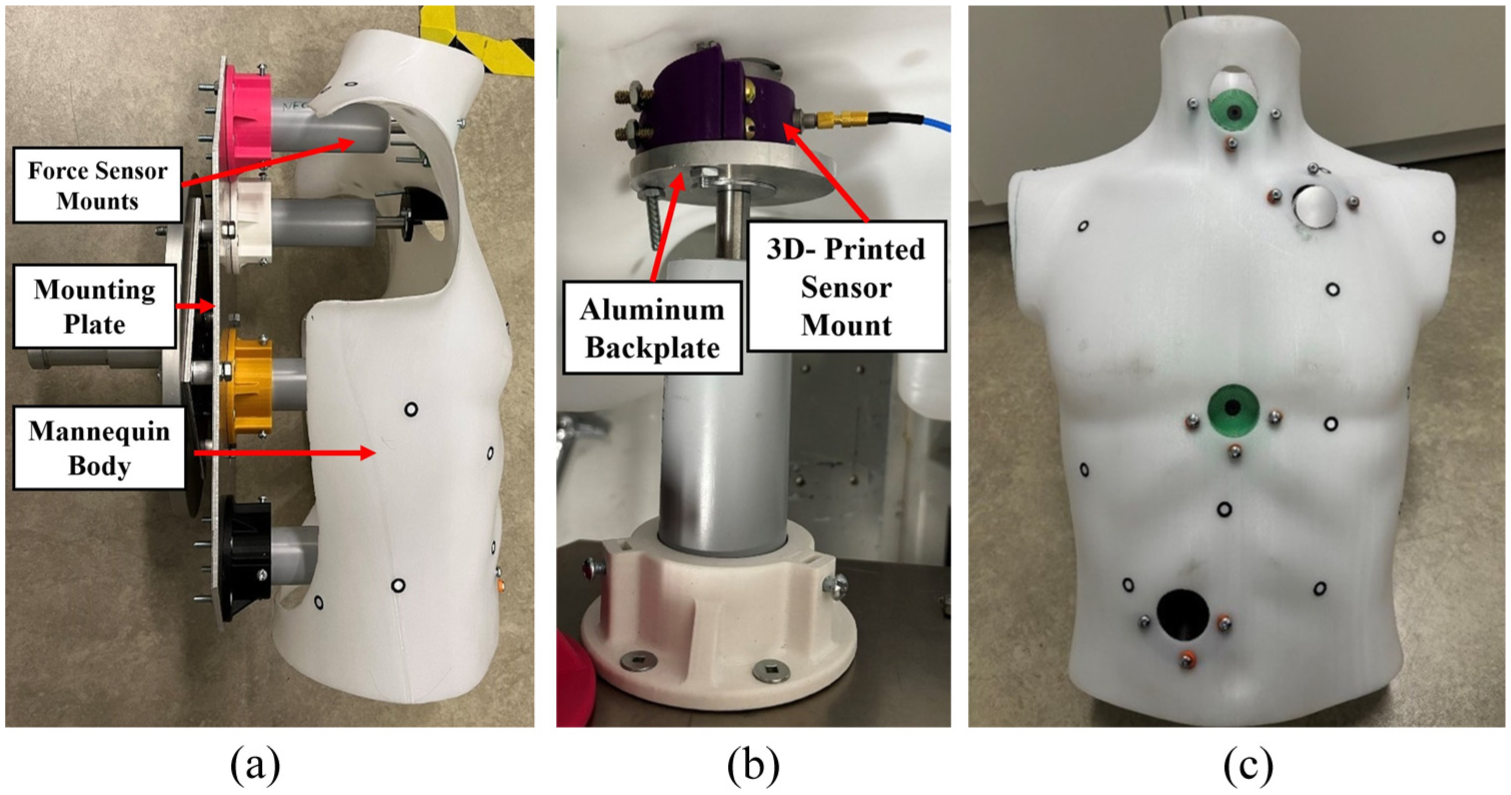
(a) Side-view of fully assembled surrogate mounted to the attachment plate of the test rig, (b) close-up of clavicular spring subassembly equipped with a force sensor. The custom 3D-printed sensor mount ensured the force sensor was flush with the body surface, and (c) frontal view of assembled test surrogate with a force sensor at the clavicle.
Each impact location was instrumented with a PCB 200C20 (PCB Piezotronics, MTS Systems Corporation, Depew, New York, USA) piezoelectric force sensor. The force sensor has a maximum measurement capacity of 88.96 kN and a frequency response of 40 kHz. Sensor mounts were designed to support the PCB 200C20 force sensors securely (Figure 2(b)). To allow sensor mounts to sit flush within the contoured internal surface of the mannequin, the body form was 3D-scanned to provide the exact shape of its interior. Computer-aided design (CAD) files of each sensor mount were modeled and 3D-printed using polylactic acid filament (Prusa i3 MK3S+, Prusa Research, Prague, Czech Republic). To increase the mechanical strength, high-density print settings were used, including a print resolution of 0.25-mm, an infill of 25%, and a perimeter of 6-mm. Each sensor mount was attached to a 7.62-cm (3″) diameter, 0.53-cm (0.21″) thick aluminum reinforcing backplate to provide further strength (Figure 2(b)). Holes were cut in the surface of the mannequin (3.81-cm [1″] diameter) to allow the force sensor to be impacted directly (Figure 1(c)). Each of the four spring subassemblies was mounted via a 3D-printed flange to a large 0.47-cm (3/16″) thick aluminum backplate to support the entire surrogate for testing.
Dynamic impact testing
All impacts were performed using a pneumatic impacting apparatus previously used in multiple studies (Figure 3(a)).34–36 The apparatus uses compressed air to accelerate a projectile down a 1.83-m long tube, where it then strikes an object of interest within the impact chamber (Figure 1(a)). The novel test surrogate was mounted within the apparatus via a support structure that allowed vertical and horizontal alignment of the anatomical location of interest with the exit of the acceleration tube (Figure 3(a)). No post-impact translation was permitted to reflect the inertia of the body. A previously developed projectile 34 was modified to mount a sectioned regulation hockey puck (Figure 3(b)). The projectile (mass = 386g) was propelled through an acceleration tube to strike the surrogate with a target impact velocity of 13 m/s (29 mi/h). This combination of mass and speed was chosen to replicate the impact energy (32.6 J) of a 20.6 m/s (46 mi/h) hockey puck (assuming puck mass of 156g), a value similar to the NOCSAE commotio cordis speed range 13.4–22.4 m/s (30–50 mi/h); while staying within the constraints of the pneumatic impacting system.
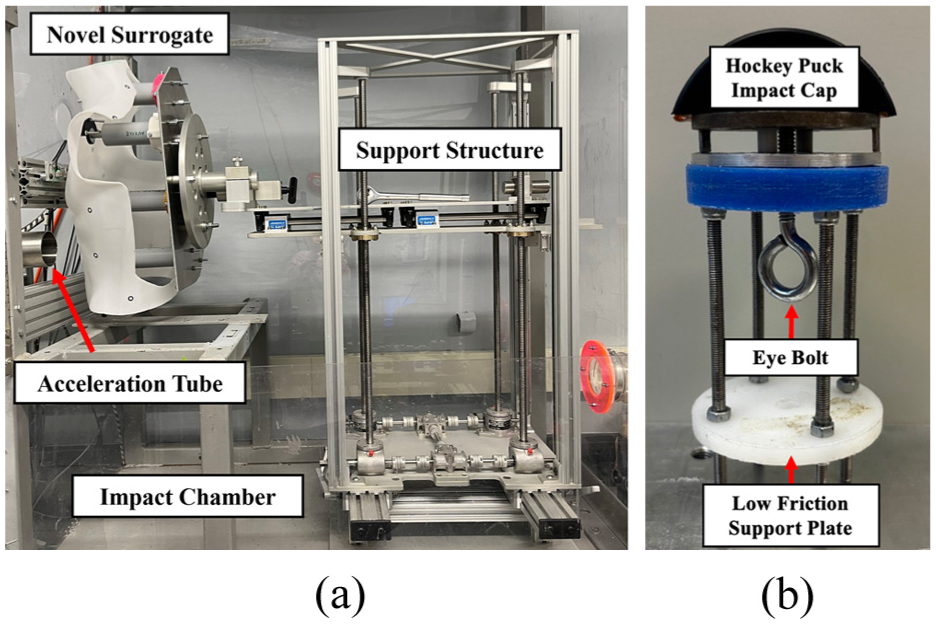
(a) Pneumatic impacting apparatus with novel surrogate installed. The support structure allows vertical, horizontal, and rotational alignment of the surrogate with the acceleration tube and (b) the impact projectile used for dynamic testing had a front-sectioned regulation hockey puck impact cap.
A thin layer (1.67-mm) of vinyl was placed on the force sensor impact cap to reduce vibration noise. Two LR-X 250C optical sensors (Keyence Corporation, Osaka, Japan) measured the impact velocity of the projectile. Force data were collected using a NI-PXIe-1082 Data Acquisition system (National Instruments, Austin, TX, USA) with a PXIe-4480 module sampling at 1 MHz.
Initial impact testing was performed to characterize the baseline response of the surrogate (with no padding present). Five impacts were performed at both the neck and clavicle. The rib and sternum locations were not tested to focus herein on the highest and lowest stiffness locations (hypothesized to demonstrate the range in protective capacity of materials). Repeatability of the surrogate, the difference between the neck and clavicle impact responses, and structural strength of the surrogate (qualitatively) were assessed to evaluate surrogate functionality.
Eight different materials (D3O Inc., London, UK), including EVA foam (MEARCOAH®, China), were evaluated for their impact attenuation (Figure 4(a)). Cut to 50-mm × 50-mm (2″ × 2″) size, one piece of each material was tested at each location, with double sided tape holding the materials in place. Five impacts were applied to each, with the same foam sample being used for all trials to assess the effect of repeated impacts on attenuation (with 10 min recovery between tests as multiple impacts can occur quickly in hockey). Samples were only replaced if the material was noticeably damaged after an impact.
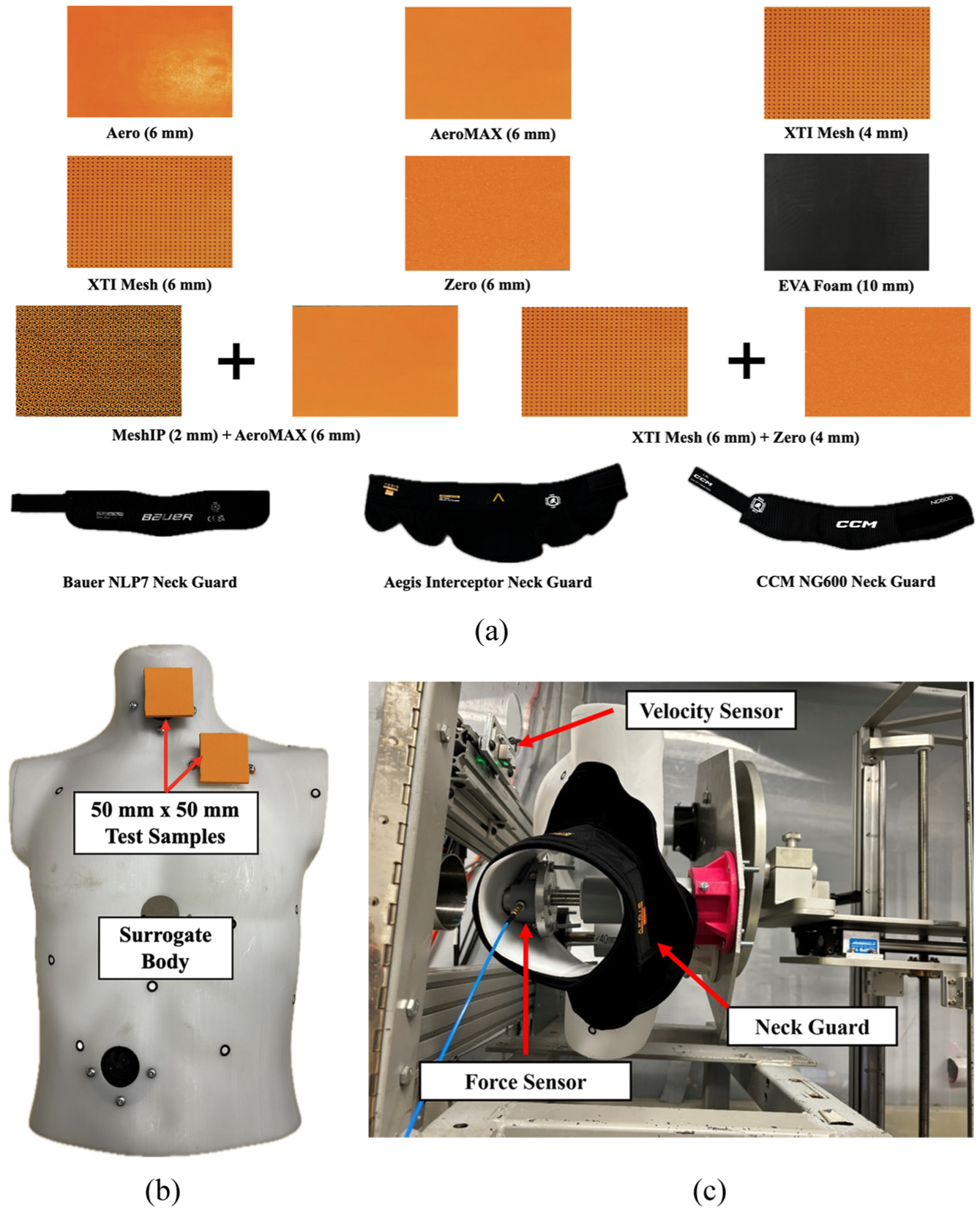
(a) The eight materials tested at both the neck and the clavicle, along with the three hockey neck guards tested, (b) placement of 50 mm × 50 mm AeroMAX test sample, placed at the neck and clavicle impact location, and (c) novel surrogate wearing the Aegis Interceptor neck guard. Protection provided by material/neck guard was quantified by the embedded force sensor.
Three commercially available hockey neck guards, the Bauer NLP7 (Bauer Hockey LLC, Peak Achievement Athletics, Exeter, NH, USA), the CCM NG600 (CCM Hockey, Sport Maska Inc., Montreal, QC, Canada), and the Aegis Interceptor (Aegis Impact Protection, Hamilton, ON, Canada), were also tested. Each neck guard was secured on the surrogate as intended to be worn (Figure 4(b)). Five impacts were performed on each neck guard model, with samples being replaced between trials only if severe damage/deformation was observed.
Peak force, coefficient of variation (CV), and percent force reduction of each foam/neck guard (relative to unpadded) were the primary metrics investigated. CVs were calculated separately for each material at each location, with a CV below 10% considered acceptable. 37 CVs of the unpadded trials were used to assess surrogate repeatability, while CVs of padded trials were used to assess multi-impact consistency of each material. Welch’s t-tests were performed between padded and unpadded trials, and trials at different impact locations, to determine if the level of impact attenuation provided, or the change in stiffness between the neck and clavicle, was significant (α = 0.05).
Results
In total, 105 (45 clavicle and 60 neck) dynamic impacts were performed. Impact velocity measured 12.9 ± 0.49 m/s (28.9 ± 1.1 mi/h; CV = 3.8%) across all impacts, with a corresponding impact energy of 32.1 ± 2.4 J. Unpadded impacts resulted in a mean peak force of 8277 ± 186 N (CV = 2.3%) for the neck, and a mean clavicle peak force of 9886 ± 328 N (CV = 3.3%), which were significantly different (p = 0.0001). The force-time histories for the neck and clavicle were similar, with both quickly rising to their respective peaks, before unloading at a similar rate to zero (Figure 5).
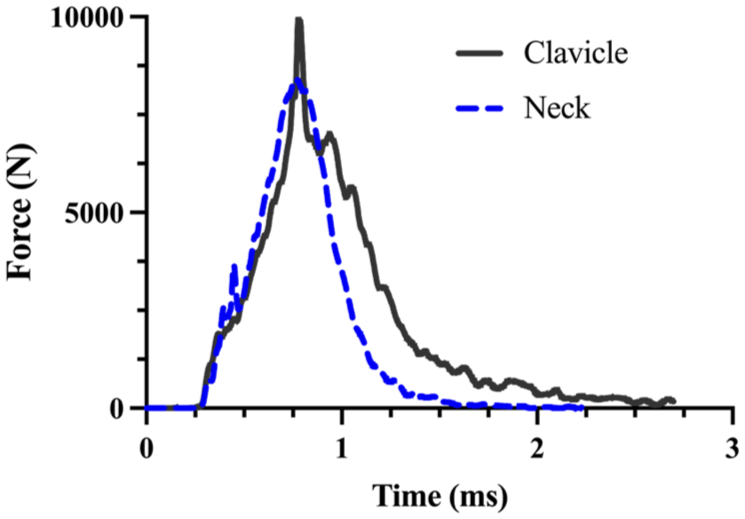
Representative force-time plot for the unpadded neck (dashed blue) and clavicle (solid gray) impacts.
Each material tested reduced the peak force from the unpadded condition with varying magnitudes (Figure 6). The XTI mesh (6 mm) + zero (4 mm) provided the largest force reduction for both the neck (mean force reduction = 42%) and the clavicle (mean force reduction = 46%). The EVA (10 mm) and zero (6 mm) foams provided the least protection at both locations. At the clavicle, the EVA (10 mm) and zero (6 mm) provided a similar level of attenuation (p = 0.59), reducing peak force by 13% and 14%, respectively. The impact attenuation provided by the EVA (10 mm) and zero (6 mm) was significantly different (p = 0.004) for the neck, with the EVA (10 mm) providing 18% force reduction, while the zero (6 mm) reduced the force transmitted to the surrogate by 8.1%. CVs for each of the eight materials tested were 1.2%–5.1% at the neck and 1.8%–4.6% for the clavicle. EVA foam (10 mm) samples were replaced after each impact due to large residual deformation that did not recover. All other materials maintained their integrity throughout the five impacts; thus, they were not replaced. When comparing the XTI Mesh at 6 and 4 mm, increasing material thickness had a modest improvement in force reduction. These reductions were 2.2% at the neck (not significant, p = 0.16) and 7.3% at the clavicle (significant, p < 0.0001).
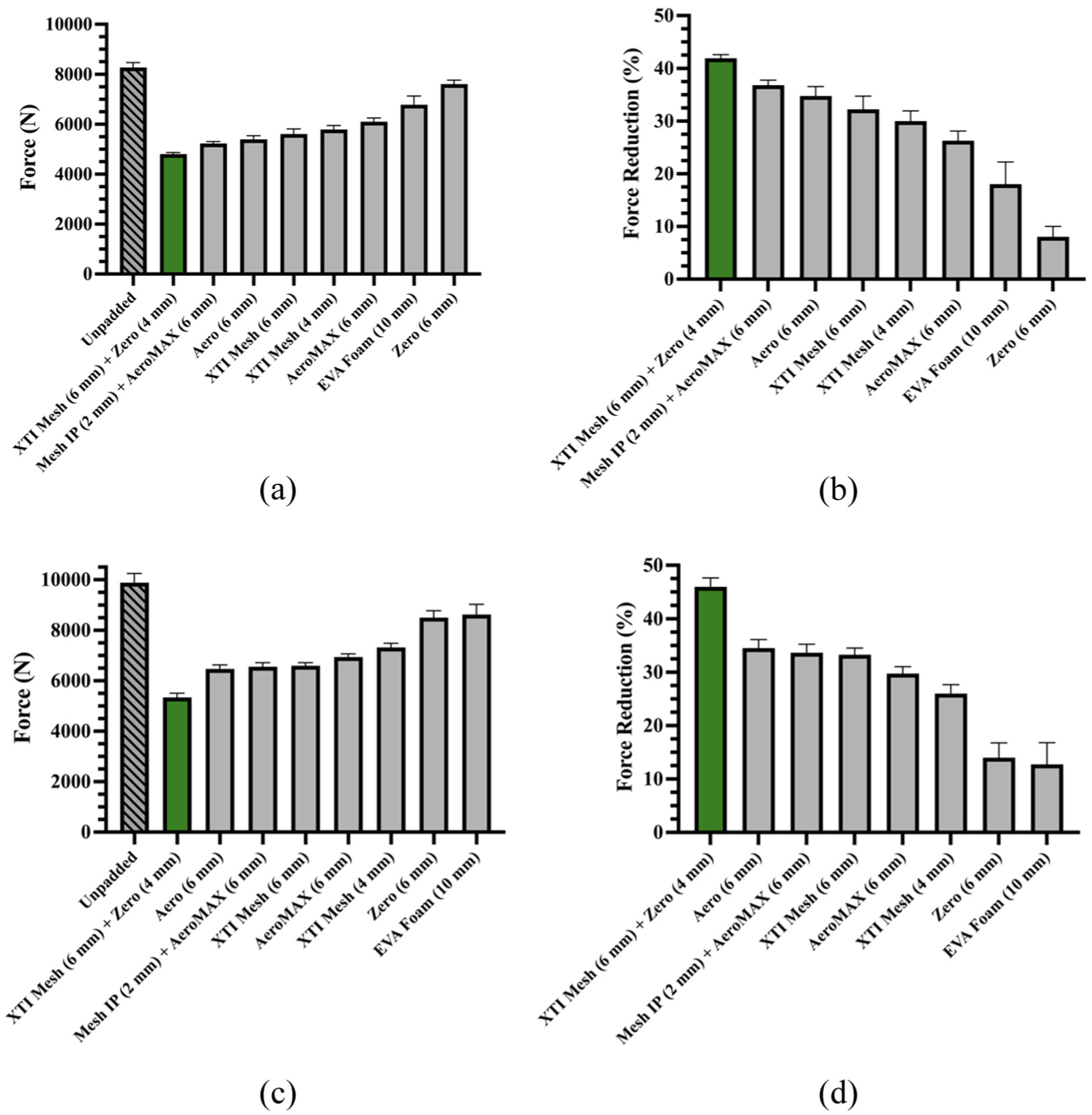
Protection provided by materials. Peak force for: (a) neck and (c) clavicle was measured by the force sensor in the surrogate. Percent force reduction for (b) neck and (d) clavicle were calculated relative to the unpadded tests at the same location. Green indicates the material that provided the greatest force reduction from the unpadded condition (gray hatched bars).
Of the three commercial neck guards, the Aegis Interceptor provided the greatest force reduction, reducing transmitted force by 39% (Figure 7). In contrast, the Bauer NLP7 and CCM NG600 had significantly lower attenuation (p < 0.0001) than the Aegis Interceptor, providing 6.4% and 4.4% peak force reduction, respectively, though these reductions were significant when compared to the unpadded condition (Bauer: p = 0.001, CCM: p = 0.008). Repeatability was high for each neck guard, with CVs of 1.3%, 1.4%, and 3.2% for the Bauer NLP7, the CCM NG600, and the Aegis Interceptor, respectively. However, the Bauer NLP7 and CCM NG600 products were replaced after each impact due to visible physical deformation. The Aegis Interceptor did not show any visible deformation or performance changes over the five impacts, thus only a single sample was used for all tests. Neck guard thickness did not influence performance as the Aegis Interceptor provided the largest force reduction despite being the thinnest of three guards tested (Aegis Interceptor = 9.9-mm, Bauer NLP7 = 10.2-mm, CCM NG600 = 15.5-mm).
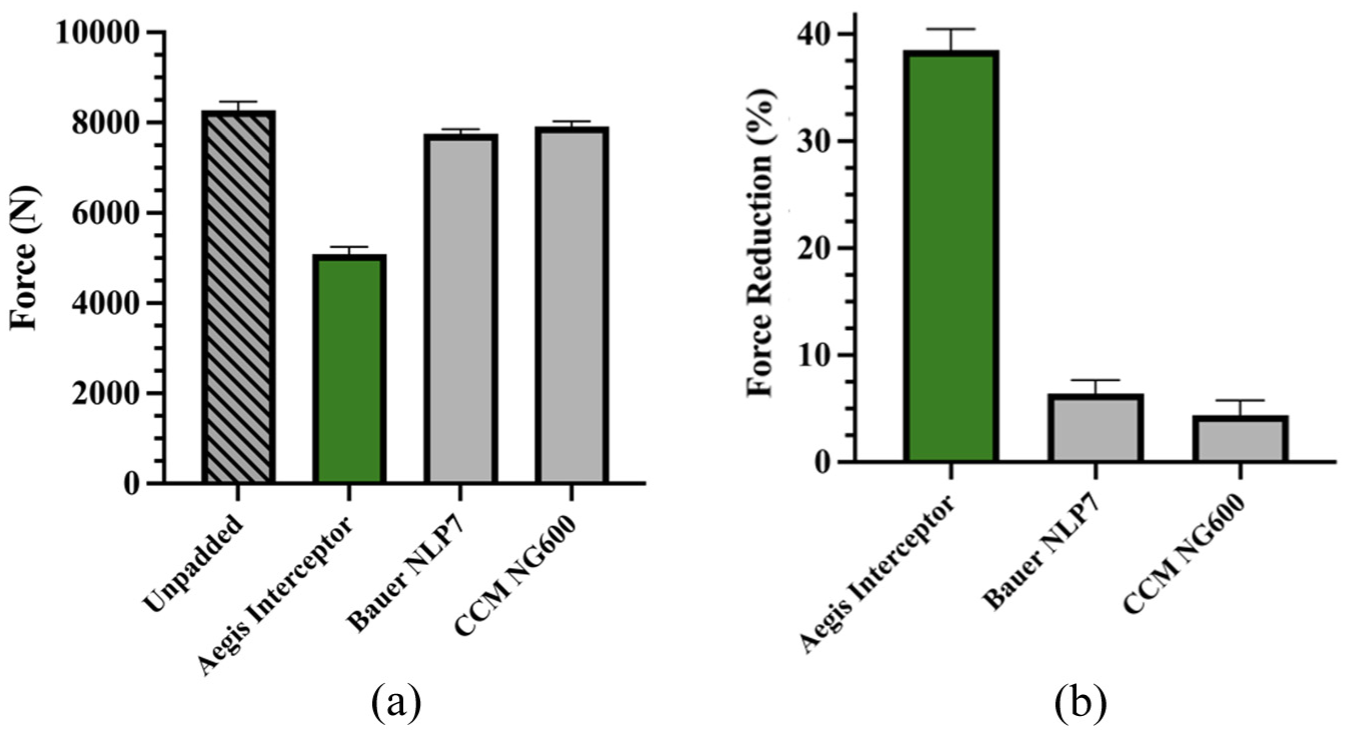
Protection provided by commercially available neck guards. (a) peak force was measured by the surrogate force sensor and (b) percent force reduction was calculated relative to the unpadded tests. Green indicates material that provided the greatest force reduction from the unpadded condition (gray hatched bars).
Discussion
This study represents the first known test surrogate developed specifically to assess chest and neck protection in response to hockey puck impacts. Four anatomical locations (neck, clavicle, sternum, and lower rib) were represented to investigate the protection hockey equipment provides to each location, given their noted weaknesses. The novel surrogate developed was based on the success of other platforms, such as the CSA Z325:20 hip protector platform 21 and the NOCSAE commotio cordis surrogate, 16 identifying accurate mechanical stiffness, anatomical geometry, effective mass, and surrogate repeatability as key design features to evaluate protective materials adequately. Previously, standards (such as equestrian chest protectors 38 ) have relied on using rigid anvils for their test surrogates due to simplicity and consistency considerations, though these provide limited accuracy as they do not generally mimic anatomical stiffness or geometry. Neglecting anatomical compliance in surrogate design may allow test materials to compress more than they would on the human body, leading to an overestimation of their protective capabilities. This study is also the first to quantify the impact protection provided by current commercially available hockey neck guards, highlighting the current vulnerability of hockey players due to a lack of comprehensive equipment standards.
Each of the eight foams tested reduced the peak force experienced at both the neck and clavicle, with a large range of effectiveness. Similar trends in force reduction were observed for both the neck and clavicle, but the neck measured smaller peak forces due to its increased compliance. For both impact locations, the XTI mesh (6 mm) + zero (4 mm) provided the largest reduction in peak force (42%–46% force reduction), indicating it is a good option for future hockey equipment design. Neither the EVA (10 mm) nor zero (6 mm) would be recommended for future implementation as they collectively performed the worst (8%–18% force reduction). None of the tested materials reduced clavicular peak force below its reported fracture limit (700–3600 N25–28), suggesting that when used alone, the tested materials would not provide enough protection to eliminate injury risk. In the present study, materials were not tested with hockey shoulder pads worn overtop, as would be used in play. Hockey shoulder pads provide some clavicle protection via a hard shell; thus, the combination of higher-performance materials and shoulder pads may reduce clavicle impact forces below injurious levels, and is an area for future investigation.
The EVA was the only foam option that required replacement between tests. After impact, it showed severe deformation, with puck indentation nearly the entire depth of the foam that recovered only minimally over time. The remaining seven foams showed no significant visual wear, with no drift in performance, indicating their potential ability to provide multi-impact protection (within the constraint of the five impacts applied). Hockey equipment degradation can also be caused by factors not considered in this study, such as sweat and washing cycles. Future studies should quantify the effect of these factors on the performance of protective materials.
The materials tested herein ranged in thickness from 4 to 10 mm, where one material (XTI mesh) was tested in two thicknesses. The thicker samples only improved protection at the clavicle (stiffer location), highlighting the importance of body stiffness representation in protective material testing. Generally, thicker materials are expected to provide greater protection, 39 but this may be limited by densification of the foam and “bottoming out.” The difference in thickness limits the direct comparison among the various materials, where the “best” performing samples were among the thickest (10 mm). It is possible that an alternate combination of materials could provide similar or even superior force reduction within the same thickness. Increased thickness generally comes at the expense of comfort and flexibility, and thus, user experience is an important consideration not investigated herein. Sacrificing comfort and flexibility for increased protection may hinder widespread player adoption, limiting the purpose of the protective improvements. Future work should quantify the effect of material thickness on impact absorption during hockey puck impacts to determine the ideal thickness for protective equipment.
Comparison of commercially available neck guards identified the Aegis Interceptor as the only potentially effective option in response to direct puck impacting, providing a 39% force reduction compared to the unpadded scenario. This product is marketed as providing impact protection along with the BNQ-required cut protection; thus, these results were unsurprising. There was no observed decline in performance after repeated impacts, indicating that the Aegis Interceptor is likely capable of offering protection against multiple strikes. Due to the lack of injury limit research for the neck in response to blunt trauma, it is not currently known if any of the neck guards tested would reduce impact force below injurious levels. The only potentially relevant study of the human neck was in response to strangulation, identifying a fracture force of 1406 N for the hyoid bone, with substantial compression of the larynx occurring as well. 40 None of the materials tested reduced peak force below this level, indicating bone fracture and laryngeal injury may occur even while wearing a neck guard, though the risk of serious injury and/or death may be reduced. It should be noted that though the direction of loading is similar between a hockey puck impact and strangulation, the loading rate and contact area differ substantially, indicating this value should be used cautiously in the context of this study. It is also likely that some post-impact kinematic motion of the player could further absorb energy, which was not reflected in the current setup (thus representing a potential “worst case” scenario). The Bauer NLP7 and CCM NG600 neck guards both provided low impact attenuation, unsurprisingly, as current neck guard test standards only require cut resistance. Bauer and CCM represent the two largest hockey equipment companies, and their neck guards are widely used among youth and amateur players. Cases of serious injury and death due to puck strikes while wearing a neck guard have been reported in literature and media,14,15,41,42 further signifying the need for neck guard standards also to consider impact protection.
While the results of this study provide previously unknown insight into the effectiveness of materials when impacted directly by a puck, impacts were limited to a singular impact velocity (∼13 m/s, equivalent impact energy of a 20.6 m/s or 46 mi/h hockey puck) using a controlled pneumatic impacting system. Within a hockey game, pucks may travel at a wide range of velocities depending on age and level of play, and may contact at a range of orientations, potentially indicating that the worst-case scenario may not be represented in this study. In recreational play, pucks can average 22.4 m/s (50 mi/h) compared to 33.6 m/s (75 mi/h) for elite players. 23 The focus of this study was to determine the effectiveness of protective materials for amateur play; thus, an impact velocity within this range was chosen. Elite-level impacts may result in reduced protection due to increased puck velocities, though the magnitude of this reduction is currently unpredictable due to the unknown rate dependence of both protective foams and human tissue. Additionally, impacts performed in this study are already well above postulated neck injury limits (1406 N), suggesting impacts at elite levels would likely cause injury. To quantify the effectiveness of protective equipment fully, impacts should be performed over the range of expected impact velocities to ensure the viscoelastic material behaviors of foams and anatomical structures are properly considered. Additionally, the novel surrogate used in this work is limited to single-axis force measurements, therefore any off axis loading present during testing is not currently accounted for in the results, a common limitation among other surrogates.
Limitations
The clavicle, sternum, and rib were modeled using compression springs that closely matched the mechanical stiffnesses reported in the literature. Previous studies were included in the review only if soft tissue was present during testing, due to the impact attenuation provided by soft tissues. Specimen sex and anthropometry were not consistent across, nor within, the studies referenced; thus, the values may reflect larger or smaller body sizes with varying amounts of soft tissue. An increase in soft tissue thickness has previously been shown to increase impact attenuation due to the additional tissue providing more depth for energy absorption. 43 Furthermore, the surrogate was based on a male mannequin, and as such, only qualitatively matches male geometry. Future development of population-specific (e.g. 50th percentile male) stiffness data could provide a more refined and accurate model. Use of mass scaling could also lead to additional surrogates to be designed for other populations of interest, such as fifth percentile females and children, allowing for targeted equipment testing for specific ages and sexes.
No studies could be found investigating the stiffness of the neck in response to blunt impacts; thus, neck stiffness was estimated using a human body model. The THUMS HBM is a widely used open-sourced tool for impact biomechanics investigation. At the time of this study, the THUMS neck model has been validated for its kinematic motion during frontal, lateral, and rear sled tests, though its ability to model blunt loading accurately has not yet been evaluated. The cadaveric blunt impact data required to validate it in this mode do not currently exist; thus, its accuracy is presently unknown. The THUMS has been validated for blunt impacts to various other parts of the body,44–46 which may indirectly lend confidence to its use as an investigative tool for this study. Should the state of knowledge on neck impact stiffness change, the compression springs could easily be altered to reflect this. The surrogate could also be adapted to investigate impacts in other sports or fields by outfitting it with the relevant protective equipment and the current methodology repeated.
Surrogate biofidelity could not be readily quantified in this study due to the lack of relevant biomechanical response data for the neck under high-speed blunt impact conditions. No experimental studies examining blunt trauma to the neck or throat could be identified at the time of this study, as the field has historically focused on neck injury from bending. Unlike the neck, clavicular stiffness used in this study was obtained from previous dynamic post-mortem human subject (PMHS) experiments investigating the clavicle’s response to seatbelt loading, which tends to occur at velocities below 7 m/s. Though potentially more compliant than the stiffness expected from puck impacting (due to viscoelasticity of clavicle), it was necessary to base clavicle stiffness on seatbelt loading scenarios as no research has been completed at higher rates. These limitations in available data prevent direct comparison between the surrogate and actual human biomechanical response in the context of high-speed, localized, blunt impacts. Future evaluation of surrogate biofidelity should be conducted once the necessary dynamic response corridors become available, to ensure the surrogate’s response is biomechanically accurate under hockey puck loading.
Conclusions
Effective standardization of protective equipment requires a repeatable test methodology, including the use of a test surrogate that provides accurate anatomical geometry and stiffness, to characterize the level of protection provided. A novel biomechanical test surrogate was developed to evaluate protective materials, including commercial neck guards, against hockey puck impacts to the neck and clavicle. The surrogate was designed to mimic the geometry and stiffness of the body to minimize potentially overestimating protection provided by a material due to unrealistic anatomical compliance. Testing showed considerable variation in impact attenuation among materials, with one commercial neck guard and four material options providing moderate protection. None of the materials tested herein reduced impact forces below the likely injury thresholds, indicating further equipment improvements may be warranted. This work may inform the development of improved standards for neck and chest protection and provide guidance for advancements in hockey equipment design, enhancing player safety.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Niko Apparel Systems, who were not involved in data collection or interpretation of the results presented.