
Abstract
Reports of greater incidence of knee pain and injury in older female runners compared with their younger counterparts may be associated with differences in lower limb biomechanics that influence knee joint loading. The aim of this study was to investigate footwear interventions aimed at influencing lower limb biomechanics in older female runners (>45 years). Strategies for reducing peak rearfoot eversion and the external knee adductor moment were investigated, since both measures have been associated with knee joint injury. Twenty female runners (mean age 50.7 ± 5.6 years) performed 10 running trials in four footwear conditions: neutral running shoe (Control); neutral shoe with 4° medial heel wedge insole (Medial Wedge); neutral shoe with 4° lateral heel wedge insole (Lateral Wedge); and neutral shoe with combined insole with 5° lateral wedge and medial arch support (Combined Insole). Peak rearfoot eversion and knee external adductor moment were compared for the four conditions using RMANOVA and post-hoc Tukey tests (p < 0.05). Compared with the Control, peak rearfoot eversion was lower for the Combined Insole condition, with this value being lower than for all other insole conditions (p < 0.05). Compared with the Control, the peak knee external adductor moment was lower for the Lateral Wedge and the Combined Insole conditions (p < 0.05). These results support the use of a combined insole with lateral wedge and medial arch support for the reduction of peak rearfoot eversion and peak knee external adductor moment, variables that have been associated with increased risk of knee injury. If aiming to reduce knee external adductor moment alone, then the lateral wedge technology employed in this study provides an effective method for older female runners.
Introduction
Increased leisure time and a greater awareness of the associated health benefits of exercise have led to unprecedented growth in the number of older adults performing regular exercise.1,2 However, it has been reported that older athletes participating in sports activities have a high injury rate compared to younger participants, 3 with females reported to be at particularly high risk. For example, females have been reported to experience greater levels of knee pain and osteoarthritis.4,5 The identification of strategies for reducing the risk of injury in older females when participating in running activities is of particular importance if this population is to benefit from increased activity levels.
In order to develop approaches to reduce risk of injury in older female runners, it is first important to identify whether there are specific characteristics of the running gait of this population that may predispose them to injury. Characteristic features of running gait reported for older female runners compared with their younger counterparts have included greater rearfoot eversion and knee external adductor moment. 6 Large magnitude and velocity of rearfoot eversion have been associated with increased risk of developing lower limb overuse injuries from resulting high knee internal rotation. 7 A high magnitude of knee external adductor moment has been identified as a risk factor for the development and progression of medial knee osteoarthritis,8,9 a condition of particular concern in older females. 10 It is therefore suggested that strategies for the control of rearfoot eversion and knee external adductor moment are of particular importance for older female runners. The manipulation of footwear characteristics presents a potential strategy for influencing these measures, with the level of support identified as a particularly important design feature in footwear for the ageing population. 11
Footwear support typically relates to the level of medial-lateral stability – the level of control of inversion/eversion of the foot. 12 Manipulation of this medial-lateral support has been used as a strategy for reducing rearfoot eversion and knee external adductor moment. However, the specific interventions are potentially conflicting – increased medial support has been demonstrated as a method for reducing the level of rearfoot eversion, 13 whereas increased lateral support has been found to be a useful strategy for reducing knee external adductor moment. 14 This presents a challenge when attempting to develop a footwear intervention to reduce both of these measures.
Design strategies for influencing the level of medial-lateral support provided by footwear include manipulation of the geometry and materials of the mid and outsole, as well as the addition of insoles. Traditional approaches at controlling rearfoot movement have focused on supporting or blocking inward rolling (pronation) of the foot with a stability/motion control shoe or orthotic device with medial support, with some evidence that these strategies can reduce the amount of rearfoot movement. 13 However, since this medial support potentially causes abduction of the tibia, this may cause a lateral displacement of the knee, increasing the moment arm of the ground reaction force about the knee joint centre, thus increasing the knee external adductor moment. Therefore, a footwear intervention with added medial support may be beneficial for restricting the level of rearfoot eversion, but may increase the knee external adductor moment.
A footwear or shoe insert design feature that has had demonstrated success in the reduction of knee external adductor moment during walking is the introduction of a lateral wedge insole.15–17 The mechanism for this reduction has been reported to be through a redirection of the ground reaction force vector, reducing the moment arm about the knee joint and thus the magnitude of the frontal plane moment. Whilst lateral wedging presents a possible intervention for reducing knee external adductor moment, such an intervention places the foot in a more everted orientation relative to the ground, which may increase the amount of rearfoot eversion relative to the lower leg, an effect that has been reported in walking. 18 In walking studies, lateral wedging ranging between 4° and 14° has been reported to be effective in reducing knee external adductor moment. 17 However, larger degrees of wedging have been associated with discomfort and non-adherence.17,19 Therefore, relatively low levels of inclination are more likely to be a suitable intervention in runners.
Owing to the characteristic features of high rearfoot movement and knee external adductor moment generally observed in older female runners, this population may benefit from footwear with specific design characteristics aimed at providing control of these features of running gait. This study aimed to investigate the effect of varying medial-lateral support of inserts on both rearfoot eversion and knee external adductor moment. The influence of adding a 4° medial wedge or a 4° lateral wedge was investigated. In addition, a commercially-available combined orthotic device incorporating 5° lateral wedging and medial arch support was included. This orthotic insole has been demonstrated to limit rearfoot eversion and knee external adductor moment during walking, 20 whilst the influence on running gait has not been explored. It was hypothesised that during running (i) the medial wedge insole (Medial Wedge) would decrease rearfoot eversion and increase knee external adductor moment; (ii) the lateral wedge insole (Lateral Wedge) would decrease the peak knee adductor moment, with an accompanied increase in rearfoot eversion and knee internal rotation angles; (iii) the combined orthotic device (Combined Insole) would reduce rearfoot eversion and knee external adductor moment.
Methods
Twenty older female runners (mean age 50.7 years, standard deviation (SD) 5.6) were recruited from a local women’s running club, with this number of participants based on a statistical power analysis performed using data from a previous study of older female runners. 6 All volunteers described their running as recreational, with a minimum of 5 years running experience. Each runner participated in at least three 1-h running sessions per week. All training was done with the same group, having similar 10 km personal best times (60.9 ± 4.2 min). Participants had no history of orthopaedic or neurological ailments that could affect their running gait. They were also free from symptoms of a musculoskeletal injury or knee osteoarthritis at the time of testing, verified using a knee pain survey (KOOS knee osteoarthritis observation survey; scores mean 89.2, SD 2.6; Roos and Lohmander 21 ). Prior to data collection, each runner completed a Physical Activity Readiness Questionnaire (PAR-Q, Canadian Society for Exercise Physiology, 2002) and provided informed consent.
A neutral women’s running trainer was used as a Control condition (Control: Somnio Women’s Pacemaker 2.0, Somnio Inc., 2010). Three distinctly different insole interventions were selected to determine if insole design influenced frontal plane ankle and knee biomechanics. Medial and lateral inserts included wedged inserts with a 4° incline in the heel area on the medial side (Medial Wedge) or lateral side (Lateral Wedge) (Figure 1). These inserts were placed in the running shoes under the footbed. The combined orthotic intervention (Combined Insole) incorporated mechanisms aiming to influence both rearfoot eversion and knee moment. The Combined Insole included a medial support under the medial longitudinal arch, aiming to restrict rearfoot eversion following heel strike, as well as a 5° lateral wedge along the length of the lateral sole and into the forefoot, aiming to restrict the lateral tilt of the foot and subsequent abduction of the lower leg (Combined Insole: Salfordinsole, Incorporating Lateral Wedge Technology, Inc., 2008; Figure 2).
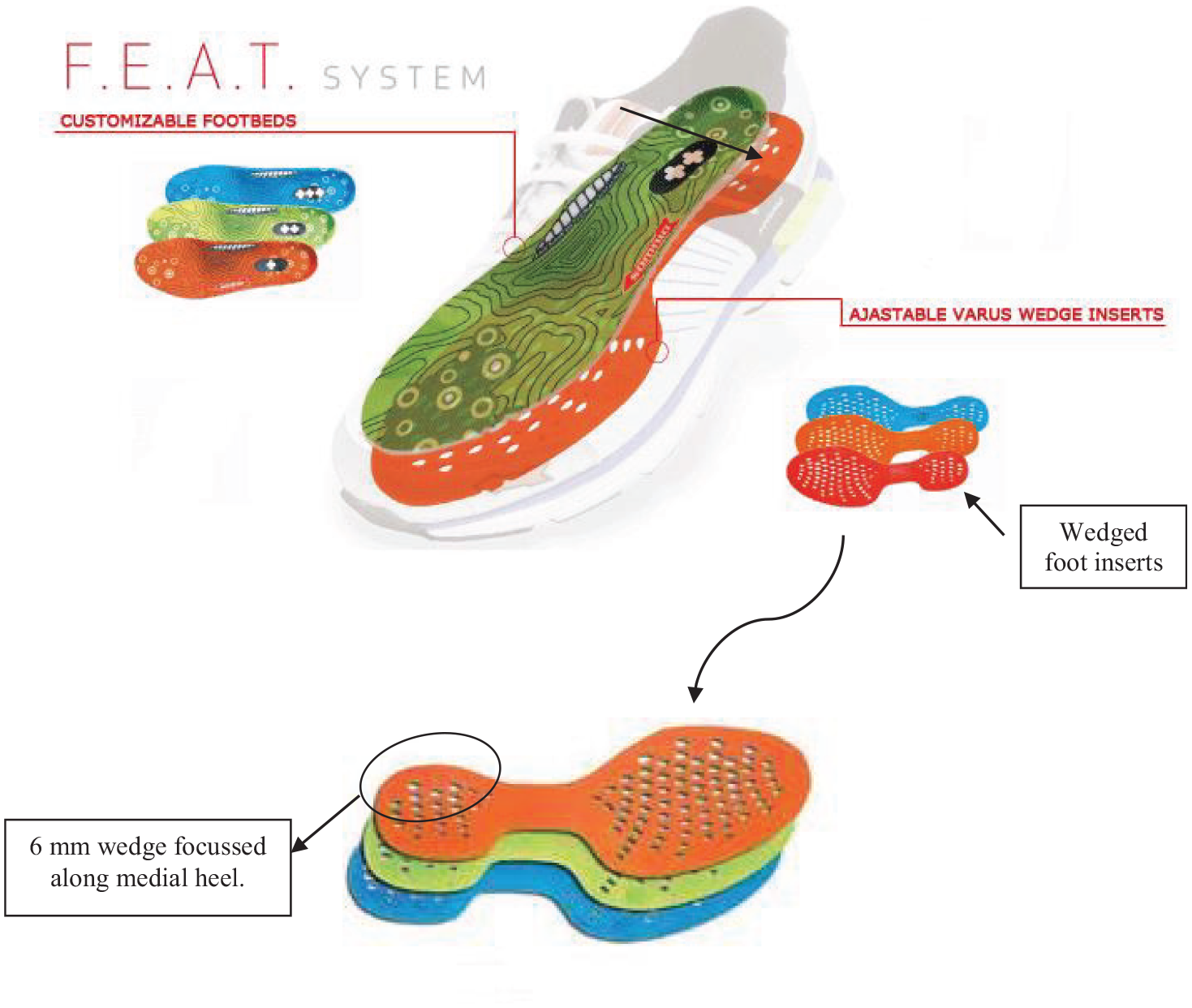
Illustration of the foot beds and 6 mm (4°) wedged inserts added to the shoes.
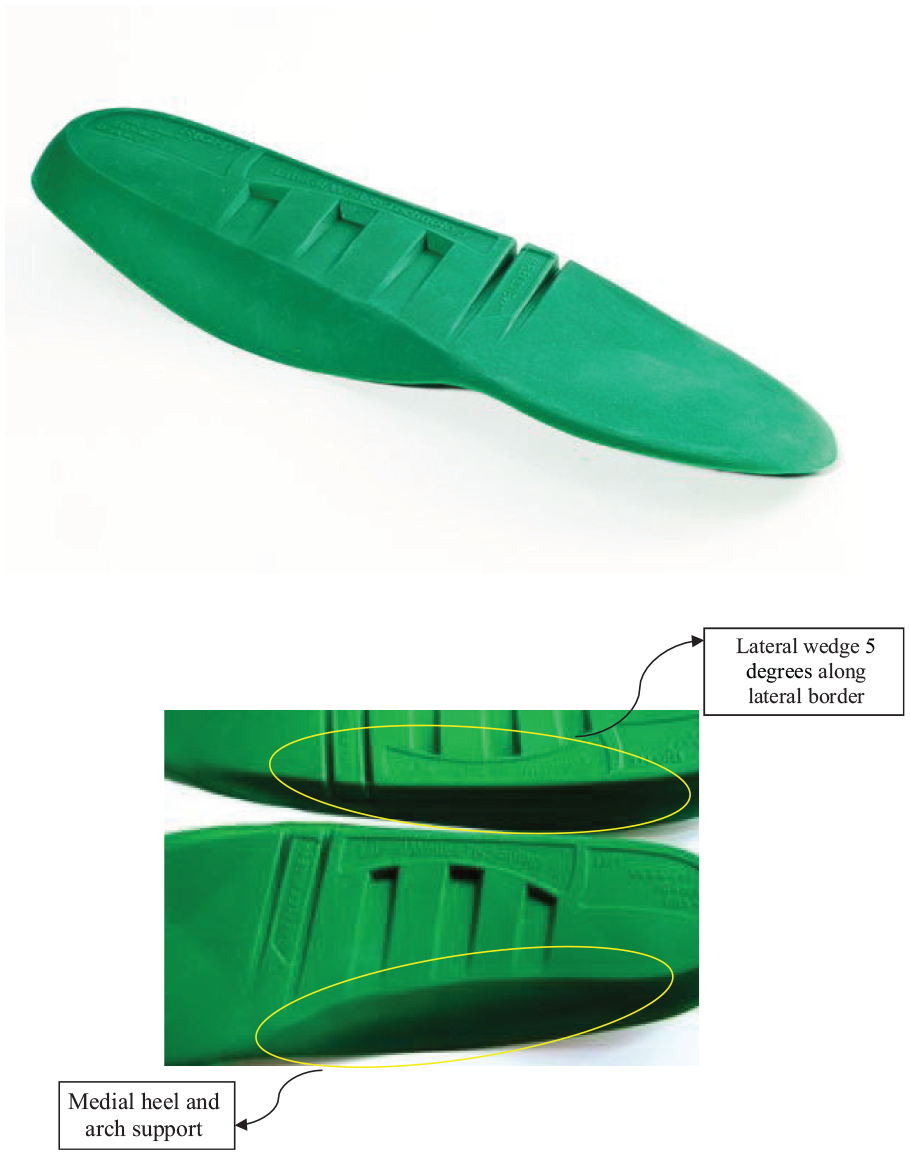
Image of the orthotic intervention, incorporating arch support and lateral wedge technology.
Eleven reflective markers were attached to the right lower limb of each participant and joint angles were defined using a modified version of the model presented by Soutas-Little et al. 22 Three-dimensional lower limb kinematic data were collected using an 8-camera motion capture system (Vicon Peak, 120 Hz, automatic, optoelectronic system; Peak Performance Technologies, Inc., Englewood, CO) synchronised with a single floor mounted force platform (960 Hz, AMTI, Advanced Mechanical Technology, Inc., Watertown, MA). Each participant performed running trials at 3.5 m s−1 ± 5% along a 16 meter runway, striking the force platform with their right foot. This running speed had been identified during pilot work and was monitored using infrared timing gates positioned 1.25 m on either side of the centre of the force plate. Participants performed practice trials to get accustomed with the trial requirements and footwear condition. A successful trial was one which had the right foot contact the force plate cleanly while achieving the required running speed. Ten successful trials were collected for each condition, with the test conditions performed in a random order.
Three dimensional ankle and knee joint angles and angular velocities were determined throughout ground contact. The knee external adductor moment was calculated using inverse dynamics using a customised MATLAB code (MathWorks Inc., Natick, MA) and normalised to body mass. Peak rearfoot eversion and knee internal rotation angle and angular velocity, along with knee external adductor moment, were determined for the ground contact phase. For each study variable, ten trial means for each participant were used to obtain group means for each footwear condition, and significant differences between conditions were identified using repeated measures ANOVAs and post hoc Tukey Honest Significant Difference (HSD) tests (p < 0.05).
Results
For the Medial Wedge compared to the Control, there was no change on any of the study variables: peak rearfoot eversion angle and angular velocity, peak knee internal rotation angle and angular velocity, and peak knee external adductor moment (Table 1, p > 0.05). Compared to the Control, the Lateral Wedge insert had no effect on the joint angles of rearfoot eversion or knee internal rotation, or the respective velocities of rotation. This Lateral Wedge intervention influenced the peak knee external adductor moment, with a lower value observed compared to the Control (p < 0.05). For the Combined Insole, the peak rearfoot eversion angle was lower than for all three other footwear conditions (p < 0.05), with a mean reduction of 5.6° compared to the Control. The peak knee internal rotation angle was lower for the Combined Insole than for both the Control and Lateral Wedge (p < 0.05). In addition, the peak velocity of internal rotation was lower when running in the Combined Insole compared to the Control (p < 0.05). For the peak knee external adductor moment, a lower value was detected for the Combined Insole compared to the Control, Medial Wedge and Lateral Wedge (p < 0.05).
Summary of group means (±standard deviation) for study variables, with p-value for the main effect.
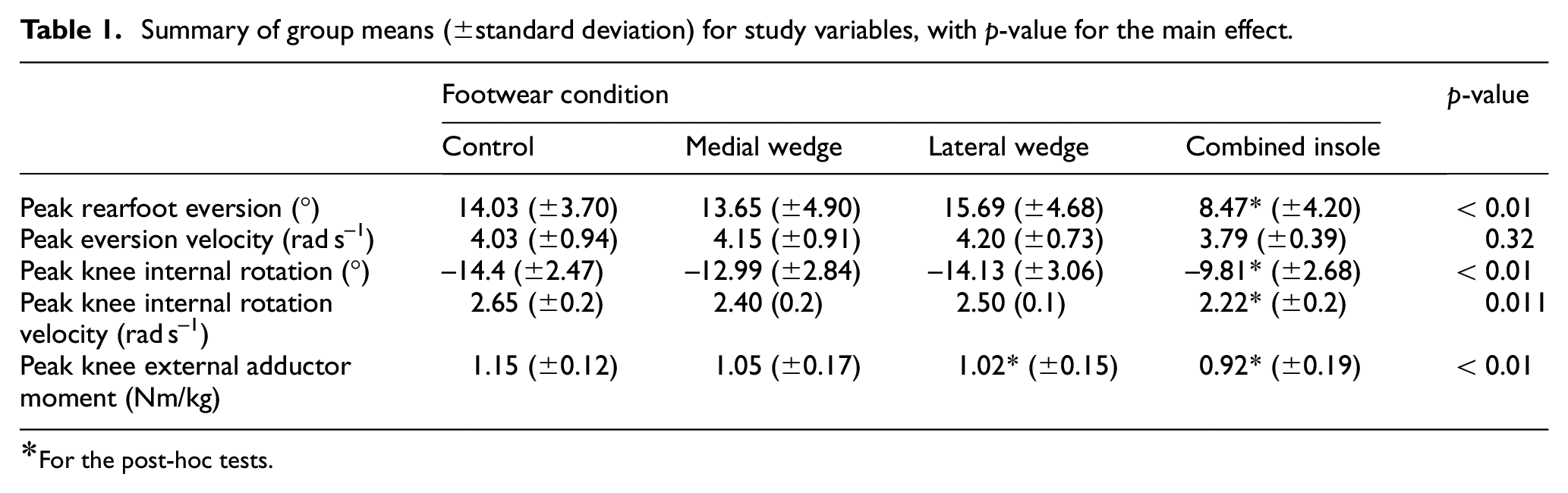
For the post-hoc tests.
Discussion
Following evidence of an increased participation by older females in exercise, and an awareness that this population is likely to develop chronic conditions, this study aimed to investigate the role that footwear interventions might play in influencing biomechanical measures that have been associated with these conditions. In particular, the role of supportive features designed to influence medial-lateral stability was investigated. This study provides new evidence regarding the potential of different footwear supportive inserts to influence biomechanical measures associated with chronic injury and osteoarthritis for older females during running.
The observation that the Medial Wedge intervention did not influence rearfoot eversion angle or angular velocity is in contrast to other research findings where medial support has frequently been reported to reduce rearfoot movement during running,13,23 and does not support the study hypothesis for this condition. Whilst medial support has been demonstrated to be a potential intervention for control of rearfoot eversion, the success of this type of intervention will depend on the specific geometry and material of the insert. For example, Braga et al. 24 argued that 4° and 5° of medial wedging may explain inconsistent reports in the literature regarding the effectiveness of medial wedging, and suggested a greater amount (7°) was required to reliably reduce peak eversion. It is therefore suggested that the lack of difference for this intervention is a result of the relatively low thickness and inclination (6 mm and 4°) of the wedge and the location only in the rear area of the shoe. These characteristics are not sufficient to elicit a significant change in rearfoot motion for the study population during running.
The hypothesis that the Medial Wedge would increase the knee external adductor moment has not been supported, with no change observed for this variable. This suggests that, whilst the intended effect of reduced rearfoot eversion has not been achieved with this insert, there is no detrimental effect on the knee moment. Comparison of this result with literature evidence for walking highlights the importance of considering the severity of the medial intervention, where a 14° medial wedge was found to increase the knee external adductor moment, 25 whereas a 10° medial wedge had no effect on the knee external adductor moment compared to the neutral condition. 26 It is therefore suggested that the relatively small 6 mm thickness of the medial insert in the current study was not sufficient to influence the knee external adductor moment. An alternative to using a medial wedge at the heel is to provide a medial arch support, with this intervention reported to increase peak external adductor moment in running. 27 Based on the results for the Medial Wedge in the current study, this specific condition cannot be recommended for control of rearfoot eversion. Whilst a greater degree of wedging or an arch support may reduce this variable, it should be determined whether an undesirable increase in the knee external adductor moment occurs, particularly for footwear targeted at older female runners.
The observed reduction in knee adductor moment with the Lateral Wedge supports the study hypothesis. This is consistent with the walking literature14,28 and running literature where participants have been young male participants,29,30 suggesting that this form of intervention could also be beneficial in older female runners. A lateral wedge will position the foot such that it is tilted laterally compared to a neutral condition, an orientation contributing to increased rearfoot eversion angle. 28 The possible undesirable effect of increasing rearfoot eversion with the Lateral Wedge, as reported in previous studies of walking31,32 and running, 33 was not detected in this study, conflicting with the study hypothesis for this measure. This lack of influence on rearfoot angle occurs despite the wedge being sufficient to reduce the adductor moment. It is suggested that the lateral wedge has tilted both the rearfoot and lower leg medially, resulting in the knee joint centre moving medially, thus contributing to a reduced lever arm length of the ground reaction force. However, since the rearfoot eversion angle is determined as the angle between the rearfoot and lower leg, this relative angle is not increased by the intervention. Whilst the Lateral Wedge has been found to have the desired effect of reducing the peak knee adductor moment when introduced as an acute intervention, the long term use should be explored before recommending such an intervention. Reports of discomfort when lateral wedge inserts are used during walking has led to low adherence with this intervention,34,35 and running with such a device may also negatively impact comfort. The addition of medial support is suggested as an approach to reduce these negative effects. 36
For the Combined Insole in the current study, the reduced peak rearfoot eversion and internal knee rotation compared to the Control condition supports the study hypothesis. The reduced eversion is attributed to the medial arch support provided by this device and supports much literature evidence regarding the role of medial support in reducing peak rearfoot movement in running.23,37 However, observations from a number of studies where no change in this variable has been identified with changes in medial support38,39 highlights the importance of considering the specific study population and characteristics of the insert design. The design of the Combined Insole in the current study includes a lateral wedge, which might be expected to position the foot in a less inverted/more everted orientation. However, the inclusion of a lateral wedge along the length of the device did not negate the effect of the medial arch support in reducing rearfoot eversion in older female runners. This finding is consistent with the results of Nakajima et al., 36 who showed that a combined orthotic, similar to the one worn in this study, produced a reduction in rearfoot eversion. The lack of effect of a lateral wedge insert on lower limb joint angles has also been demonstrated by Kakihana et al., 16 who reported a lateral movement of the centre of pressure, but no difference in angles at the ankle and knee. It is likely that the location and form of the medial and lateral support are influential on this ability to reduce peak rearfoot eversion, despite the presence of a lateral wedge. Overall, the results regarding rearfoot eversion and internal knee rotation for the Combined Insole device support this as a potential strategy for reducing these measures in older female runners, a population which has been reported to exhibit high magnitude for these variables.
The observed reduction in knee external adductor moment for the Combined Insole compared to the Control is consistent with that reported in previous studies 20 and other lateral wedge insole devices,14,16 and can be attributed to the specific design feature of a 5° lateral wedge along the length of the lateral foot. Whilst lateral wedge insole devices have been demonstrated to be beneficial for reducing knee external adductor moment in walking, 28 the potential application of this type of intervention in running has not been extensively investigated, especially for older female runners. Studies of young males have reported reductions in knee external adductor moment.29,30 The current study has demonstrated that for older female runners, this Combined Insole provides an approach for reducing both the peak rearfoot eversion and knee external adductor moment.
In conclusion, this study has demonstrated the potential of a commercially available lateral wedge orthotic insole developed for control of knee loading and rearfoot eversion during walking to be adopted for reduction of frontal plane knee moment for older females during running, whilst simultaneously reducing the amount of rearfoot eversion. Since high values of these variables have been associated with lower limb injuries and osteoarthritis, this suggests that insoles (and footwear) with these design characteristics may be beneficial for reducing the development of these conditions in older female runners. By also considering the role of isolated lateral and isolated medial wedging on the study variables, this study has also explored the relative role of these design characteristics. If aiming to reduce knee external adductor moment alone, then the 4° lateral wedge technology employed in this study provides an effective method for older female runners, without having any adverse effect on peak rearfoot eversion.
Footnotes
Acknowledgements
We thank SalfordinsolesTM for donation of the insole samples for use in this study.
Author contributions
KL performed data collection, analysis and interpretation as part of a PhD thesis. VS acted as PhD supervisor and contributed to data interpretation and writing. SD acted as PhD supervisor and contributed to data interpretation and writing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: There are no known conflicting interests. This work was performed when Kim Lilley was a PhD student at University of Exeter.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support of the PhD project was provided by University of Exeter.