
Abstract

Dear editor,
Tuberculosis (TB) remains a public health burden despite the collective global efforts to reduce TB-related morbidity and mortality. Emerging evidence shows that despite a microbiologic cure, individuals treated for TB continue to face health challenges, particularly cardiovascular complications. 1 Although TB is primarily a lung disease, several cardiovascular complications are associated with TB, resulting from the organism, the drugs, host immune response to TB, or the effect of TB on the lungs. 2 In settings with high HIV and TB prevalence, cardiovascular diseases (CVD) are associated with increased mortality rates and reduced quality of life.3,4 Unfortunately, low-income countries have a limited capacity to investigate CVD. Advanced diagnostic techniques such as cardiac catheterization are expensive and not readily available. In this context, an electrocardiogram (ECG) is crucial.
We analyzed data from an ongoing cohort study at a tertiary hospital in Uganda as detailed elsewhere.5,6 We recorded patient pretreatment demographics, comorbidities, physical examination findings, and treatment outcomes. At TB cure, spirometry was performed by a trained technician using standardized equipment (ndd, Andover, MA, USA). ECGs were performed and interpreted by a cardiologist (P.K.) who was blinded to the participants’ lung function. Each ECG was marked as normal or abnormal with specific descriptions of changes, conduction, or rhythm abnormalities. We used multivariable logistic regression to evaluate whether lung function was independently associated with ECG abnormalities at TB cure, adjusting for age, sex, HIV status, and smoking history using STATA v.17 (StataCorp LLC, TX, USA).
We enrolled 96 participants, 67 (70%) were male and the mean age was 41.3 ± 15.0 years. Of these, 37 (38%) had abnormal ECGs, with rhythm abnormalities 23 (62%) being most common, while ischemic features were observed in 4 (11%). Participants with abnormal ECGs were older (47 ± 18 years vs 38 ± 11 years, p = 0.003), had a longer duration of respiratory symptoms (87 ± 81 days vs 54 ± 41 days, p = 0.042), and poorer lung function at TB cure, with significant associations between abnormal ECGs and reduced forced expiratory volume in one second (FEV1; p = 0.043) and forced vital capacity (FVC; p = 0.032; Table 1). Multivariable regression showed a small statistically insignificant decrease in the odds of abnormal ECGs among patients with long-standing respiratory symptoms (adjusted odds ratio: 0.99, 95% CI: 0.98–1.00, p = 0.03).
Participant characteristics by ECG abnormality.
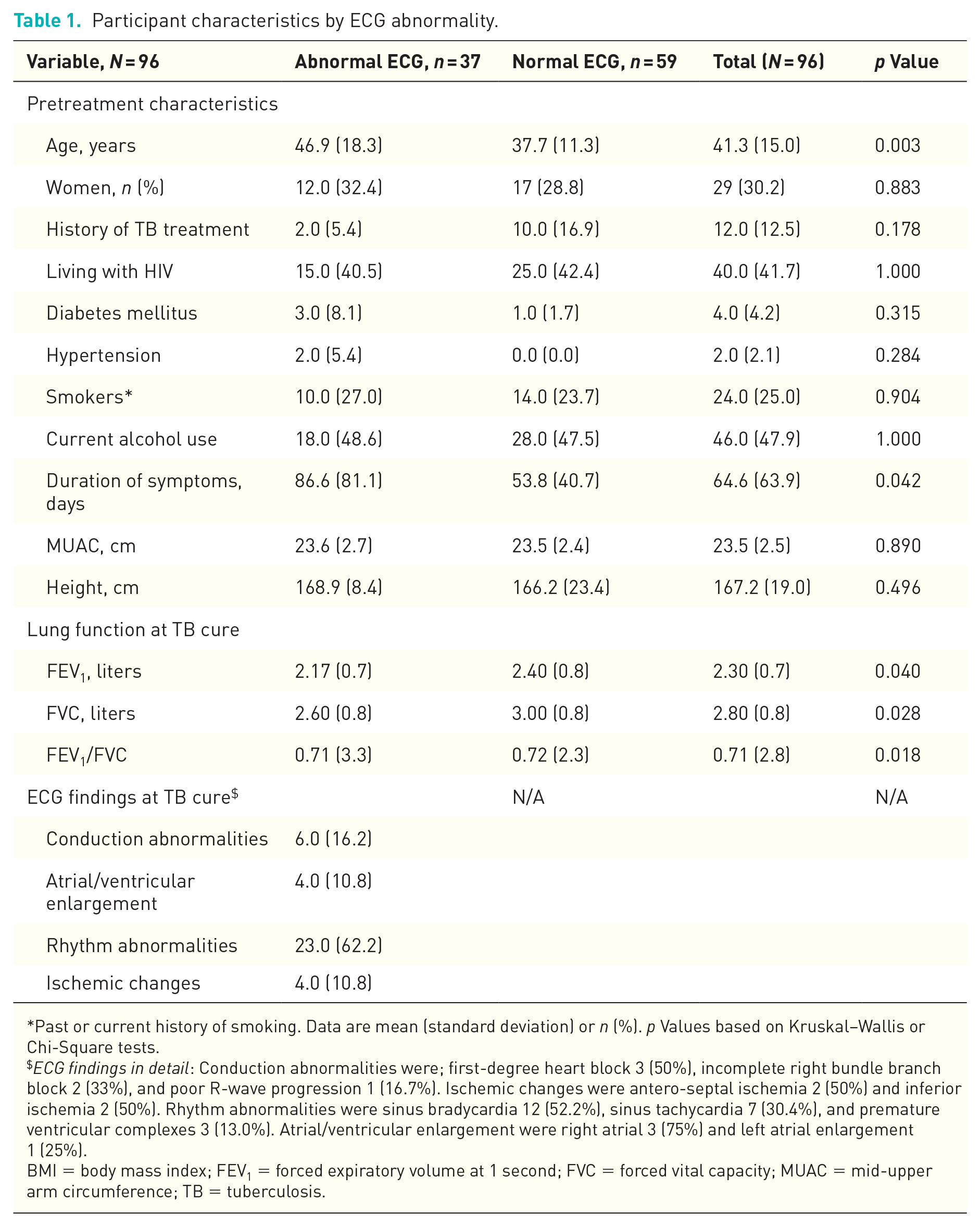
Past or current history of smoking. Data are mean (standard deviation) or n (%). p Values based on Kruskal–Wallis or Chi-Square tests.
ECG findings in detail: Conduction abnormalities were; first-degree heart block 3 (50%), incomplete right bundle branch block 2 (33%), and poor R-wave progression 1 (16.7%). Ischemic changes were antero-septal ischemia 2 (50%) and inferior ischemia 2 (50%). Rhythm abnormalities were sinus bradycardia 12 (52.2%), sinus tachycardia 7 (30.4%), and premature ventricular complexes 3 (13.0%). Atrial/ventricular enlargement were right atrial 3 (75%) and left atrial enlargement 1 (25%).
BMI = body mass index; FEV1 = forced expiratory volume at 1 second; FVC = forced vital capacity; MUAC = mid-upper arm circumference; TB = tuberculosis.
Our findings highlight early cardiovascular abnormalities in TB survivors, which are important for understanding long-term health risks in this population. Screening for CVD is essential, and while ECG may not be a standalone screening tool, it can complement other risk assessment strategies, particularly in resource-limited settings. Despite the age difference in TB survivors with ECG abnormalities, previous studies have shown that in adults aged 40–50 years in sub-Saharan Africa, the prevalence of nonspecific ECG changes can range from 15 to 30%, often influenced by comorbidities. 7 The relatively low rate of ischemic changes (11%) in our cohort suggests that these abnormalities may not be solely attributable to age. Larger cohort studies are needed to develop CVD screening tools for TB survivors in resource-limited settings.