
Abstract
Objective:
The goal of this study was to compare the computed tomography angiography scans of the segmentation results from the Cvpilot, 3mensio, and Volume Viewer systems to explore the practicability of the Cvpilot system in the automatic segmentation and technical evaluation of the aortic root before transcatheter aortic valve replacement (TAVR).
Design:
A total of 154 patients who underwent TAVR at our center from January 2022 to May 2023 were enrolled, and their computed tomography angiography images were analyzed using the Cvpilot, 3mensio, and Volume Viewer systems, respectively.
Setting:
Not applicable.
Participants:
Not applicable.
Main outcome measures:
The reconstructed computed tomography angiography images were evaluated by experts, and the measurements of the aortic roots were analyzed statistically.
Results:
Compared with the 3mensio system, 92.2% of patients (n = 142) evaluated with the Cvpilot system reached grade A, 5.2% of patients (n = 8) reached grade B, and 2.6% of patients (n = 4) reached grade C. Compared with the Volume Viewer system, 90.9% of patients (n = 140) evaluated with the Cvpilot system achieved grade A, 7.1% of patients (n = 11) achieved grade B, and 2.0% of patients (n = 3) achieved grade C. Furthermore, there was no significant difference among the measurement results of the Cvpilot, 3mensio, and Volume Viewer systems (all p > 0.05).
Conclusion:
Overall, the Cvpilot system is effective and reliable. It can accurately complete the segmentation and the measurement of aortic root structures, thereby effectively improving the measurement quality before TAVR.
Trial registration:
Not applicable.
Introduction
The safety and efficacy of transcatheter aortic valve replacement (TAVR) in the treatment of patients with aortic valve (AV) disease have been proven by multiple randomized controlled trials.1 –3 Thus far, TAVR has been widely used as an alternative to surgical AV replacement for these patients. In preprocedural imaging evaluation, computed tomography angiography (CTA), one of the main conventional evaluation methods, plays an important role in identifying anatomical structures, determining the prosthesis type, and predicting main periprocedural complications. Nowadays, CTA assessment before a procedure is completed mainly using the 3mensio (Pie Medical, Maastricht, the Netherlands) or the Volume Viewer system (Siemens Healthineers, Erlangen, Germany). 4 In addition to software operations by professional engineers, the evaluation of data is not only time-consuming but also introduces certain errors that decrease the quality of TAVR. 4 At present, only a few practical software programs are available that provide fast and accurate automatic segmentation and evaluation of the aortic root in TAVR patients through deep learning (DL). The goal of this study was to evaluate the outcomes of CTA scan analyses using the Cvpilot (TAVIgator Co., Ltd., Nanjing, China), 3mensio, and Volume Viewer systems to explore the practicability of the Cvpilot system in the automatic segmentation and clinical evaluation of the aortic root before TAVR.
Methods
Study design and population
This retrospective single-center study included 161 patients who underwent TAVR from January 2022 to May 2023 in the Nanjing First Hospital. The inclusion criteria were (1) ⩾ moderate symptomatic aortic stenosis (AS) with an effective orifice area <1.0 cm2; (2) a mean pressure gradient ⩾40 mmHg (1 mmHg = 0.133 kPa); and (3) New York Heart Association functional class ⩾ III. The exclusion criteria were (1) preprocedural CTA showing that the aortic root diameter was ⩾40 mm; (2) life expectancy <1 year; (3) an acute myocardial infarction that occurred within 1 month; (4) hypertrophic obstructive cardiomyopathy; (5) transesophageal echocardiography showing left ventricular outflow tract obstruction, intraventricular thrombus, or neoplasm; (6) complicated with infective endocarditis; and (7) other situations that were not suitable for TAVR. Meanwhile, seven patients were excluded because of poor image quality due to artifacts or poor image contrast. Finally, the study analyzed 154 pre-TAVR CTA scans (Figure 1). This study protocol was approved by the ethics committee of our hospital (ethics committee approval No. KY20230106-01-KS-01), and all patient data were desensitized.

Flow chart. A total of 161 patients who underwent TAVR were enrolled in this study. After the quality of the computed tomography angiography scans was checked, seven scans were excluded. Every scan was assessed by Cvpilot, 3mensio, and Volume Viewer, respectively. The image quality and measurement results were evaluated.
Preprocedural assessment
3mensio and Volume Viewer systems
The dual-source CT scanner (Definition Flash; Siemens Healthcare, Florsheim, Germany) was used in this study. Structural cardiologists use 3mensio workstations or the Volume Viewer system for preprocedural reconstruction. All CT images were in Digital Imaging and Communications in Medicine (DICOM) format and were transferred to the two systems, respectively (Figure 2(a)–(i)).

Comparison of reconstruction results among the Cvpilot, 3mensio, and Volume Viewer systems. (a–c) Original computed tomography angiography images. (d–f) Reconstruction images of the 3mensio system. (g–i) Reconstruction images of the Volume Viewer system. (j–l) Reconstruction images of the Cvpilot system.
Cvpilot system
Automatic segmentation and measurements were performed using the certified software (Cvpilot Software; TAVIMercy, Inc., Nanjing, China). Cvpilot software employs AI-driven algorithms to analyze complex anatomical structures, particularly the aorta and AV. Segmentation and analysis are further enhanced using the nnU-Net (No New U-Net) framework, a self-adaptive neural network architecture specifically designed for medical image segmentation. The model was reinforced through training focused on the aortic root, enabling detailed extraction of anatomical features, forming the analytical basis of this project. Under the guidance of a professional engineer, all CTA image sequences were assessed directly by radiologists using the Cvpilot system (Figure 2(j)–(l)). 5 Assessment structures included leaflets, calcification, left ventricle, and ascending aorta.
Image and measurement quality evaluation
The image evaluation criteria were as previously mentioned. 5 Results were assessed by structural cardiologist-1 (6.7 years of professional experience) and reassessed by structural cardiologist-2 (12.3 years of professional experience).
Measurement evaluation of aortic root parameters
The measurement results among the three systems were compared. The measured parameters included the mean annulus diameter, the mean left ventricular outflow tract diameter, the mean sinus tubular junction diameter, and the heights of the left and right coronary arteries. In addition, the measurement results of the 3mensio and Volume Viewer systems were averaged by measurements from expert-1 and expert-2.
Calcification burden assessment
We measured the calcification burden of the aortic root in each patient using three types of systems. The total volume of the voxels in the calcification segmentation results with an intensity higher than 850 HU was defined as the calcification volume.
Software efficiency evaluation
To accurately calculate the manual effort of evaluating the three systems, Mousotron Software (Blacksun Software, Turnhout, Belgium) was used to track and record mouse movements. We also recorded the total time it took each of the three systems to complete the evaluation.
Statistical analyses
All statistical analyses were performed using SPSS version 26.0 (IBM-SPSS Inc., Armonk, NY, USA). The Kolmogorov-Smirnov test was used to evaluate the normality of the distribution. The measurement data conforming to normal distribution were represented by mean ± standard deviation, and the continuous variables of normal distribution were compared by analysis of variance. The results of the categorical data were expressed as n (%), and the categorical variables were compared using Fisher’s exact test. Bilateral p values <0.05 were considered statistically significant.
Results
Baseline characteristics
A total of 154 retrospective patients subjected to CTA of the aorta were included in this study. The patient’s baseline characteristics are shown in Table 1. A total of 55.2% of the patients (n = 85) were male, and the average age was 71.9 ± 7.3 years. Furthermore, 44.2% of the patients (n = 68) had pure AS, and 55.8% of the patients (n = 86) also had aortic regurgitation. In addition, 61.0% (n = 94) of the patients had severe AS, and 21.4% (n = 33) had bicuspid AV.
Baseline characteristics.

Structural cardiologist rating outcomes
Compared with the 3mensio system, 92.2% of patients (n = 142) evaluated with the Cvpilot system reached grade A, 5.2% of the patients (n = 8) reached grade B, and 2.6% of patients (n = 4) reached grade C. Compared with the Volume Viewer system, 90.9% of patients (n = 140) evaluated with the Cvpilot system achieved grade A, 7.1% of patients (n = 11) achieved grade B, and 2.0% of patients (n = 3) achieved grade C (Figure 3).

The outcomes of Cvpilot image quality ratings compared to the 3mensio and the Volume Viewer system.
As expected, the leaflet boundaries were clear and the calcification distributions were ideal in patients who achieved grade A. In 19 cases of grade B, the reason for the slightly poor assessment results was the small artifacts in the CTA scans, which in turn led to a slight decrease in reconstruction quality. However, of the rare seven cases of grade C, five cases exhibited over-segmentation of the leaflets that resulted from artifacts, and the other two patients had inadequate segmentation due to severe calcification.
Measurements outcomes
The measurement results of the three systems are displayed in Figure 4. Compared with the 3mensio and the Volume Viewer systems, the Cvpilot system achieved the results of the mean annular diameter (24.4 ± 4.0 vs 24.5 ± 4.2 vs 24.5 ± 3.9, p = 0.567); the mean left ventricular outflow tract diameter (25.2 ± 4.3 vs 25.5 ± 5.0 vs 25.4 ± 4.7, p = 0.131); the mean sinus tubular junction diameter (30.5 ± 5.8 vs 30.6 ± 6.3 vs 30.5 ± 5.5, p = 0.433); the mean left coronary artery height (12.3 ± 2.9 vs 12.3 ± 3.0 vs 12.3 ± 3.3, p = 0.748); and the mean right coronary artery height (17.7 ± 4.2 vs 17.7 ± 3.9 vs 17.7 ± 4.1, p = 0.692), which showed a good correlation with no significant statistical differences.
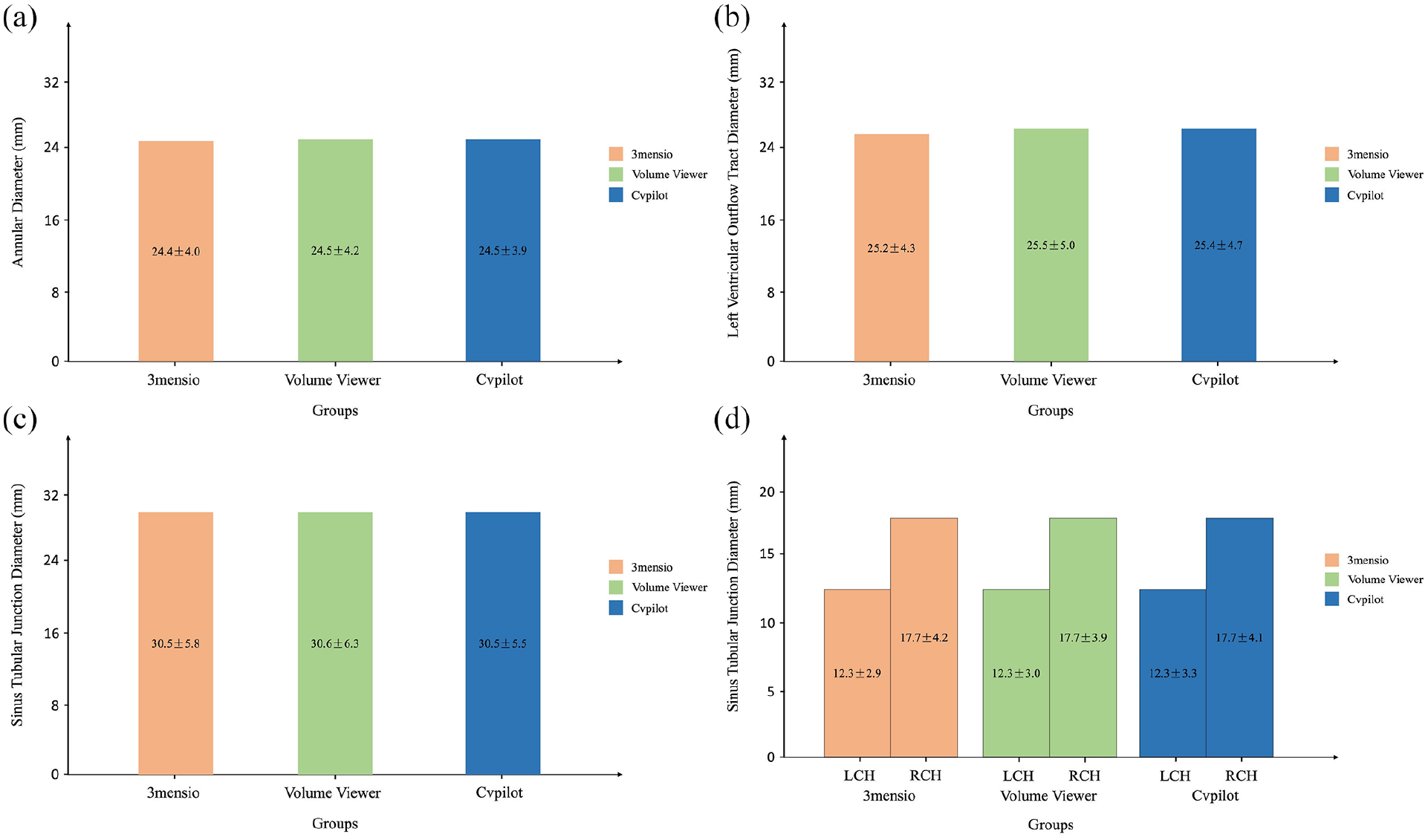
Comparison of measurements among the 3mensio, Volume Viewer, and the Cvpilot systems. (a) Annular diameter, (b) left ventricular outflow tract diameter, (c) sinus tubular junction diameter, and (d) left and right coronary artery heights.
Calcification burden assessment outcomes
We evaluated the robustness of the Cvpilot system in the assessment of the calcification volume of the aortic root (Figure 5). The calcification volumes measured by the 3mensio, Volume Viewer and the Cvpilot system on the supra-annular plane (flap plane 4 mm; 216.5 ± 78.2 mm3 vs 226.1 ± 64.4 mm3 vs 207.6 ± 75.3 mm3, p = 0.373), the annular plane (1133.8 ± 639.6 mm3 vs 1083.5 ± 673.0 mm3 vs 1040.4 ± 711.2 mm3, p = 0.421), the left ventricular outflow tract plane (12.0 ± 8.3 mm3 vs 12.9 ± 7.6 mm3 vs 12.0 ± 9.2 mm3, p = 0.784), and the leaflets (546.2 ± 307.8 mm3 vs 526.0 ± 344.9 mm3 vs 562.3 ± 412.0 mm3, p = 0.536) were not statistically significant. If the annular calcification was extensive and severe, it might slightly affect the measurement accuracy of the Cvpilot system, but it was still within the acceptable range.

Comparison of calcification volumes among the 3mensio, Volume Viewer, and Cvpilot systems. (a) Super-annular plane, (b) annular plane, (c) left ventricular outflow tract plane, and (d) leaflet plane.
Software efficiency evaluation outcomes
We collected the total time and mouse movement distance required for measurement evaluation using the Cvpilot, the 3mensio, and the Volume Viewer systems, respectively. Among these, compared with the results of manual measurement by the 3mensio system, the total times taken by the Cvpilot system to complete the automatic measurement and the total mouse movement distance were significantly reduced (1.0 ± 0.8 min vs 17.7 ± 6.6 min, p < 0.001; 63.2 ± 25.7 m vs 372.1 ± 114.5 m, p < 0.001; Figure 6). Meanwhile, the reductions were also observed when comparing the Cvpilot system and Volume Viewer system (1.0 ± 0.8 min vs 18.4 ± 6.9 min, p < 0.001; 63.2 ± 25.7 m vs 381.9 ± 151.6 m, p < 0.001; Figure 6). The results show that the Cvpilot system can help surgeons improve work efficiency and reduce the workload of preprocedural evaluation.

Comparison of measurement efficiency evaluation outcomes. (a) Evaluation total time, and (b) mouse movement distance.
Discussion
Our goal was to segment and evaluate the aortic root anatomy in CTA scans using the Cvpilot system based on a DL algorithm. Compared with the 3mensio and the Volume Viewer systems, the Cvpilot system can reliably segment the aortic root and accurately measure main anatomical structures, so it has important clinical value and significance.
Combined with the current trend of global pre-TAVR evaluation, artificial intelligence (AI), especially DL, has become a hot topic. Compared with traditional algorithms, DL has achieved obvious advantages in terms of segmentation accuracy, algorithm generalization, and arithmetic speed. 6 In particular, the neural network architecture represented by the convolutional neural network has become a technical cornerstone for image segmentation, target detection, and template matching.7,8 An AI diagnostic system is not only solely image-oriented but also provides diagnostic suggestions based on appropriate images, which may greatly improve the efficacy and quality of imaging evaluations.7,8
However, in the field of TAVR, most DL applications are early exploratory in nature. Astudillo et al. 9 proposed using convolutional neural networks to detect and locate the sinuses and the coronary arteries. Meyer et al. 10 confirmed the accuracy of machine learning in TAVR by comparing semiautomatic and fully automatic segmentation software. The preceding researchers conducted preliminary explorations of the complex anatomical structures of the aortic root, but there were some limitations such as lack of leaflet phenotype, incomplete segmentation, and poor accuracy of anatomical parameters.
The results of this study show that the Cvpilot system, which is based on nnU-Net, can accurately segment the aortic root structures and complete accurate measurements of the main anatomical positions. On one hand, compared with the results of the 3mensio and the Volume Viewer systems, 92.2% and 90.9% of the Cvpilot system CTA scans reached grade A of the reconstruction quality, showing good reliability in the initial clinical application. Furthermore, the reason for the slightly poor assessment results of the 19 grade B cases was the small artifacts in the CTA scans, which in turn led to a slight decrease in reconstruction. On the other hand, the main anatomical positions measured by the Cvpilot system were similar to those measured by the 3mensio and Volume Viewer systems, further suggesting that the Cvpilot system may play a more important role in the pre-TAVR evaluations.
There are some limitations to this study. First, this was a retrospective study. Therefore, inherent selection bias was unavoidable. In the next step, we plan to conduct prospective studies to verify the reliability of this study. Second, the study only included data from a single center, which limited its clinical generalization. Third, we focused on the reproducibility and measurement accuracy of Cvpilot in this study. In the future, we plan to develop this algorithm for pre-TAVR strategy formulation and complication prediction to further enhance its clinical value.
Conclusion
Compared with traditional volume mapping methods and manual labeling methods, our results show that the Cvpilot system can clearly display aortic root structures. The nnU-Net-based DL segmentation is the current advanced medical segmentation model, and the system has shown strong versatility in evaluating patients with bicuspid or tricuspid AV diseases. The results of this study demonstrate that the Cvpilot system provides rapid reconstruction and accurate visualization that will play an important role in pre-TAVR measurements. In addition, the system provides a feasible solution for processing AV structures quickly and accurately, which may further benefit patients with AV diseases in the future.