
Abstract
Background:
Our aim was to review the current literature of the use of directional atherectomy (DA) in the treatment of lower extremity critical-limb ischemia.
Methods:
A search for relevant literature was performed in PubMed and PubMed Central on 16 April 2020, sorted by best match. Three searches across two databases were performed. Articles were included that contained clinical and procedural data of DA interventions in lower extremity critical-limb ischemia patients. All studies that were systematic reviews were excluded.
Results:
Eleven papers were included in this review. Papers were examined under several parameters: primary patency and secondary patency, limb salvage/amputation, technical/procedural success, complications/periprocedural events, and mean lesion length. Primary and secondary patency rates ranged from 56.3% to 95.0% and 76.4% to 100%, respectively. Limb salvage rates ranged from 69% to 100%. Lesion lengths were highly varied, representing a broad population, ranging from 30 ± 33 mm to 142.4 ± 107.9 mm.
Conclusions:
DA may be a useful tool in the treatment of lower extremity critical-limb ischemia.
Introduction
Peripheral artery disease (PAD) is an atherosclerotic disease of the lower limbs that affects over 200 million people worldwide.1–4 PAD is uncommon in younger populations but its prevalence rises sharply with increasing age to approximately 30% of men and 40% of women above the age of 80. 4 PAD has placed a considerable burden on the American healthcare system, which will only increase due to the rising proportion of the American population developing key risk factors for PAD such as diabetes mellitus, hypertension, dyslipidemia, and obesity.1,3 The American healthcare system spent $4.37 billion on PAD-related treatment in 2001. 5 Many PAD patients are asymptomatic but symptomatic patients present with symptoms ranging from lifestyle-limiting claudication to critical-limb ischemia (CLI).2,6,7
CLI, defined clinically as ischemic rest pain, tissue loss, or gangrene in the presence of PAD and hypoperfusion of the lower extremity, is associated with significant mortality, morbidity, and increased use of healthcare resources.8,9 CLI represents the most advanced form of PAD and currently encapsulates 1–3% of all PAD patients. 10 Left untreated, CLI patients can lose their limbs or suffer from complications such as gangrene and sepsis. 11 Across all patients with PAD, there is a 30–50% occurrence of cardiovascular events including myocardial infarction and stroke over a 5-year period. 12 Patients with CLI however, face the same risk over a 1-year period. 12 Additionally, the risk of major amputation at or above the ankle is less than 5% in claudicant patients over 5–10 years; it is 30–50% in the first year for CLI patients who are not revascularized. 12 The rate of primary amputation in CLI patients is 25%, increasing to 30% at 1 year. 13 Therefore, this subgroup of the PAD patient population will become increasingly relevant in the treatment and management of PAD.
Directional atherectomy (DA) has become a popular endovascular technique that is safe and effective in treating patient populations including both claudicants and CLI. 14 DA mechanically removes plaque and debulks vessels without leaving a stent within. 14 The advent of drug-coated balloons (DCBs) have propelled forward the ‘leaving nothing behind’ approach of treatment. 6 Additionally, DCBs have shown superior results compared with plain old balloon angioplasty (POBA) as demonstrated by various clinical trials such as the LEVANT I and II, IN.PACT SFA, and ILLUMENATE treating short- to intermediate-length lesions.15–18
In this systematic review, we aimed to evaluate the body of literature on the clinical outcomes of endovascular interventions utilizing DA in the CLI cohort of PAD patients.
Methods
By using the participant, interventions, comparisons, outcomes, and study design search strategy, an examination of relevant literature was performed in PubMed and PubMed Central (PMC) on 16 April 2020 sorted by best match. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was followed to conduct a study-level systematic review; however, a review protocol did not exist for this specific topic. Detailed here are the specific keyword searches and criteria used to filter search results thereafter. The search terms are in square brackets with the Boolean relationship ‘AND’ or ‘OR’. All searches excluded publications before the year 2000 and used filters for ‘English,’ ‘Humans,’ and ‘Full Text’ in PubMed. No specific filters were utilized for the type of publication such as ‘Clinical Study’ or ‘Systematic Review’ in an effort to include any relevant literature and additional references found therein.
Articles were included that contained clinical and procedural data of DA interventions in CLI patients in the lower extremities or DA used in a combination therapy in CLI patients in the lower extremities. There was no additional contact to authors for acquiring further information. All studies that were systematic reviews were excluded.
The purpose of this search before manual evaluation of article content was to perform a broad search on the current literature of DA in relation to CLI. Upon applying a set of filters (‘English,’ Humans,’ ‘Full Text,’ and a time range of ‘01/01/2000–12/31/2020’) 13 results remained to be independently evaluated. Articles were included if data of CLI patients being treated with DA were presented. This generated four references used in this literature review (Figure 1).
The purpose of this search before manual evaluation of article content was to encapsulate articles that utilize the term ‘critical-limb-threatening ischemia’ (CLTI), another commonly used term in describing PAD patients with ischemic rest pain or tissue loss. Upon applying a set of filters (‘English,’ ‘Humans,’ ‘Full Text,’ and a time range of ‘01/01/2000–12/31/2020’) 175 results remained to be independently evaluated. Articles were included if data of CLI or CLTI patients being treated with DA was presented. This generated one additional reference used in this literature review (Figure 1).
The purpose of this search before manual evaluation of article content was to utilize an extension to the PubMed database to capture any references not found in the first search. Upon applying a time range of ‘01/01/2000–12/31/2020,’ 109 results remained to be independently evaluated. Articles were included if data of CLI patients being treated with DA was presented. This generated an additional six references used in this literature review (Figure 1) bringing the total number of references in this review to 11.

Flowchart of reference selection.
Once individual evaluation was complete, we separated each article’s results according to the outcomes and follow-up period. The categories were as follows: primary and secondary patency, limb salvage/amputation, technical/procedural success, complication/periprocedural events, and mean lesion lengths. We compared each of these study outcomes at equivalent follow-up periods.
An analysis using the Cochrane ROBINS-I assessment tool19 was also utilized to determine overall risk of bias for each article in this study (Table 1).
Risk bias analysis of articles.

N/A, not applicable.
Results
Eleven references were selected for review and discussion from the search detailed in the methods section above. Three searches were performed for this literature review and findings from the references will be presented under the following headings in the results section: primary patency and secondary patency, limb salvage/amputation, technical/procedural success, complications/periprocedural events, and mean lesion length. Table 2 presents the study characteristics extracted from each article, as well as additional information that is relevant to this review.
Characteristics of each study used in this review.

ABI, Ankle Brachial Index; CLI, critical-limb ischemia; DA, directional atherectomy; DCB, drug-coated balloon; PTA, percutaneous transluminal angioplasty.
Primary patency and secondary patency
One of the most critical parameters when evaluating the efficacy of endovascular intervention devices are the primary and secondary patency rates. Of the 11 papers reviewed, 10 discussed primary patency rates at 12 months. Two single-center, single-arm, prospective, non-randomized studies by Stavroulakis et al. 16 and Cioppa et al. 17 examined a combination therapy of DA with DCB in a cohort where patients presented with either lifestyle-limiting claudication or CLI (18 lifestyle-limiting claudication + 3 CLI and 18 lifestyle-limiting claudication + 12 CLI, respectively).20,21 The cohorts in both of these papers were very small, limiting any generalizability of their findings. In addition, only a small proportion of these already limited cohorts were CLI patients. Stavroulakis et al. 16 showed primary patency at 12 months in 19 out of 20 patients (1 patient died in follow up) and showed secondary patency in all patients throughout the study. 20 Cioppa et al. 17 showed primary patency in 27 of the 30 patients and secondary patency in all 30 at 12 months. 21 Unfortunately, only the overall primary patency rate was presented for the entire cohort. There was no distinction made between claudication and CLI patients. A largescale retrospective review of a prospectively maintained database by Gallagher et al. 18 examined 304 CLI patients who presented with superficial femoral artery (SFA) lesions. 22 Depending on the location of the lesion, primary patency rates at 12 months and 24 months for CLI patients ranged from 37.8% ± 7.1% to 56.3% ± 5.3% and 21.6% ± 6.5% to 49.3% ± 6.0%. 22 Secondary patency at 12 months and 24 months ranged from 70.2% ± 4.9% to 83.1% ± 6.9%, and 61.8% ± 7.5% to 73.9% ± 8.7%, respectively. 22 Out of the 799 included subjects in the DEFINITIVE LE trial by McKinsey et al., 14 201 were CLI patients. Depending on the lesion location, primary patency at 12 months ranged from 67% to 78%, and secondary patency at 12 months was 88%. 14 In a study by Zeller et al., 20 19 of the 36 subjects treated with DA had CLI and reported 12- and 24-month primary and secondary patency rates (67% and 91%; 60% and 80%, respectively). 23 Semaan et al. 21 conducted a retrospective review of 56 patients who received endovascular revascularization. 24 Of the 56, 18 received DA with 12 of those treated with DA presenting with CLI. 24 Among patients who were treated with DA there was a 75% 12-month primary patency rate. 24 A prospective study of 18 consecutive CLI patients from March 2012 to March 2013 by Bracale et al. 22 reported a 12-month primary and secondary patency rate of 83.3% and 94.4%, respectively. 25 Within a CLI subject cohort of 99 patients, Loor et al. 23 reported a 12-month primary patency rate of 63% in 33 subjects treated with DA. 26 Patients treated with DA from August 2004 to January 2006 were enrolled into a prospective database by Keeling et al. 24 that included 70 plaque excisions across 66 patients. 27 Twenty-five excisions occurred within a limb considered to be critically ischemic. 27 Across the entire cohort, 12-month primary and secondary patency rate was 61.7% and 76.4%, respectively. 27 Upon conducting a retrospective review of 480 tibial interventions across 421 patients, Todd et al. 25 examined 418 CLI interventions, of which 79 were treated with atherectomy, and 13 with DA specifically. 28 Primary and secondary patency rates are reported only for the atherectomy group as a whole (61% and 95%, respectively). 28 The primary and secondary patency rates at 12 months are detailed below in Figure 2.

Comparison of primary and secondary patency rates at 12 months (%).
Limb salvage/amputation
Preserving the integrity of the target limbs and preventing amputation in CLI patients is critical in attempting to treat and manage other systemic morbidities exacerbating their PAD. Stavroulakis et al. 16 reported no amputations in their CLI cohort (n = 3) and did not report limb salvage rates. 20 Cioppa et al. 17 reported 12 month 100% (n = 18) limb salvage and 3 minor below-ankle amputations in CLI patients. 21 Gallagher et al. 18 reported limb salvage rates at 12 and 24 months for SFA, popliteal, tibial, and multilevel lesions. In the SFA (n = 76), 12- and 24-month limb salvage rates were 97.1% and 91.2%, respectively. 22 Popliteal (n = 35) limb salvage rates were 87.0% and 78.3% at 12 and 24 months, respectively. 22 The tibial (n = 121) 12- and 24-month limb salvage rates were 79.7% and 77.0%, respectively. 22 Although not significant, DA was superior to POBA or POBA and stenting in limb salvage rates. 22 Multilevel lesions (n = 71) had limb salvage rates of 81.4% and 76.7% at 12 and 24 months, respectively. 22 McKinsey et al. 14 reported a 12-month limb salvage rate of 95% in CLI patients (n = 201) and three unplanned amputations in the CLI group. In a comparison of DA (n = 18) and angioplasty (n = 38), Semaan et al. 21 reported no significant differences in limb salvage rates (87% and 97%, respectively). 24 In a similar comparison of DA (n = 20) and angioplasty (n = 15), Tan et al. 26 presented 6-month limb salvage rates of 88% and 78%, respectively. 29 The rates of limb salvage were similar between groups, and no statistical difference was found. Loor et al. 23 reported a significantly higher 12-month limb salvage rate in their surgical bypass group of subjects (n = 59) compared with the DA group (n = 33; 87% versus 69%). 26 In the atherectomy group of the CLI cohort (n = 79) examined by Todd et al. 25 there was a 12-month limb salvage rate of 81%. 28 The available data have been tabulated in Figures 3 and 4.

Limb salvage rates at 12 months (%).

Limb salvage rates by lesion and treatment (Gallagher et al. 18 )
Technical/procedural success
The technical and procedural success of devices is a key parameter in evaluating their safety. Stavroulakis et al. 16 reported a 90% technical success rate, and Cioppa et al. 17 reported a 100% procedural success rate.20,21 McKinsey et al. 14 reported a procedural success rate of 83.0% in CLI patients within the DEFINITIVE LE trial. Semaan et al. 21 reported 94% technical success in DA patients. 24 Tan et al. 26 reported a collective technical success of 93% across DA and angioplasty patients. 29 Bracale et al. 22 reported 100% technical success. 25 Across the 70 plaque excisions presented by Keeling et al. 24 there was a technical success of 87.1%. 27 Todd et al. 25 saw a technical success rate of 98% in the atherectomy group. 28 Gallagher et al., 18 Zeller et al., 20 and Loor et al. 23 did not provide technical or procedural success rates.22,23,26
Complications/periprocedural events
In addition to technical and procedural success rates, the presence or absence of complications or periprocedural events acts as a valuable assessor of the safety of a device or technique being examined. Gallagher et al. 18 reported only an overall complication rate of 6.9% for both claudicant and CLI patients. 22 Stavroulakis et al. 16 reported periprocedural complications in 15% of the cohort. 20 Cioppa et al. 17 reported no complications or periprocedural events. 21 McKinsey et al. 14 reported periprocedural events in 12.9% of the CLI subgroup. Zeller et al. 20 reported a 3% complication rate. 23 Semaan et al. 21 reported thromboembolic events in 22% of the DA group. 24 Tan et al. 26 reported a complications/periprocedural event rate of 58.6% in the DA group; 29 Todd et al. 25 reported a 13% complication rate in their atherectomy group. 28
Mean lesion length
The mean lesion lengths were reported in 9 of the 11 articles reviewed and have been tabulated in Figure 5. For clarity, it is important to note that McKinsey et al., 14 Bracale et al., 22 and Keeling et al. 24 were the only references to report mean lesion length specific to CLI patients.
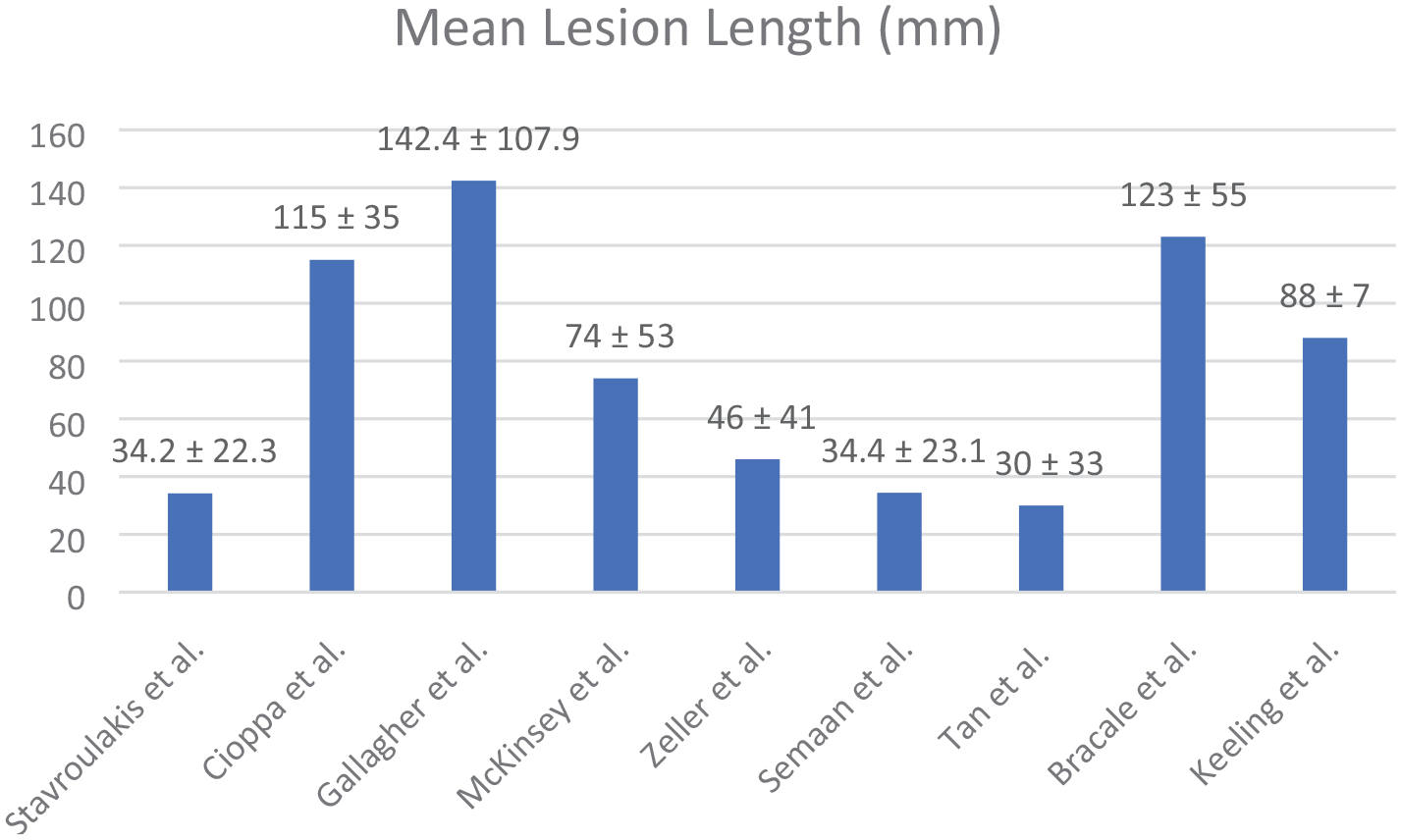
Comparison of mean lesion length (mm).
Discussion
CLI continues to be classified as the most severe complication of PAD, with treatment modalities limited to either endovascular revascularization or open surgical revascularization. The former includes POBA, drug-eluting stents (DES), bare metal stents (BMS) and DCBs, which have all shown safety and efficacy in treating CLI.27–31 However, the effectiveness for DA as an adjunctive or stand-alone treatment for CLI remains to be assessed.
From the current literature, DA as an adjunct to DCB shows positive effects for lower extremity lesions. Stavroulakis et al. 16 and Cioppa et al. 17 who both conducted prospective studies, found higher rates of 12-month primary and secondary patency amongst their patient populations, as well as a higher rate of 12-month limb salvage for subjects with CLI. Furthermore, Stavroulakis et al. 16 and Cioppa et al. 17 reported higher 12-month primary patency rates than the DEFINITIVE AR study (86.7%), which assessed DA as an adjunct to DCB among a population without CLI. 32 While these results may shine greater light on the use of DA with DCB, it is not without mention that both Stavroulakis et al. 16 and Cioppa et al. 17 utilized small study populations, with the former recruiting just three CLI patients.
The remaining nine studies assessed DA as its own treatment modality. Of these articles, Gallagher et al., 18 Todd et al., 25 and the DEFINITIVE LE trial by McKinsey et al. 14 had the largest participant pools. Each study also compared the outcomes with other groups, where Gallagher et al. 18 compared DA with percutaneous transluminal angioplasty (PTA) or PTA with stenting; McKinsey et al. 14 compared DA in claudicants with DA in CLI; and Todd et al. 25 compared DA with angioplasty.
While Gallagher et al. 18 did not notice a difference in first-year outcomes across treatment groups, CLI patients with SFA chronic total occlusions (CTOs) treated with DA had better 2-year outcomes than the angioplasty-alone group. In addition, McKinsey’s DEFINITIVE LE trial determined that DA was safe and effective across in both patients with claudicants or CLI. 14 Only Todd et al. 25 claimed that DA did not provide benefit over angioplasty. While these opinions may differ, the strengths of the McKinsey et al. 14 and Gallagher et al. 18 studies are they analyzed far more patients undergoing atherectomy than Todd et al. 25 (799, 194, and 79, respectively). Additionally, the work by McKinsey et al. 14 is a prospective, single-armed trial that contains the largest cohort of CLI patients treated with DA, while the work by both Gallagher et al. 18 and Todd et al. 25 were retrospective analyses.
Of the remaining articles, each assessed the outcomes of DA in only a small number of CLI patients. Keeling et al., 24 Zeller et al., 20 Semaan et al., 21 and Tan et al. 26 determined that DA was an effective method of treatment for endovascular therapy, but specific outcomes for the patients that had CLI were not discussed. Semaan et al., 21 and Tan et al. 26 were also studies that compared DA with angioplasty, where they concluded both methods were viable PAD treatments. Bracale et al. 22 was a unique study in this review, as they assessed only CLI patients, arriving at the same conclusion previously stated where DA is an effective modality of treatment. Lastly, Loor et al. 23 was the only study that compared DA with bypass surgery, concluding that bypass may provide better outcomes for CLI patients than atherectomy.
With the current evidence, a greater number of studies lean towards the safety and efficacy of DA, but the specific relationship of this technique in regard to CLI requires further exploration. Six of the articles in this review were single-center, single-armed, prospective, non-randomized studies which limits the extent to which meaningful findings can be drawn from the results. The remaining studies were all retrospective analyses, which may contain an inferior level of evidence compared with prospective studies, along with an inherent bias as each investigator reviewed their databases. In addition, while McKinsey’s DEFINITIVE LE trial contained the greatest study population, its non-randomized nature hampered the strength of the evidence provided.
Outside of the DEFINITE LE trial, there are no largescale clinical trials that have examined the efficacy and safety of DA use in treating CLI patients with comprehensive data on key outcomes for CLI patients such as limb salvage rates and amputations. Most studies examine cohorts comprising a combination of claudication and CLI patients, with the latter commonly consisting of fewer subjects. DA presents itself as a potentially useful tool in the treatment of lower extremity CLI; however, additional, focused studies of this cohort are needed.
Limitations
The limitations of this systematic review include inherent bias of the individual studies selected. Many were single-armed, prospective studies, which lacked comparison or control groups. The remaining studies were retrospective, and while they compared different interventions, there was a lack of any randomization. Additionally, different methodologies were followed by each study. Lastly, there was the potential of omitting relevant articles due to our search consisting of only the databases of PMC and PubMed.
Footnotes
Author contributions
All authors contributed in a significant manner to the conception, planning, writing and editing of this manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.