
Abstract
Background:
Although tolvaptan, an electrolyte-free water diuretic for congestive heart failure (HF), is reported to have no effect on long-term mortality or HF-related morbidity, there may exist some subgroups of patients who may receive beneficial effect of tolvaptan. The purpose of this study was to identify clinical factors associated with mid-term effect of tolvaptan on clinical outcomes of patients who discharged after acute HF.
Methods:
We retrospectively analyzed 140 patients (88 male; mean age, 77.1 ± 11.0 years) with acute HF who received tolvaptan (initial dose 8.6 ± 3.6 mg/day) during their hospitalization. They were divided into two groups according to how the tolvaptan was used at discharge; 77 in the tolvaptan-continued group and 63 in the discontinued group.
Results:
The Cox proportional hazards model revealed that eGFR was the only independent predictor for the occurrence of mid-term cardiac events (composite of re-hospitalization due to HF and all-cause death; aHR = 0.9870, p = 0.02597). The Kaplan–Meier survival curves of the two groups demonstrated no difference in cumulative event-free rates. In the subgroup with preserved renal function at admission (eGFR ⩾ 30 ml/min/1.73 m2), the continuous use of tolvaptan increased composite events (aHR = 2.130, p = 0.02549).
Conclusions:
The continuous use of tolvaptan after discharge did not affect mid-term cardiac events of HF overall but may be associated with increased cardiac events in the subgroup with preserved renal function. These findings suggest that the tolvaptan administration might need to be limited to treatment of in-hospital acute HF.
Introduction
Although advances in medical therapy for chronic heart failure (HF) have improved clinical outcomes, there remain a substantial proportion of patients who repeats hospitalization for HF. 1 Hypervolemia is associated with mortality and hospitalization for HF. 2 However, excessive use of loop diuretics in order to achieve euvolemia leads to increased mortality due to deleterious effects on neurohormonal activation, electrolyte balance, and cardiac and renal function.1,3 From this point of view, tolvaptan, a selective vasopressin V2 receptor antagonist, is an electrolyte-free water diuretic which acts on the distal nephron collecting. 4 Previous studies have demonstrated that tolvaptan alone may not cause neurohormonal activation.5,6 Although these observations indicate that tolvaptan may have beneficial effect on HF patients, a large-scale clinical trial (EVEREST) showed no effect on long-term mortality or heart failure-related morbidity. 1 A series of meta-analyses indicated that there may exist some subgroups to whom tolvaptan is effective. 7 However, clinical factors associated with efficacy of tolvaptan remain unclear. 8 In this study, we aimed to identify clinical factors associated with the mid-term effect of tolvaptan on clinical outcomes of patients who were discharged after acute decompensated HF.
Methods
Patients
This study has been carried out in accordance with the Declaration of Helsinki. The study protocol was approved by the Bioethical Committee on Medical Research, School of Medicine, Kanazawa University. Written informed consent for data collection and its use was obtained from all patients at the time of admission. We retrospectively analyzed consecutive 214 patients with acute decompensated HF who received tolvaptan (initial dose 8.6 ± 3.6 mg/day) during their hospitalization in our institutions from January 2011 to December 2013. The dosage of tolvaptan and treatment period were decided by a physician based on the clinical conditions of each patient. The following patients were excluded from this study; those who needed hemodialysis, cardiopulmonary support system or renal transplantation, those who died before discharge, those who were hospitalized more than 90 days, those who were not followed up after discharge. Thus, 74 patients were excluded and the remaining 140 patients were analyzed (Figure 1).

Flow chart of the study. Consecutive 214 heart failure patients treated with tolvaptan during hospitalization were retrospectively included in this study. 74 patients were excluded and the remaining 140 patients were analyzed.
Clinical evaluations
Standard M-mode and two-dimensional echocardiographic studies were performed to identify and quantify the morphological features of the left ventricle in accordance with the guideline of the American Society of Echocardiography. 9 The 140 patients were divided into two groups according to the condition of the tolvaptan use at discharge; 77 in the tolvaptan-continued group and 63 in the discontinued group. The continuation or discontinuation of tolvaptan after discharge was decided by physicians based on clinical conditions. Cardiac events were defined as composite cardiac events including re-hospitalization due to deteriorated HF and all-cause death (death from any cause). Cardiac events were retrospectively corrected by using the medical record system.
Statistical analysis
Continuous variables are expressed as mean ± SD or median (interquartile range), as appropriate. Categorical variables are presented as absolute numbers and proportions (%). Mann–Whitney U test and Fisher’s exact test were used to compare continuous variables and categorical data between two groups. Wilcoxon signed-rank test and Friedman test with Bonferroni correction were used for paired data. The Cox proportional hazards model was used to estimate the hazard ratio (HR) and 95% confidence interval for cardiac events. Cumulative event rates were examined by the Kaplan–Meier method and log-rank test. A p value <0.05 was considered statistically significant.
Results
Baseline characteristics
The baseline characteristics of the patients at the time of admission and treatment during hospitalization are shown in Table 1. The mean age of the 140 patients was 77.1 ± 11.0 years, of which 88 (62.9%) were males. All patients except two had New York Heart Association (NYHA) ⩾ III classes. Left ventricular ejection fraction (LVEF) and estimated glomerular filtration rate (eGFR) were 51.6 ± 17.0% and 39.0 ± 21.9 ml/min/1.73 m2, respectively. Loop diuretics were used for all patients except one. The time to initiation of tolvaptan treatment after hospital admission was 5 (2–12) days. In comparison with the discontinued group, the tolvaptan-continued group showed a younger age and lower eGFR.
Baseline characteristics at the time of admission and treatment during hospitalization.

Data given as mean ± SD, median (interquartile range) or n (%).
ACE, angiotensin-converting enzyme; ALT, alanine aminotransferase; ARB, angiotensin II receptor blocker; AST, aspartate aminotransferase; BNP, brain natriuretic peptide; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; PDE, phosphodiesterase.
Changes in renal function from admission to outpatient follow up
We first assessed the changes in body weight, electrolyte and renal function in the two groups (Figure 2). Body weight decreased significantly during hospitalization in both groups (from 60.1 ± 12.3 kg to 56.1 ± 12.5 kg in the tolvaptan-continued group, p = 1.84 × 10−11; from 55.5 ± 11.7 kg to 51.9 ± 10.7 kg in the discontinued group, p = 3.14 × 10−8). Between two groups, body weight was similar at discharge (56.0 ± 12.4 versus 52.2 ± 10.9, p = 0.0996). After discharge, the serum sodium level significantly increased in the tolvaptan-continued group (138.1 ± 4.7 mEq at the time of tolvaptan administration, 140.0 ± 5.1 mEq at the first outpatient follow up, p = 0.0067), although the difference in serum sodium levels was not observed between two groups at the first outpatient follow up. The serum creatinine level consistently increased in the discontinued group, but this trend was not observed in the tolvaptan-continued group.
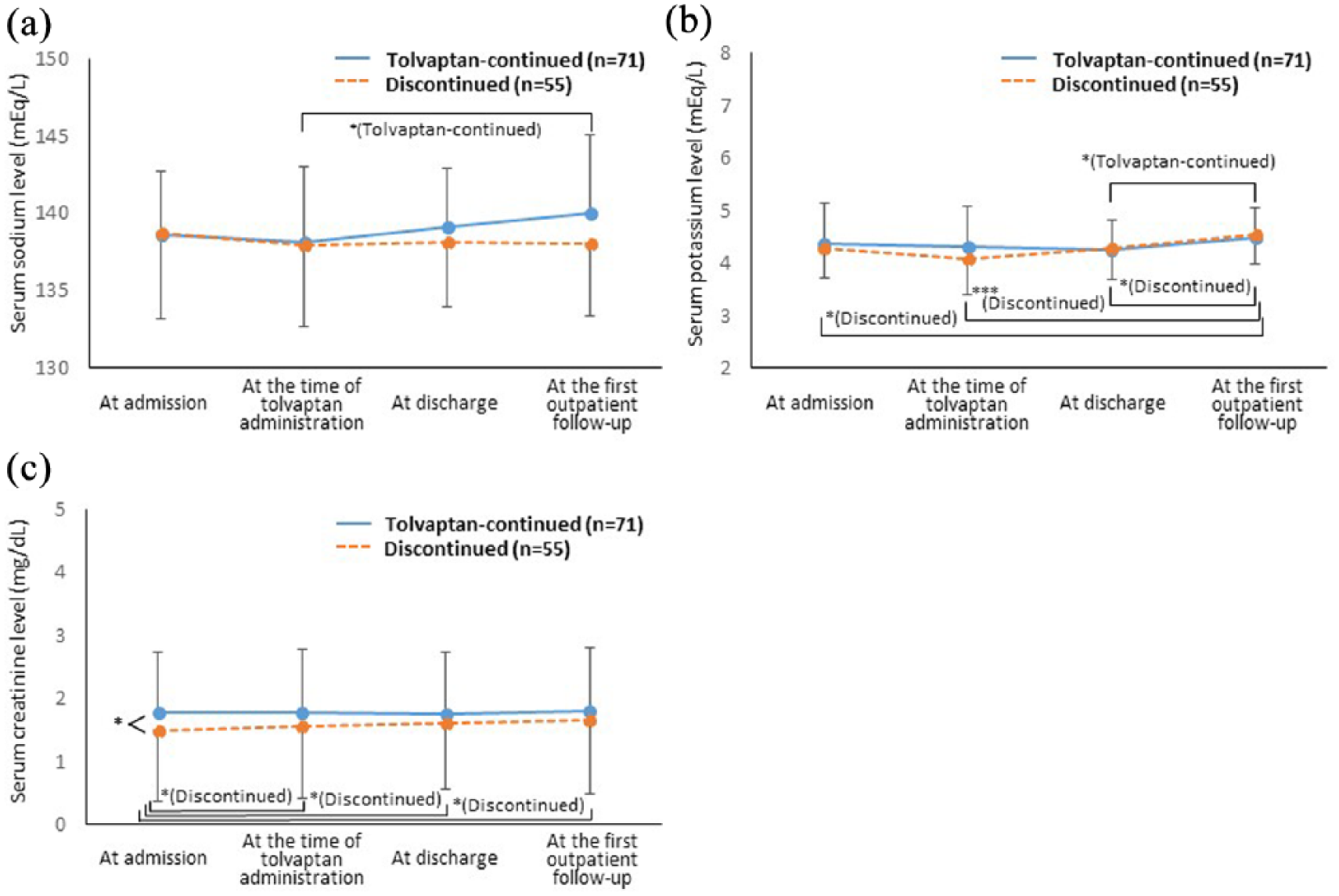
Changes in (a) serum sodium, (b) potassium and (c) creatinine levels. In the tolvaptan-continued group, the serum creatinine level did not change whereas the serum sodium level increased significantly after discharge.
Continuation or discontinuation of tolvaptan and mid-term outcomes
We then examined whether the continuous use of tolvaptan after discharge had effect on clinical outcomes in the 140 patients. During the follow-up period of 139 (58.5–365) days, 88 composite events (4 deaths and 84 re-hospitalization due to deteriorated HF) occurred. The Cox proportional hazards model revealed that eGFR was the only independent predictor for the occurrence of composite events, whereas the continuous use of tolvaptan did not predict composite events (Figure 3). Indeed, the Kaplan–Meier survival curves of the two groups demonstrated no difference in cumulative event-free rates (p = 0.0549; Figure 4). Finally, we calculated the adjusted HR for composite events in various subgroups to assess whether the continuous use of tolvaptan has beneficial or adverse effect in specific subgroups. No significant interactions were observed between the continuous use of tolvaptan and composite events in subgroups of age (cutoff = 80 years), sex and LVEF (cutoff = 40%), whereas the continuous use of tolvaptan was associated with increased composite events in the subgroup with preserved renal function at admission (eGFR ⩾ 30 ml/min/1.73 m2; Figure 5).

aHRs of composite events calculated by the Cox proportional hazards model. eGFR was the only independent predictor for the occurrence of composite events.
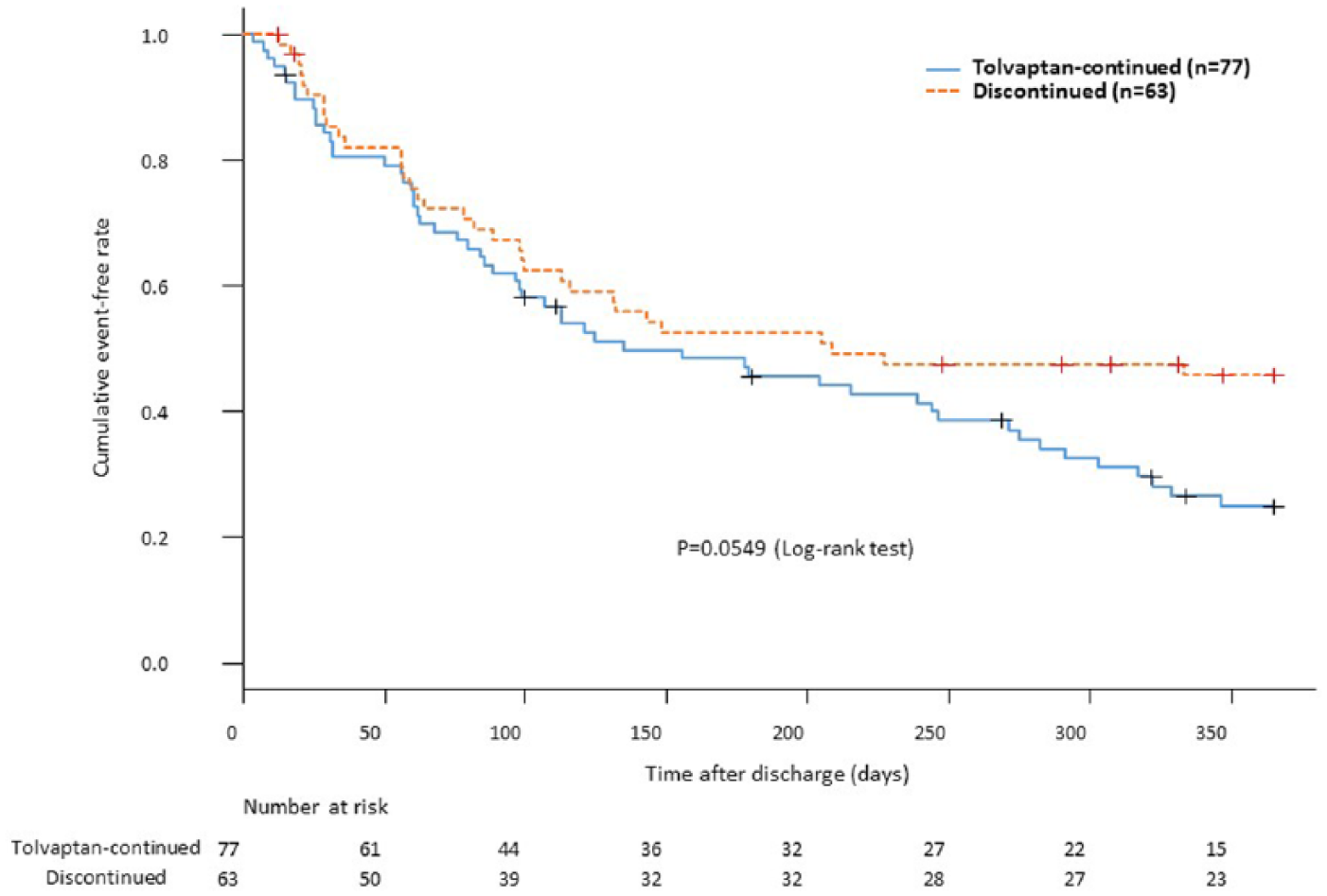
The Kaplan–Meier survival curves of cumulative event-free rates in the tolvaptan-continued and discontinued groups. There was no significant difference between them.

Subgroup analyses for the composite events associated with continuous use of tolvaptan, which were adjusted for all clinical variables. The continuous use of tolvaptan was associated with increased composite events in the subgroup with preserved renal function.
Discussion
In this study, we demonstrated that the continuous use of tolvaptan was not associated with worsening renal function after the discharge of patients who had been hospitalized with acute decompensated HF. The continuous use of tolvaptan did not have any effects on the occurrence of composite events in the overall HF patients but may be associated with increased composite events in the subgroup with preserved renal function.
Tolvaptan did not cause worsening renal function
Excessive use of loop diuretics has been associated with worsening renal function and a poor prognosis in patients with HF, which can in part be explained by intravascular dehydration.10,11 Meanwhile, tolvaptan selectively binds to the vasopressin V2 receptor and inhibits reabsorption of free water, 12 resulting in osmotic movement of fluid from the extravascular to intravascular space. Thus, administration of tolvaptan alone may not result in intravascular dehydration, a major factor in renin–angiotensin–aldosterone system activation and worsening renal function. 5 Although we did not measure serum aldosterone levels and plasma renin activity in this study, unchanged serum creatinine levels during the study period in the tolvaptan-continued group (Figure 2) is consistent with these previous observations.
Tolvaptan may be associated with increased mid-term cardiac events in HF with preserved renal function
Our data demonstrated that the continuous use of tolvaptan did not have beneficial or adverse effects on the occurrence of composite events in the overall 140 HF patients [Figures 3 and 4]. A previous large-scale clinical trial (EVEREST) reported similar results; tolvaptan initiated for the acute treatment of patients hospitalized with HF had no effect on long-term mortality or heart failure-related morbidity. 1 However, there may exist some subgroups of patients who may receive beneficial effect of tolvaptan. The post hoc analysis of ACTIV in CHF trial demonstrated that the 60-day mortality was lower in patients whose serum sodium had improved, 13 although this association was not observed in a subgroup analysis of the EVEREST trial. 1 In terms of renal function, previous studies showed that preserved eGFR was associated with favorable response to tolvaptan, defined by increased urine volume, in acute decompensated HF. 14 However, it remains unclear whether HF patients with preserved eGFR receive beneficial effects of tolvaptan on mid-term clinical outcomes. Unexpectedly, the continuous use of tolvaptan after discharge was associated with increased mid-term cardiac events in the subgroup with preserved renal function (eGFR ⩾30 ml/min/1.73 m2; Figure 5). Thus, tolvaptan may have a dual aspect in the treatment of HF according to the treatment phase; tolvaptan may be useful for in-hospital management of acute decompensated HF without resulting in electrolyte imbalance and worsening renal function (Figure 2), while it may also be associated with increased mid-term cardiac events in the subgroup with preserved renal function (Figure 5). Factors contributing to this mid-term finding are unclear. However, attenuation of tolvaptan effects after discharge may be a possible explanation. 15 Although we were unable to investigate the dose of loop diuretics in the outpatient clinic, it can be assumed that the tolvaptan-continued group with preserved renal function might not have been treated with a sufficient dose of loop diuretics after attenuation of tolvaptan effects. In addition, water intake after discharge might have been increased due to thirst, a major side effect of tolvaptan, which could be another factor associated with this mid-term finding.
Meanwhile, this adverse association was not observed in the subgroup with impaired renal function (eGFR <30 ml/min/1.73 m2), which is consistent with a recent study demonstrating the safety and efficacy of tolvaptan for long-term management of HF with chronic kidney disease. 16
Together, we suggest that clinicians should pay attention to signs of worsening HF in patients with preserved renal function who need to continue tolvaptan after discharge. Given the beneficial effects on fluid management without electrolyte imbalance or worsening renal function (Figure 2), administration of tolvaptan might need to be limited to in-hospital management of acute decompensated HF, in patients with preserved renal function. Further large-scale, prospective studies are warranted to verify subgroups of HF patients who may receive benefits or disadvantages from the continuous use of tolvaptan.
Study limitations
This study has several limitations. First, this was a retrospective study. Thereby, the reasons for continuation or discontinuation of tolvaptan varied according to the condition of the patients. In addition, data at discharge [e.g. hemodynamic parameters, serum brain natriuretic peptide (BNP) levels and the dosage of loop diuretics] were missing in a significant number of patients due to the retrospective nature of the study design. As a result, the severity of HF at discharge might be different between the two groups. Second, the number of patients was relatively small. Further, about one-third of the patients were excluded according to the criteria. Third, the study population was enrolled in tertiary referral centers, thus creating a selection bias regarding the stage of the disease. Fourth, presence or absence of the past history of HF, which can be associated with the re-hospitalization rate, was missing.
Conclusion
The continuous use of tolvaptan after discharge did not affect mid-term cardiac events of HF overall but may be associated with increased cardiac events in the subgroup with preserved renal function. Since efficacy and safety of tolvaptan for fluid management during hospitalization was observed in this study, the tolvaptan administration might need to be limited to treatment of in-hospital acute decompensated HF.
Footnotes
Acknowledgements
We thank Dr Tetsuo Konno for his comments on our manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Kensuke Fujioka, Sumio Mizuno, and Masakazu Yamagishi received lecture fee from Otsuka Pharmaceutical Co., Ltd.