
Abstract
Background:
The aim of the present study was to determine whether raised preoperative serum creatinine affected the long-term outcome in patients undergoing surgical aortic repair for Stanford A acute aortic dissection (AAD).
Methods:
A total of 240 patients diagnosed with Stanford A AAD underwent surgical repair from January 2006 to April 2015. A propensity score matching was applied, resulting in 73 pairs consisting of one group with normal and one group with preoperative elevated creatinine levels. The cohorts were well balanced for baseline and preoperative clinical characteristics. Both groups were compared regarding their early postoperative variables, as well as estimated survival with up to 9-year follow up. Also, the impact of acute postoperative kidney injury and its severity on long-term survival was analyzed.
Results:
The proportion of patients suffering Stanford A AAD with raised creatinine levels was 31.3% (n = 75). After propensity matching, there were no statistically significant differences regarding demographics, comorbidities, preoperative baseline and clinical characteristics. Postoperatively matched patients with elevated creatinine had longer intensive care unit (p < 0.001) and total hospital stay (p = 0.002), prolonged intubation times (p = 0.014), higher need for hemofiltration (p < 0.001), higher incidence of temporary neurological disorders (p = 0.16), infection (p = 0.005), and trend toward higher incidence of sepsis (p = 0.097). However, there were no significant differences regarding 30-day mortality (20.5% versus 20.5%, p = 1.000) and long-term overall survival. Further, neither the incidence nor the different stages of acute kidney injury according to the Acute Kidney Injury Network showed any statistically significant differences in terms of long-term survival for both groups [log rank p = 0.636, Breslow (generalized Wilcoxon) p = 0.470, Tarone–Ware p = 0.558].
Conclusions:
Patients with elevated creatinine levels undergoing surgical repair for Stanford A AAD demonstrate higher rate of early postoperative complications. However, 30-day mortality and long-term survival in this patient cohort is not significantly impaired.
Introduction
Acute kidney injury (AKI) is one of the major adverse events after aortic surgical procedures and is associated with prolonged hospital stay, adverse prognosis, increased costs and even death.1,2 The incidence of AKI in patients after repair of acute Stanford A acute aortic dissection (AAD) is significantly higher compared with other cardiac surgical procedures and is described with an incidence ranging from 18% to 67%, whereas 11–14% of these patients require dialysis due to renal failure after surgery.3–6 The mortality among patients with dialysis-dependent renal failure as an independent risk factor may account for 37.8%. 7 Postoperative AKI after surgical repair of AAD might be caused multifactorially by predisposing factors such as preoperative administration of radiocontrast medium, pre-existing vascular disease, cardiopulmonary bypass followed by systemic inflammatory response, blood transfusion, or ischemia–reperfusion injury.8–10 Also, preoperatively elevated serum creatinine level is revealed as an independent predictor for postoperative renal failure requiring dialysis and resulting in higher morbidity and mortality.11,12
However, the reported incidence of postoperative AKI after repair of AAD varies widely and the influence of preoperatively elevated serum creatinine levels in this demanding patient cohort is still presenting a lack of data in terms of long-term results. Furthermore, previous comparative studies have been limited by several confounders due to their retrospective design biasing postoperative outcome. The aim of this study was to determine whether raised preoperative serum creatinine affects early and long-term outcomes in patients undergoing surgical aortic repair for acute aortic type A dissection. Further, the impact of AKI, standardized according to the criteria of the Acute Kidney Injury Network (AKIN), 13 on long-term outcome was assessed.
Patients and methods
As already described elsewhere, 14 the study design was a retrospective review of the prospectively collected data. The institutional board of Cologne University approved this study and waived the need for individual patient consent. Another analysis based on the patient cohort from the present report was published by our group elsewhere. 14 All data sets are represented by routine parameters from our institution that did not constitute any additional burden for the patients. This manuscript presents a separate study with a different protocol and approval process than the abovementioned study. An analysis of all consecutive patients who underwent aortic repair for an AAD Stanford A between January 2006 and April 2015 was performed, with a particular focus on the preoperatively measured serum creatinine level. A total of 250 patients diagnosed with AAD Stanford A were admitted to our hospital during the study period. Ten of them died prior to surgery, whereas 240 patients underwent aortic repair. All patients included had their creatinine serum levels measured before undergoing surgical aortic repair. The upper limit of the normal reference range for creatinine in our unit was 1.1 mg/dl. Patients were divided into two groups depending on their preoperative serum creatinine. The proportion of 31.3% (n = 75) was hospitalized with elevated serum creatinine prior to the surgical procedure. A propensity score matching was applied resulting in 73 pairs consisting of one group with normal and one with preoperative creatinine levels ⩾ 1.1 mg/dl. The cohorts were well balanced for baseline and preoperative clinical characteristics. The surgical procedure for our patients suffering an AAD is already described by our group and published elsewhere. 14
The primary endpoint was long-term overall cumulative survival with up to 9-year follow up. Secondary endpoints were early postoperative clinical characteristics and complication rates. Follow up was obtained through direct contact with patients and patients’ relatives, physicians and local hospitals, as well as through data collection from our institutional quality information management system and electronic documentation system. Further, the impact of AKI, according to the criteria of the AKIN, 13 on the long-term outcome was examined. AKIN, stage I was defined as an increase of the serum creatinine level by 0.3 mg/dl or an increase to the 1.5–2.0-fold in 48 h from baseline; stage II was defined as an increase to 2.0–3.0-fold of the preoperative value in 48 h; stage III was defined as an increase more than threefold from baseline, a value more than 4.0 mg/dl, or the need for dialysis.
Statistical analysis
All data were analyzed using IBM SPSS Statistics for Windows, Version 21 (IBM Corp., Armonk, NY, US) and are presented as continuous or categorical variables. Continuous data were evaluated for normality using one sample Kolmogorov–Smirnov test and confirmed by histograms. Continuous variables were expressed as the mean ± standard deviation in cases of normally distributed variables or median (interquartile range) in cases of non-normally distributed variables. Categorical variables are presented as total numbers of patients and percentages. Continuous data were analyzed with unpaired t test for normally distributed variables and Mann–Whitney U test for non-normally distributed variables. Pearson’s χ² or Fisher exact tests were used for categorical data dependent on the minimum expected count in each cross tab. Kaplan–Meier survival estimation was applied for long-term survival analysis. Propensity score matching function of SPSS software was conducted to reduce confounding bias between the groups. A propensity score for each patient was estimated using a logistic regression model with preoperative characteristics that showed statistically significant differences between the two groups as independent variables. Matching was based on one-to-one nearest neighbor matching method with a tolerance level on the maximum propensity score distance (calipers of width 0.2 standard deviations of the logit of the propensity score). This propensity-score-based matching procedure resulted in a total number of 73 pairs that were well matched for baseline characteristics. p values < 0.05 were considered statistically significant.
Results
As already published elsewhere, 14 preoperative demographics and baseline characteristics of the entire patient cohort were initially compared using a univariate analysis in order to define parameters that might influence outcomes. The matching was performed based on patients’ characteristics that were statistically different between the two groups in the analysis of the entire cohort including logistic Euroscore (p = 0.007), proportion of female patients (p = 0.008), incidence of diabetes (p = 0.004), rate of pericardial effusion (p = 0.042), hemodynamic instability (p < 0.001), and proportion of patients in coma (p = 0.036). Unlike the variability of the baseline characteristics of both groups in the entire population, the two propensity-matched groups were well balanced, and no significant differences were observed in patients’ demographics and preoperative baseline characteristics, except for weight (Table 1).
Demographics and preoperative baseline characteristics after propensity matching.
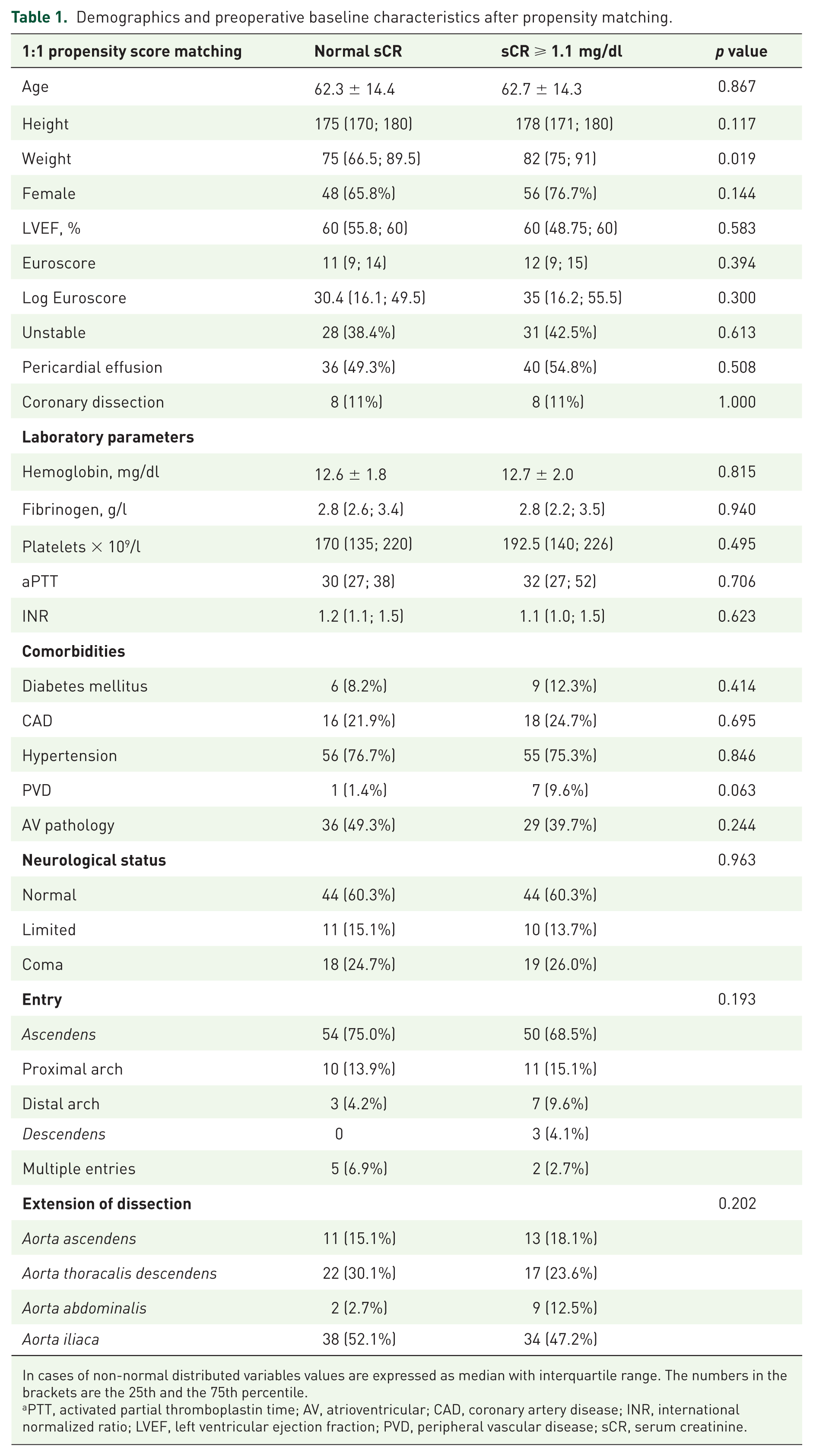
In cases of non-normal distributed variables values are expressed as median with interquartile range. The numbers in the brackets are the 25th and the 75th percentile.
PTT, activated partial thromboplastin time; AV, atrioventricular; CAD, coronary artery disease; INR, international normalized ratio; LVEF, left ventricular ejection fraction; PVD, peripheral vascular disease; sCR, serum creatinine.
Early postoperative outcome
The incidence of postoperative AKI in the cohort of 146 patients was 64.4% (n = 94). AKIN stage I was observed in 51.4% (n = 75) of the patients, stage II occurred in 12.3% (n = 18), whereas stage III was only present in one case (0.7%). After matching, patients with elevated preoperative serum creatinine levels presented a significantly higher incidence of temporary neurological dysfunction (28.6% versus 48.5%; p = 0.016), whereas there were no significant differences in terms of in-hospital stroke rate (p = 0.628). Other early postoperative variables and complications, such as gastrointestinal bleeding (7% versus 21.9%; p = 0.011), mechanical ventilation time (p = 0.021), the need for continuous venovenous hemofiltration (CVVH) (11.3% versus 38.9%; p < 0.001), and postoperative infections (39.4% versus 63.0%; p = 0.005) were observed with a significantly higher rate in the cohort with preoperative creatinine levels ⩾ 1.1 mg/d (Table 2). There were no statistically significant differences between the two groups (p = 0.677) in terms of proportions of patients who were discharged home (18.3% in the normal creatinine cohort versus 11.6% in the cohort with creatinine ⩾ 1.1 mg/dl), to a rehabilitation center (35.2% versus 37.7%), to an external intensive care unit (ICU) (25.4% versus 29%) or who died in hospital (21.1% in the normal creatinine cohort versus 20.3% in the cohort with creatinine ⩾ 1.1 mg/dl). A separate analysis regarding ICU death (p = 0.792) and intra-operative death (p = 1.000) showed no statistically significant difference.
Intraoperative and early postoperative outcomes after propensity matching.

In cases of non-normal distributed variables values are expressed as median with interquartile range. The numbers in the brackets are the 25th and the 75th percentile.
FFP, fresh frozen plasma; ICU, intensive care unit; RBC, red blood cells; sCR, serum creatinine.
Analysis of cause of death
Analyzing causes of death in both groups, there was a significantly higher incidence of multiorgan failure in the group with elevated preoperative serum creatinine levels (1.4% versus 11.1%; p = 0.017) and a trend toward a higher rate of sepsis (2.7% versus 9.7%; p = 0.097). While other causes of death, such as cardiac death (5.5% versus 9.7%, p = 0.335), bleeding (6.8% versus 1.4%, p = 0.209), ischemic or hemorrhagic stroke (6.8% versus 1.4%, p = 0.209) and other conditions (5.5% versus 5.5%, p = 1.000) were similarly distributed between the two groups.
Long-term outcomes
Long-term outcome with up to 9-year follow up was analyzed and compared between the groups using Kaplan–Meier estimation. Patients with elevated serum creatinine (sCR) levels ⩾ 1.1 mg/dl preoperatively and patients with nonelevated preoperative sCR levels appeared to be comparable after propensity score matching (Figure 1). In terms of survival estimation after propensity score matching, comparing groups with similar risk profiles showed no significant differences in long-term overall cumulative survival in both groups. Kaplan–Meier estimations resulted in no statistically significant differences between the two groups in both generalized Wilcoxon (p = 0.531) test which is more sensitive for early postoperative period and log rank (p = 0.483) test which is more sensitive for later follow up. Further, neither the incidence nor the different stages of acute kidney injury according to AKIN showed any statistically significant differences in terms of long-term survival for both groups [log rank p = 0.636, Breslow (generalized Wilcoxon) p = 0.470, Tarone–Ware p = 0.558; Figure 2].

Overall cumulative survival for propensity-matched patients with normal and preoperative elevated serum creatinine with acute Stanford A dissection after surgical aortic repair.

Overall cumulative survival for patients with acute Stanford A dissection after surgical aortic repair according to Acute Kidney Injury Network stages.
Discussion
The aim of our study was to evaluate the impact of preoperative elevated sCR levels on short- and long-term outcome of patients undergoing aortic repair after diagnosis of AAD. AAD is known as a life-threatening disease with a reported mortality up to 30%.15–17 Preoperative elevated sCR levels are described as predictive of renal failure, with increased early mortality and affected long-term outcome.7,11,12,18 Our patient cohort with elevated creatinine levels undergoing surgical repair for Stanford A AAD demonstrated significantly higher early postoperative complication rates, longer ICU and total hospital stay, prolonged intubation times, higher need for hemofiltration, higher incidence of temporary neurological disorders, more infections, and a trend toward higher incidence of sepsis. However, these early results did not impact long-term survival in this patient cohort.
The upper limit of the normal reference range for creatinine in our unit was 1.1 mg/dl. Sato and colleagues demonstrated that the best cut-off value of preoperative creatinine concentration associated with postoperative renal replacement therapy for patients undergoing cardiac surgery was 1.12 mg/dl, with a sensitivity of 60.2% and a specificity of 85.0%. 12 Most of the studies7,11,12,18 represent patients with chronically elevated creatinine levels undergoing elective cardiac surgery. Further, there are studies investigating the impact of chronic kidney disease on long-term survival, especially on patients suffering from an AAD showing a significant proportion of adverse events.19,20 However, several studies are comparable with our findings, showing that preoperative elevated sCR or poorer glomerular filtration rate in patients undergoing surgical repair may not have a significant effect on long-term survival.4,21 However, patients with an AAD represent a demanding collective and might not easily be comparable with patients of abovementioned studies for various reasons. First, AAD is a major emergency, comprising patients with potentially unstable cardiovascular conditions with an unknown baseline kidney function. Patients with normal renal function may develop AKI on admission and present elevated baseline sCR levels. On the other hand, the total incidence of AKI due to AAD might be extremely underestimated in these patients; AKI itself, depending on the definition used, is described as having an incidence of 5–30% after cardiac surgery and is associated with an increased mortality.22,23 Again, patients with an AAD represent a special cohort showing a significantly higher incidence of AKI ranging from 18% to 67% and requiring renal replacement therapy in 11–14% of those patients.1,4–6 The incidence of postoperative AKI in the cohort of 146 patients was comparable with 64.4%, however the amount of patients suffering from AKIN stage II and III was lower compared with other studies. 5 Overall need for CVVH at our institution for patients undergoing aortic repair after AAD was 25.2%. The incidence is considerably high; however, the incidence is similar to the results by Wu and colleagues. 8 Not surprisingly, renal replacement therapy was performed with a significantly higher rate in the patient cohort with preoperative elevated sCR levels (11.3% versus 38.9%; p < 0.001). Even though dialysis is known as a negative predictor, with an increased postoperative mortality rate over 30%, 7 patients with elevated preoperative sCR levels and a significant higher need for postoperative CVVH did not affect long-term outcome.
There are two possible explanations for preoperative elevated sCR levels and the incidence of postoperative AKIN, whereas both can be affected either by intrinsic or prerenal kidney injury. 24 Prerenal AKI might be caused by decreased renal perfusion due to hypotension, cardiovascular instability and hemorrhagic shock. It is essential to attenuate the progressing tubular necrosis as one of the main pathomechanisms of AKI to avoid a damage that might lead to a chronic kidney injury.8,25 Studies have demonstrated that an instant onset of renal replacement therapy possibly improves the outcome.8,26,27
The reason why the long-term outcome of our cohort was not significantly affected might be the fact that our patients on the ICU are daily visited by a nephrologist, and CVVH is accessible promptly without any delay. Whereas the incidence of CVVH in the group with elevated preoperative sCR levels was higher compared with other studies, it did not affect long-term survival, possibly due to the early commencement of CVVH and attenuation of transient tubular necrosis leading to restoration of renal function.
Limitations of the study
This study is an analysis of prospectively collected registry data from a single medical center. All consecutive patients undergoing aortic repair after AAD were included in our analysis, resulting in a large cohort for a disease with low incidence. The propensity score matching allowed for a fair comparison of patients with very similar risk profiles, thus significantly reducing possible confounders. However, the total number of 240 patients and 73 pairs after matching represents a relatively small patient cohort, potentially limiting statistical power. As AAD represents a life-threatening emergency, in many cases, little can be said about the reason of their elevated preoperative sCR levels. The differentiation between chronic renal disease and an AKI cannot be absolutely confirmed. Overall cumulative survival over long-term follow up might only be a surrogate for the absence of chronic renal failure, which is known to be associated with decreased long-term survival. Further, the impact of renal malperfusion due to the dissected descending aorta is a possible explanation for the incidence of renal failure and was not investigated in this study.
Reconcluding, the findings of this study demonstrated higher rate of early postoperative complications in patients with Stanford A AAD, such as neurological disorder, gastrointestinal complications and the need of hemofiltration, thus the analysis helps to determine the strategies of patient management in the early postoperative period. However, long-term survival in this patient cohort is not significantly impaired, and that allows us to make an inference about the priority of the initial period regarding overall patients’ viability. Despite overall comparability with many other studies, there is still remaining discrepancy to a certain extent requiring the need for more investigations in order to assess the underlying factors of renal dysfunction affecting the long-term outcome after surgery for Stanford A AAD.