
Abstract
Background:
Pericardial effusion (PE) can develop in several pathological scenarios, and is often initially evaluated by means of echocardiography. Computed tomography (CT) has been used as an aid in the management of patients presenting with PE, in selected cases. The role of CT-guided pericardiocentesis in contemporary practice, however, remains not fully ascertained. We aimed at presenting a systematic review concerning the state-of-the-art of this technique.
Methods:
A systematic review of published data on the use of CT for guiding pericardiocentesis was carried out (search performed on PubMed, ISI Web of Knowledge and Scopus databases).
Results:
From title and abstract analysis, 14 articles were included that met the prespecified criteria. After full-text analysis, six articles were excluded. The eight articles under analysis included a total of 635 procedures performed in 571 patients. CT guidance was mostly used in a postoperative setting (364 procedures). Most procedures were done mainly for therapeutic purposes (528 procedures). Success rates ranged from 94% to 100%. Complications ranged from 0% to 7.8%.
Conclusion:
CT-guided pericardiocentesis is a useful technique in the approach to PE, in several clinical scenarios. Its use can be especially relevant in the postoperative period, as well as in individuals with suboptimal image quality (as assessed by echocardiography, for the moment the first choice in the approach to most cases of PE).
Introduction
The pericardium, surrounding the heart and root of the great vessels, can be affected by a plethora of diseases. 1 Physiologically, the pericardial sac contains a small amount of fluid which acts as a lubricant and minimizes friction between its parietal and visceral layers.1,2 Pericardial effusion (PE), the accumulation of excess fluid in the pericardial space, can develop in several pathological scenarios and have different clinical consequences.1,2 Presentation depends on variables such as aetiology and speed of accumulation and can range from an asymptomatic patient to chest discomfort, dyspnoea, orthopnoea and cardiac tamponade.1,3,4 As such, the management of a PE should be individualized and directed at the underlying cause.1,3 Though not always necessary in its approach, pericardiocentesis can be of relevance for diagnostic as well as therapeutic purposes.1,4 According to the current European Society of Cardiology guidelines, pericardiocentesis (or surgery, if necessary according to clinical context) is indicated in the presence of cardiac tamponade, or for symptomatic moderate to large pericardial effusions which do not respond to medical therapy, as well as in case of suspicion of unknown bacterial or neoplastic aetiology. 1
Echocardiography plays a pivotal role in the contemporary assessment of these patients, allowing the diagnosis of a PE as well as assessing its impact on cardiac function.1,2,4 It is the imaging modality of choice for the guidance of pericardiocentesis, being portable, quick to perform and allowing continuous real-time imaging.2,5,6 In comparison with a blind technique, the use of echocardiography to guide a pericardiocentesis represents an important step in optimizing this invasive procedure. 5 This has been highlighted in contemporary guidelines.1,2 Although a major advancement in the approach to a PE, several factors such as patient body type, pulmonary disease, recent cardiac surgery (where many times effusions can be loculated and accumulate rapidly) and pain or inappropriate acoustic windows due to a surgical wound can negatively affect its performance.2,7,8 Given these possible shortcomings in terms of image acquisition as well as the necessity for a precise needle orientation (especially in nontypical approaches), computed tomography (CT)-guided pericardiocentesis has gained interest.6,9,10 This technique, some of the first descriptions of which concerning PE diagnosis and possible pericardiocentesis guidance were made over 30 years ago,11,12 has been thoroughly detailed elsewhere.6,7,13 It potentially allows overcoming many of the hindrances concerning echocardiography, and can also be relevant for the exclusion of other thoracic pathologies.6,14,15 As such, its use could be of relevance in several clinical situations.6,14,15 However, despite previously published series and technical descriptions, the role of this technique in the contemporary approach to a PE remains to be fully specified.2,6,9,16
Given these considerations, we aimed at presenting a systematic review concerning the use of CT-guided pericardiocentesis, as well as comment on the future perspectives of this technique.
Methods
Search strategy
The systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance, as detailed in the PRISMA checklist (available at www.prisma-statement.org).
The study started with a search on three databases: Medline (PubMed), ISI Web of Knowledge and Scopus, using the queries “computed tomography AND pericardiocentesis”; “computed tomography AND pericardiostomy”; “CT AND pericardiocentesis”; “CT AND pericardiostomy”.
The search took place between July and August 2017, and no articles were excluded based on publication date. The aim of our search was to identify studies assessing the use of CT-guided pericardiocentesis. The queries resulted in a total of 439 articles on the PubMed database (full search details available in Supplementary File 1), 149 on ISI Web of Knowledge and 639 on Scopus. No additional studies were found after searching the references of previous review articles.
Inclusion criteria
Both prospective and retrospective human studies were included.
Exclusion criteria
Case reports, congress abstracts (without subsequent full paper publication) and studies containing fewer than 10 patients were excluded, as were studies written in languages other than English.
Studies using CT mainly in order to evaluate PE characteristics but not using this imaging method in order to guide a pericardial procedure (i.e. pericardiocentesis/pericardiostomy) were also considered outside the scope of the present report.
Quality assessment of studies and data extraction
Study quality and eligibility were individually assessed by three investigators.
The investigators individually assessed if studies addressed the use of CT-guided pericardiocentesis, and if all inclusion/exclusion criteria prespecified for the review (as described above) were met. This was done initially through title and abstract analysis, and then (if abstracts complied to specifications) through full-text assessment. In addition, the investigators specifically sought whether the articles described the number of individuals under study, as well as the success rate of the procedure. Data extraction (see Tables 1 and 2) was individually done from the data published in the articles, and then compared by the investigators. Different opinions regarding the relevance of articles were solved by consensus between the authors.
Overview of studies assessing CT-guided pericardiocentesis (and/or pericardial drain placement).

= different definitions (see text for details);
= data presented jointly for CT and echo-guided pericardiocentes (see text for details).
AR, aortic replacement; ASD, atrial septal defect; CABG, coronary artery bypass graft; HT, heart transplant; NA, not available; VS, valve surgery; VSD, ventricular septal defect.
Overview of complications described in studies assessing CT-guided pericardiocentesis (and/or pericardial drain placement).
Percentage in some studies calculated from values described.
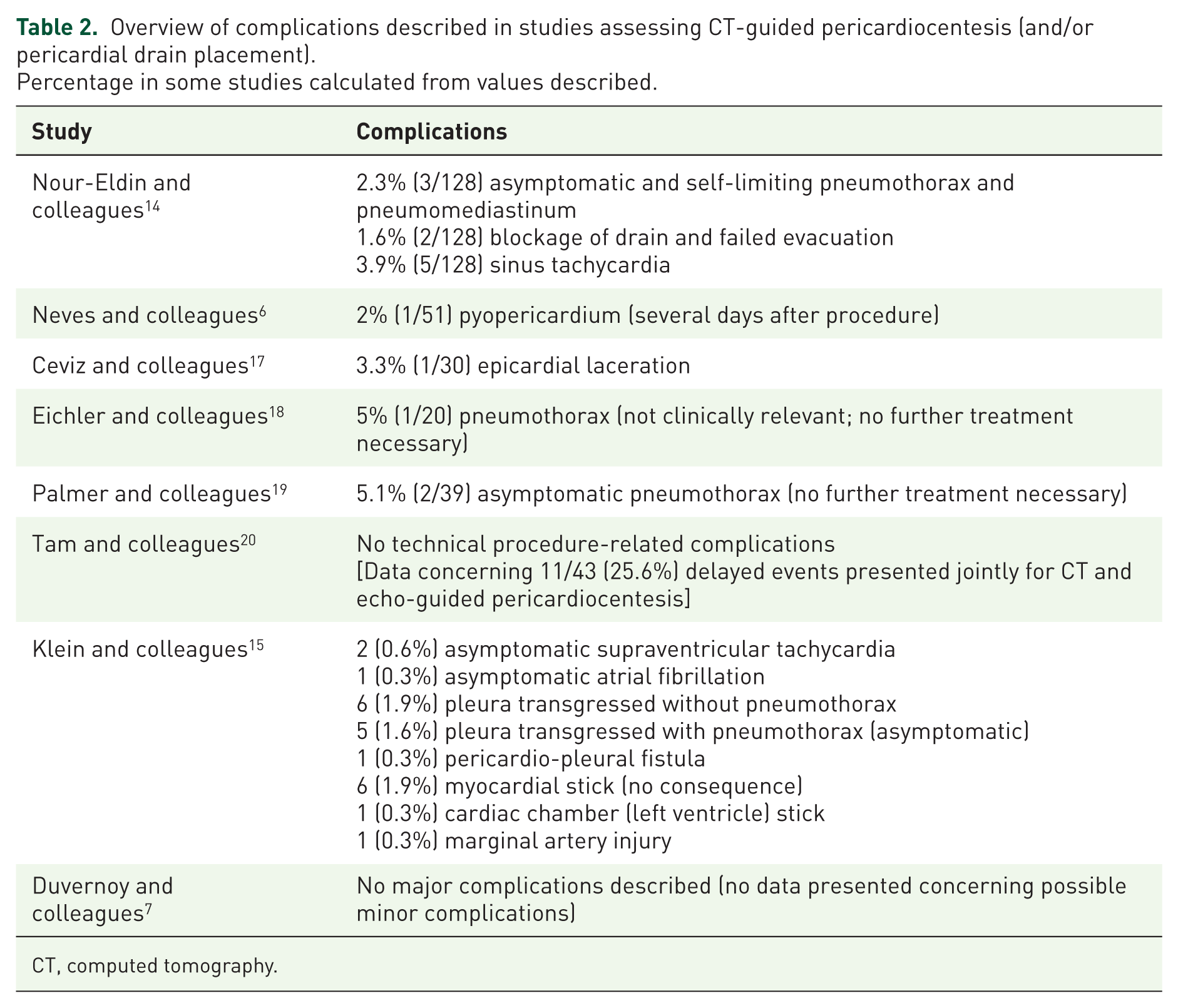
CT, computed tomography.
Global article quality assessment was carried out according to the method used by Haffar and colleagues. 21
Results
From title and abstract analysis, 14 articles were included that met the prespecified criteria, and this set of articles was analysed by the authors. After full-text analysis, six studies were excluded from this review. Of these, three studies used CT to characterize PE in patients who were subjected to echocardiography-guided22,23 or fluoroscopy-guided pericardiocentesis, 24 one used CT to assess the site of pericardial puncture in an ablation procedure, 25 one used the technique to quantify PE in patients prior to percutaneous pericardiocentesis (not specifying that CT was the method of choice for guiding the procedure) 26 and another concerned mainly the non-invasive evaluation of PE (not presenting data concerning the pericardiocentesis procedure). 18 No further articles were excluded, and all described the number of individuals assessed, as well as the success rate. Data from the included studies were extracted from the published articles (see detailed information below). A flowchart showing the literature search method, as well as the resulting number of articles selected, is displayed in Figure 1.
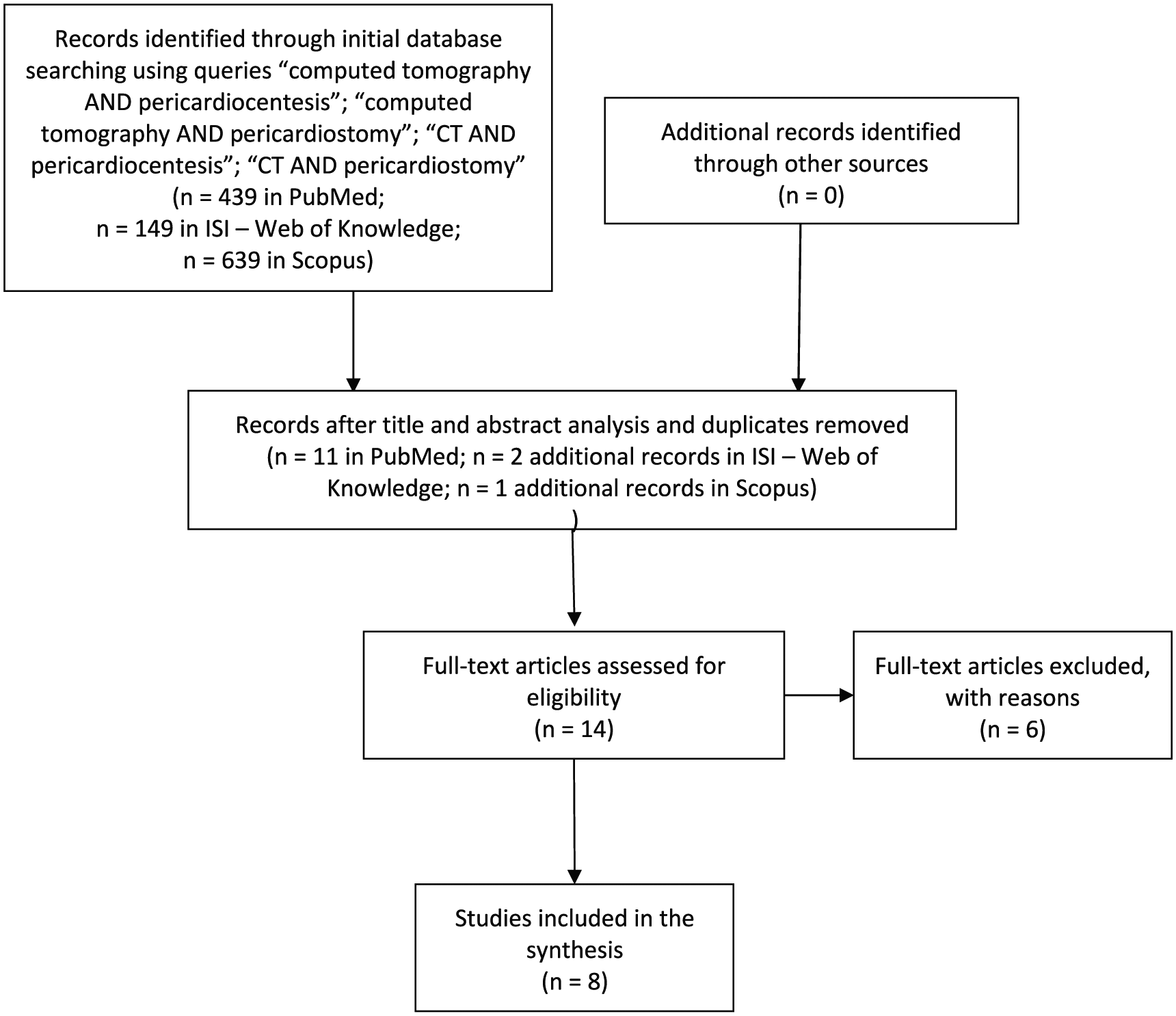
Flowchart showing the literature search method.
The total of eight articles that were included in this review were published between 1996 and 2017 and included a total of 635 procedures performed in 571 patients.6,7,14,15,17,19,20,27
An overview of the studies included is depicted in Table 1 (note that data concerning the study by Tam and colleagues 19 are mostly not specified given that for many variables this study presents a joint description for CT and echocardiography-guided procedures).
Concerning the clinical context, data were available for 595 procedures (partially available for Klein and colleagues). 15 CT guidance was mostly used in a postoperative setting, which comprised 61.2% of the total (364 procedures).
In terms of main indication, data were also available for 557 procedures. Most were done mainly for therapeutic purposes, representing 94.8% of the total (528 procedures).
Success rates ranged from 94 to 100%,6,7,14,17,19,27 although definitions varied according to different studies (see Discussion).
Complications ranged from 0%7,19 to 7.8%. 14 Reporting, however, varied in different studies (as further debated in the Discussion).
An overview of complications described in the studies included is depicted in Table 2.
Concerning the risk of bias of each study, two important sources of bias pertained to the selection of individuals (some after being considered inadequate for echo-guided procedures, whereas in other studies such a condition was not present), as well as to different definitions regarding success (technical versus clinical), as detailed in Table 1 and in the Discussion.
The results of global article quality assessment carried out according to the method used by Haffar and colleagues 21 are presented in Supplementary File 2.
Discussion
The present systematic review assessed the current data concerning CT-guided pericardiocentesis (associated or not with pericardial drain placement). A total of eight studies were included in the final analysis, comprising a total of 635 procedures performed in 571 patients.6,7,14,15,17,19,20,27 It has been previously described that there is great heterogeneity among patients with a PE, given their clinical setting.1,28 Over the last decades, there has been substantial improvement in the application of pericardiocentesis.4,5 Much of this improvement is derived from the use of echocardiography to guide this intervention, and contemporary data attest to its utility in achieving a high degree of success with a low level of complications.5,29,30 The two large series on echocardiography-guided pericardiocentesis, one assessing a total of 1127 and the other 161 procedures, reported a complication rate of 4.7% (1.2% major and 3.5% minor) and 5.5% (1.2% major and 4.3% minor).5,30 This overall favourable profile has been highlighted in the current guidelines. 1 This procedure, however, can be more complex in several types of patients, namely those recently submitted to cardiac surgery, as well as those with suboptimal acoustic windows.6,14,19 In addition, PE characteristics can also pose difficulties in their approach, namely if they are loculated or small (and it should be acknowledged that even small PE, if developed rapidly, can have an important negative impact on clinical status). Some subgroups, such as postsurgery and oncologic patients, appear to be particularly susceptible to adverse consequences associated with the presence of PE.15,19,28 Importantly, these same patients often pose difficulties in terms of ultrasound guidance, and as such there has been interest in the use of other modalities to guide this procedure.15,19,27,31 Of these, CT is especially attractive, given the possibility for good visualization of access route and surrounding structures and the ability (if needed) to guide ancillary procedures.9,13,27 This technique can also provide information on the nature of the PE by the attenuation values of the fluid (assessed as Hounsfield units, with simple effusions generally presenting low attenuation values, contrary to proteinaceous or haemorrhagic content).1,2,22 In addition, it allows precise quantification of the amount of pericardial fluid 1 and has excellent capacity to address pericardial calcification.1,2 The current literature describes a high degree of success associated with this technique.6,7,14,15,17,19,20,27 Another smaller series including eight patients submitted to a total of 11 procedures also reported 100% technical success, and 91% success in draining sufficient pericardial fluid. In this study patients presented with a PE (assessed by echocardiography) which was considered not drainable by ultrasound guidance. 10 It should be acknowledged, however, that different definitions (namely technical versus clinical) were used in different studies. For example, in the study by Klein and colleagues, technical success was reported in 98.4% of cases. In terms of clinical success, though data was only available for a subset of 292 patients, 78.8% showed improvement (whereas 79.4% of those with echocardiographic evidence of tamponade showed improvement). 15 Also, in the report by Ceviz and colleagues, technical success was described in all 30 cases under review. 20 The procedure, however, was deemed successful in only 29 of those (considering that in one of the patients, although a catheter was placed in the pericardial space, fluid was unable to be aspirated given the presence of an organized hematoma). 20 However, despite this discrepancy, when globally considering the studies assessing this technique, CT-guided pericardiocentesis can present an adequate treatment in a majority of otherwise complex patients.17,27
Complications reported were in the range of 0% to 7.8%,7,14,19 as shown in Table 2. These were mainly minor complications (with no need for further invasive interventions or associated relevant clinical adverse outcomes), albeit it should be acknowledged that different definitions for complications were used among different studies. There were, however, instances of important complications which required further treatment (namely one arterial puncture and an epicardial laceration with ensuing hemopericardium).15,20 Puncture of cardiac structures (namely the heart per se or the coronary arteries) is an important potential complication of pericardiocentesis.5,19,27 Although there is data, such as reported in the study by Klein and colleagues, 15 of myocardial chamber stick without apparent adverse events, this complication can have serious consequences, as illustrated in one case described in the same report (with need for fluid resuscitation and subsequent pericardiocentesis) and in the large series of echocardiography-guided pericardiocentesis by Tsang and colleagues where five patients needed surgery and one died as a consequence of chamber puncture. 5 When analysing and comparing data (both in terms of success and complications) between CT and other imaging modalities (and especially echocardiography) caution must be exercised. This stems from several important caveats which limit the application of direct comparisons between different types of published series. One is the fact that at least in some studies one of the criteria for inclusion was the inability to use an echocardiographic approach.17,20 In other cases, this technique was used in some of the patients after a previously failed attempt by another imaging modality, 27 whereas in others still this approach was undertaken in subgroups of patients without a description of previous echocardiography.15,27 As acknowledged by different authors, this highlights the technical difficulty associated with some of these interventions.15,17,19 As described above, CT-guided pericardiocentesis can provide a valuable alternative to surgical intervention in different groups of patients, such as those after surgery or with inadequate echocardiographic profiles.17,27 Another important consideration is that some complications such as rhythm disturbances and infection can also be associated with other imaging techniques, and given their nature may be more related to the procedure per se than to the specific imaging modality used.6,19 It should be noted that despite concerns towards the application of this technique, given the fact that it can be more time-consuming than echocardiography, 7 several reports addressed (whether in all of or part of the cohort under study) the use of CT-guided pericardiocentesis in individuals with hemodynamic compromise (including tamponade features).14,15,27 The results obtained (illustrated in Table 1) argue in favour of the notion that, in certain selected cases, CT guidance could be contemplated in the face of individuals with cardiac tamponade and adverse features for other imaging modalities (namely postoperatively or under anticoagulation).
Importantly, CT-guided pericardiocentesis has several limitations. Firstly, this technique uses ionizing radiation, which could limit its use in certain subgroups (and contraindicates its use during pregnancy).1,2 In the contemporary series reported by Neves and colleagues, median total effective radiation was 3.3 mSv. 6 Given the marked progress in terms of radiation exposure reduction in CT scans, future studies should try to address the radiation requirements for conducting these procedures.32,33 Highlighting differences in terms of radiation exposure with regards to different techniques could theoretically also be of relevance, comprising a further argument for the standardization of the procedure. Secondly, though CT-guided pericardiocentesis can be performed without the need for intravenous contrast, in certain cases this can be used to allow better visualization of anatomical structures (namely the pericardium or vascular structures).2,6,15 This strategy can, however, be associated with nephrotoxicity or the occurrence of allergic reactions.1,2 Finally, although, as described above, there is data concerning the applicability of CT-guided pericardiocentesis in symptomatic patients (and some with features of cardiac tamponade),14,15 the limited availability and lower portability of this technique when compared with echocardiography is still one matter which should be kept under consideration.
Especially when ultrasound guidance is considered not feasible, the risk–benefit ratio should be clinically and holistically pondered, taking also into consideration data for surgical techniques. Although it has previously been stressed that despite the possibility of using a safer technique, pericardiocentesis should not be routinely performed in the face of a PE,3,6 the possibility of improving the performance of this invasive procedure seems of great clinical relevance. Given that no large randomized controlled trial of echocardiography versus CT guidance as a first option (with both short and mid-term follow up) was reported in the present literature, and in the face of the considerations presented, it seems consensual that echocardiography remains a first choice in the approach to most cases of a PE. However, the present review presents several clinical scenarios where CT can play a major role. Additionally, given the technical considerations pertaining to CT and its possible advantages, its use could be integrated in different settings with that of echocardiography, thus allowing for a global multimodality assessment of a PE. As data concerning this technique continues to unravel its full potential, the need for high-quality selection of adequate cases for CT guidance will become a critical necessity in the ever-evolving age of precision medicine.
Limitations
Several limitations should be acknowledged concerning the present review.
Firstly, different CT and pericardiocentesis systems (namely types of CT systems, as well as types of catheters) were used across the range of studies included. This could be a source of bias given that, as described above, there have been important technological developments over the years in the CT field.32,33
Secondly, different approaches to the PE (i.e. parasternal, subxyphoid, etc.) were applied.7,14,15,19,27 As described by Nour-Eldin and colleagues, this can be associated with different degrees of success in terms of drainage. 14 Also, contrast use differed between series, and as such this technical issue should be taken into consideration. 6,15,27 Thirdly, most studies included only a limited number of individuals, and data stems mainly from retrospective cohorts from single centres. As such, prior to generalization of these results to other organizational settings, further data seems justified. As previously described, the fact that in some studies patients were included after being deemed unsuitable for echocardiography-guided pericardiocentesis or after a failed attempt, whereas in others ‘all-comers’ could be included, may also be a source of bias which should be kept under consideration.
Albeit in the presence of these limitations, this systematic review presents a current and comprehensive synthesis concerning the state-of-the-art of CT-guided pericardiocentesis, according to the published literature.
Conclusion
CT-guided pericardiocentesis is a useful technique in the approach to PE, in several clinical scenarios. Although echocardiography-guidance presents an important improvement in the performance of pericardiocentesis (namely allowing bedside use, pivotal to the clinical care of the critical patient), the use of CT can be especially relevant in the postoperative period, as well as in individuals with suboptimal image quality (as assessed by echocardiography). Given the increasing number of invasive procedures, and the potential number of associated complications, as well as the potential impact of a PE in certain subgroups (such as postsurgical and oncologic patients) the role of CT-guided pericardiocentesis in the management of this entity should be reappraised in further studies.
Supplemental Material
Supplementary_file_1_and_2 – Supplemental material for Computed tomography-guided pericardiocentesis: a systematic review concerning contemporary evidence and future perspectives
Supplemental material, Supplementary_file_1_and_2 for Computed tomography-guided pericardiocentesis: a systematic review concerning contemporary evidence and future perspectives by Eduardo M. Vilela, Catarina Ruivo, Claudio E. Guerreiro, Marisa P. Silva, Ricardo Ladeiras-Lopes, Daniel Caeiro, Gustavo P. Morais, João Primo, Pedro Braga, Nuno Ferreira, José Pedro L. Nunes and Vasco Gama Ribeiro in Therapeutic Advances in Cardiovascular Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.