
Abstract
Objectives:
The objectives of this study were to evaluate the effectiveness of a physician notification system for atrial fibrillation (AF) detected on cardiac devices, and to assess predictors of anticoagulation in patients with device-detected AF.
Methods:
In 2013, a physician notification system for AF detected on a patient’s CIED [including pacemakers, implantable cardioverter defibrillators (ICD) or cardiac resynchronization therapy (CRT) devices] was implemented, with a recommendation to consider oral anticoagulation in high-risk patients. We prospectively investigated the effectiveness of this system, and evaluated both patient and physician predictors of anticoagulation, as well as factors influencing physician decision making in prescribing anticoagulation. Both uni- and multivariable analysis as well as descriptive statistics were used in the analysis.
Results:
We identified 177 patients with device-detected AF, 126 with a CHADS2 ⩾2. Only 41% were prescribed anticoagulation at any point within 12 months. On multivariable analysis, stroke risk as predicted by CHADS2 was not a predictor of anticoagulation. ASA use predicted a lower rate of anticoagulation (OR 0.39, 95% CI 0.16–0.97, p = 0.04); physicians in practice for <20 years were more likely to prescribe anticoagulation (OR 3.39, 95% CI 1.28–8.93, p = 0.01); and physicians who believed both cardiologist and family doctor should be involved in managing anticoagulation were more likely to prescribe anticoagulation (OR 3.28, 95% CI 1.02–10.5, p = 0.05).
Conclusions:
Patients on aspirin were less likely to be anticoagulated. Physicians in practice for <20 years and who believed that both the general practitioner and cardiologist should be involved in managing anticoagulants were more likely to prescribe anticoagulation.
Introduction
Nearly 800,000 people have a stroke every year in the United States. 1 Approximately 17% of strokes are immediately attributable to atrial fibrillation (AF), while 25% have no apparent cause and are labeled as ‘cryptogenic’. 2 Strokes related to AF are associated with ~50% increased risk of disability and death within 3 months compared to strokes related to other etiologies. 3 It is increasingly recognized that a large proportion of patients labeled with cryptogenic stroke have device-detected AF.4–6
Asymptomatic AF is frequently detected on pacemakers and defibrillators, and predicts an elevated risk of stroke. 7 Many patients with clinical and device-detected AF are not anticoagulated and remain at increased risk of stroke. 8 The decision to anticoagulate these patients should be individualized, considering the patient’s stroke and bleeding risk, among other factors. Perceived risk of anticoagulation, as well as physician inexperience, have previously been associated with a lower rate of initiating anticoagulation of AF. 9
We implemented a physician notification system for device-detected AF, with a recommendation to consider oral anticoagulation. We sought to assess its effectiveness, and evaluate what patient and physician factors might influence the decision to initiate anticoagulation, through a physician survey. No previous studies have reported on the effectiveness of a physician alert system for device-detected AF, and none have described patient and physician predictors of prescribing anticoagulation to patients with device-detected AF. Our objectives were twofold. First, to evaluate the effectiveness of a physician notification system for anticoagulation of device-detected AF; and second, to assess if patient or physician factors influence the decision to initiate anticoagulation in a patient with device-detected AF.
Methods
The pacemaker and defibrillator clinic at St. Boniface Hospital (Winnipeg, Canada) sees over 6000 patients annually. The clinic is staffed by nurses trained in cardiac device interrogation, with access to a cardiac electrophysiologist for troubleshooting. In 2013, a physician notification system for AF detected on a CIED was implemented. We prospectively evaluated a cohort of patients with AF detected on their CIED between March 2013 and January 2014.
The intracardiac electrograms of all atrial high-rate episodes were reviewed by a cardiac electrophysiologist experienced in device interrogation to confirm the presence of AF lasting ⩾30 s, as per ACC/AHA guidelines. 10 If AF was confirmed, the referring physician was sent a notification via facsimile regarding the presence of device-detected AF, along and a recommendation to consider oral anticoagulation in high-risk patients. Patients were included in the study if they had no previous diagnosis of AF and were not on anticoagulation at presentation.
PACEARTTM (Medtronic, Minneapolis, USA) – a proprietary database designed for cardiac device patients – was used to assess duration of AF, device type, and demographics. We reviewed electronic chart records for patient demographics related to stroke and bleeding risk. The provincial Drug Program Information Network provided patient anticoagulant prescriptions up to 12 months after physician notification. A survey (Appendix A) was sent to all referring providers to identify physician characteristics, including years of training, attendance at continuing medical education seminars on AF, attitudes and practices in anticoagulating AF, among other data.
Primary outcome was initiation of anticoagulation within 12 months. Univariable analysis was performed to identify factors that predicted initiation of anticoagulation. The Fisher exact test was used for categorical variables, Mann–Whitney U test for numeric variables. Multivariable analysis was performed using a stepwise logistic regression to assess whether physician or patient characteristics predicted anticoagulant initiation. Descriptive statistics were used to describe the reasons for not initiating anticoagulation. The sample size was not pre-calculated, but rather all patients over the study period were enrolled to provide maximum statistical power. Ethics approval was obtained through the University of Manitoba Research Ethics Board (REB) (H2014:367). The REB waived the need for informed consent for the present study as it posed minimal risk to the patient, and from the physician perspective completion and return of the survey constituted their consent to participate.
Results
Between 3 March 2013 and 31 January 2014, over 6000 patients had their cardiac devices interrogated. Of these, 217 patients were identified as having device-detected AF. A total of 177 patients from in-province with complete data available were included in the study (Figure 1). Patient demographics are summarized in Table 1. Fifty-four percent of patients were on ASA at baseline. The rate of anticoagulation at any point in 12 months was 41% for patients with CHADS2 ⩾2 (Figure 2). In January 2015, we sent 284 surveys out to the 239 physicians who had been notified of the presence of device-detected AF in the patient cohort (Figure 3). Some patients had more than one physician. We received 154 responses for a response rate of 54%. Thirty-nine surveys were excluded due to incomplete information. The CHADS2 score was ⩾1 in 96% of patients on whom surveys were completed, with 6 min or more of device-detected AF.
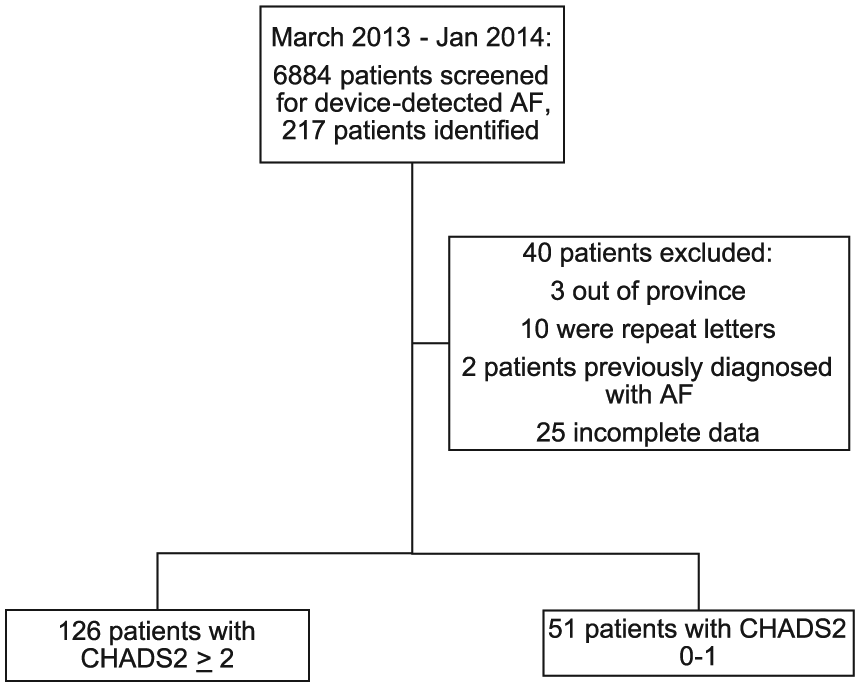
Patient identification and CHADS2 score.
Patient demographics.
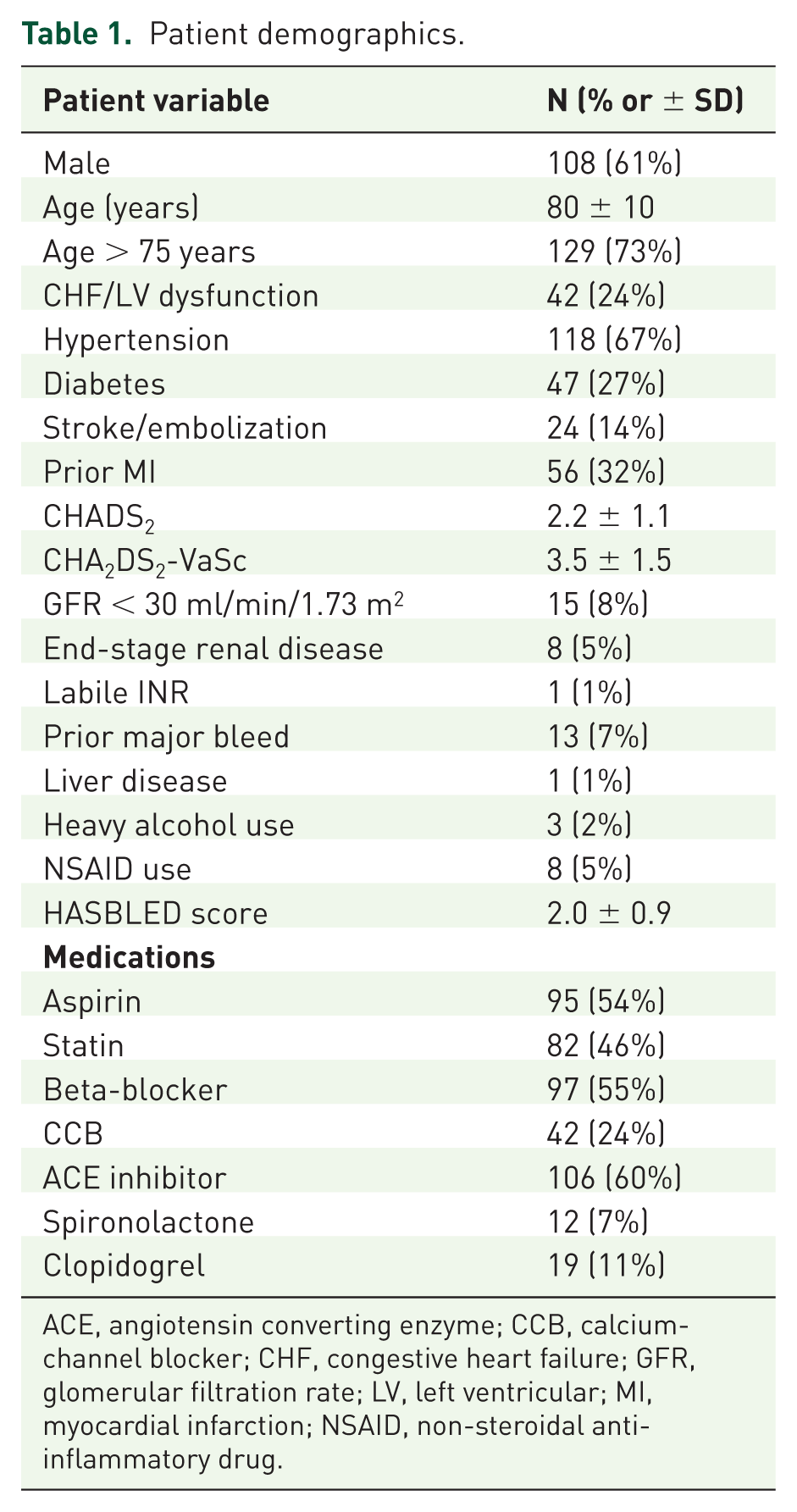
ACE, angiotensin converting enzyme; CCB, calcium-channel blocker; CHF, congestive heart failure; GFR, glomerular filtration rate; LV, left ventricular; MI, myocardial infarction; NSAID, non-steroidal anti-inflammatory drug.
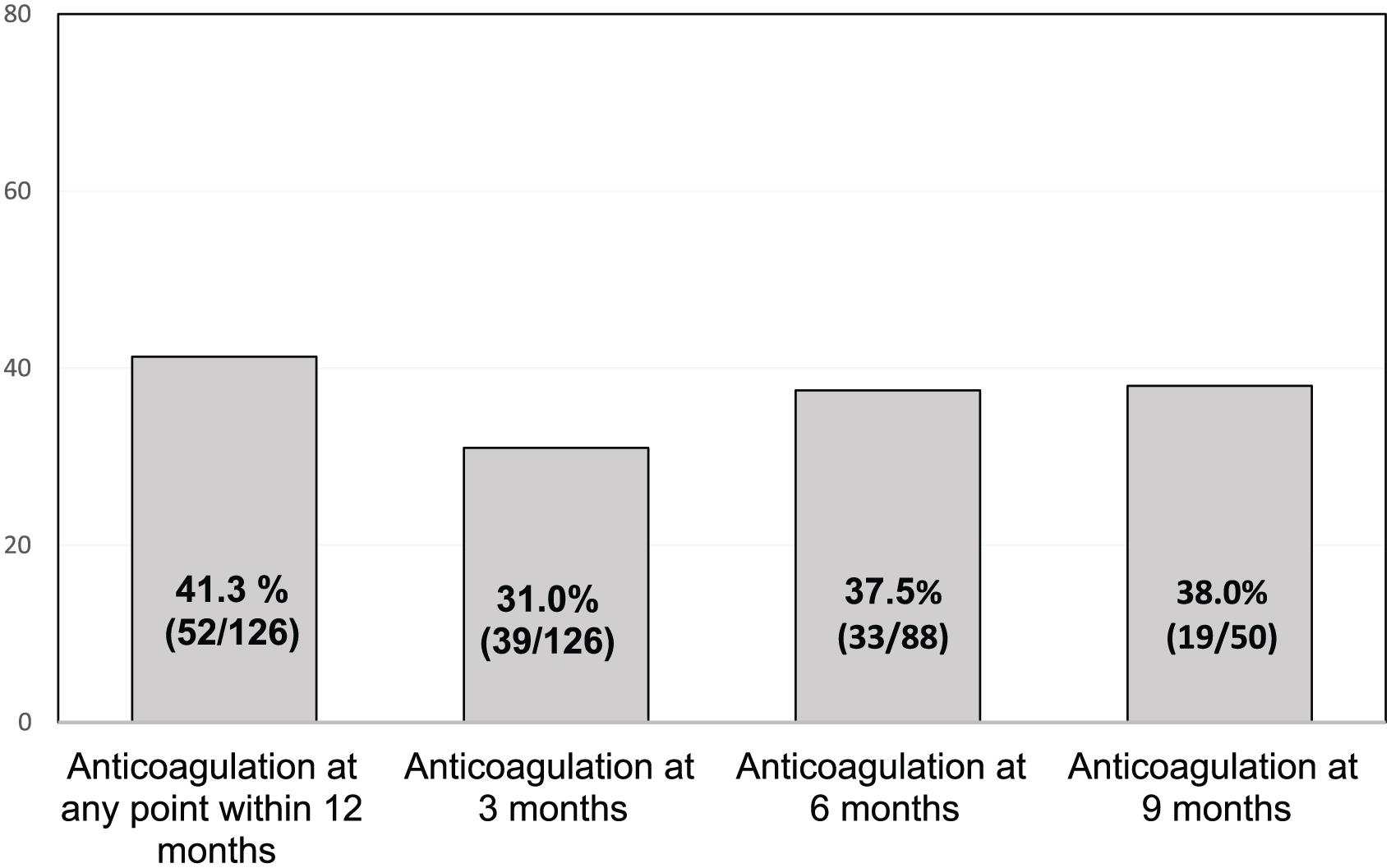
Anticoagulation rate of patients with device-detected atrial fibrillation and CHADS2 score ⩾2.
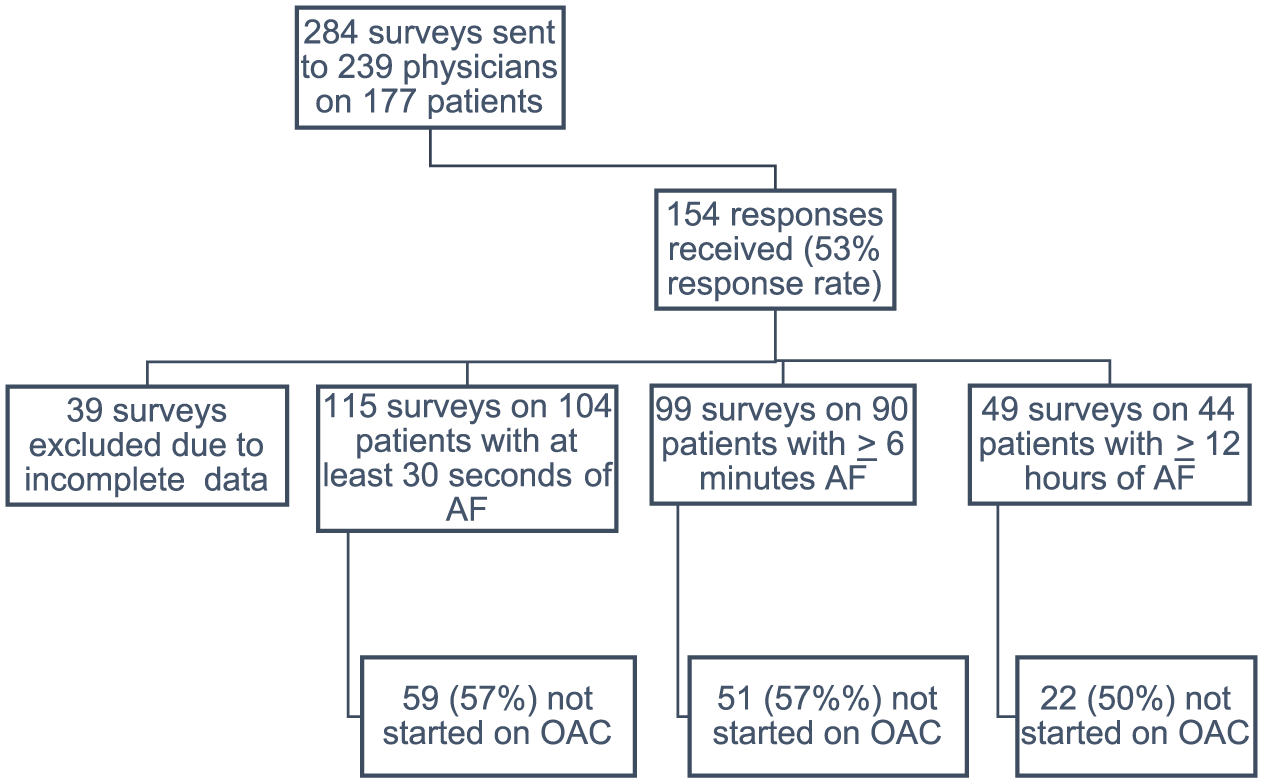
Physician survey responses and rate of anticoagulation stratified by duration of device-detected atrial fibrillation.
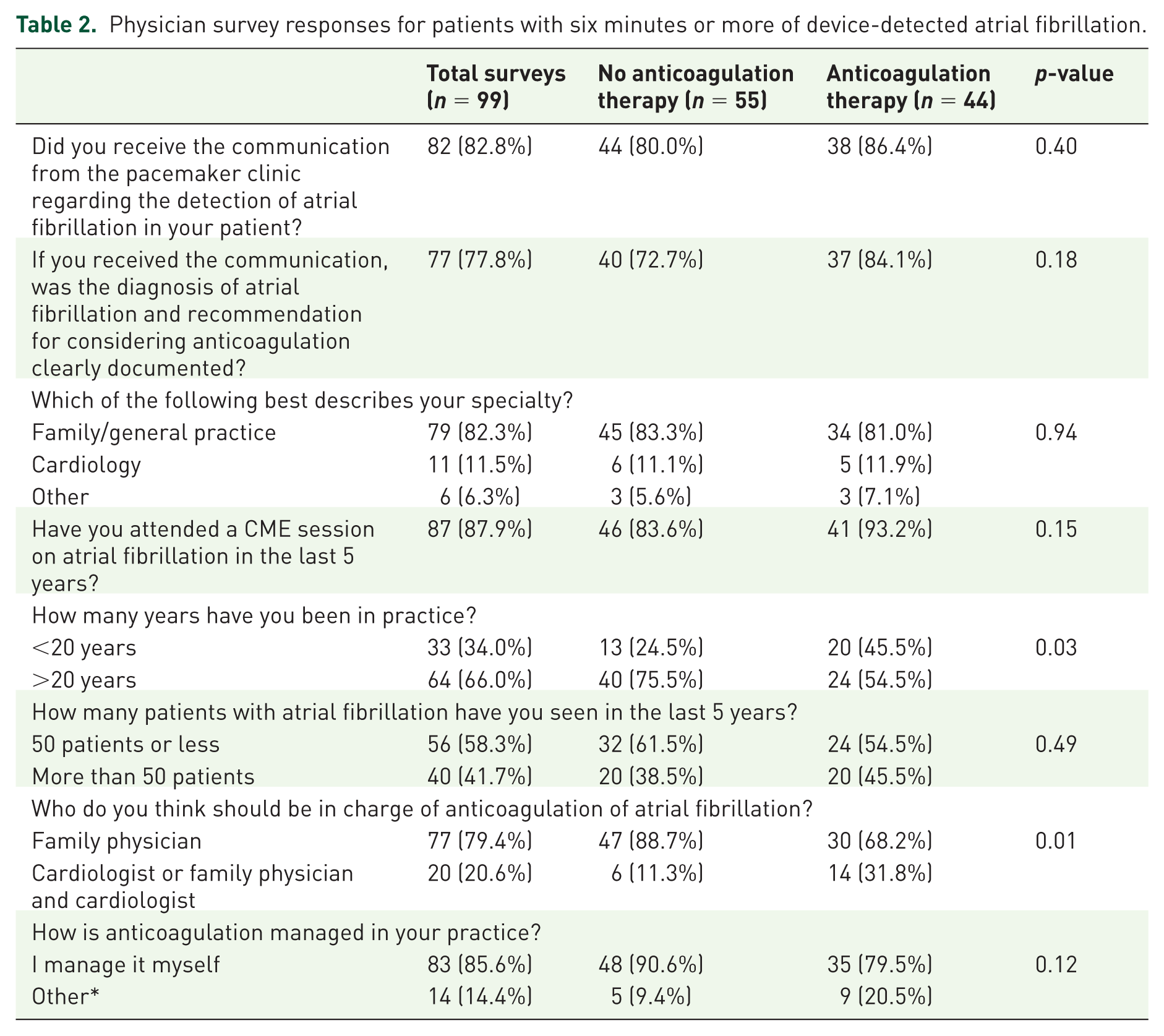
Physician survey responses and univariable analyses are summarized in Table 2 for patients with at least 6 min of AF. Most physicians responded by saying they had received the notification regarding the detection of AF on their patient’s CIED (83%, Table 2). Most respondents were family doctors, and most had attended a CME conference on AF in the previous 5 years. A majority of respondents reported managing anticoagulation on their own, and believed that a family physician ought to oversee anticoagulation, rather than a cardiologist. Physicians who had been in practice for >20 years were less likely to start their patient on anticoagulation, compared to those in practice for <20 years (76% were not anticoagulated, compared to 25% of patients with physicians in practice for <20 years (p = 0.03), Table 2).
Physician survey responses for patients with six minutes or more of device-detected atrial fibrillation.
Univariable analysis of patient factors predicting anticoagulation with at least 6 min of device-detected AF is shown in Table 3. Neither stroke risk as predicted by the CHADS2 score, nor bleeding risk as estimated by the HASBLED score were associated with anticoagulation. Multivariable predictors of anticoagulation for patients with more than six minutes of AF are shown in Table 4. Aspirin use predicted a lower rate of anticoagulation, with an odds ratio of 0.32 (95% CI 0.13–0.78). Physicians in practice for 20 years or less were more likely to prescribe anticoagulants than those in practice for longer than 20 years (OR 4.1, 95% CI 1.61–10.42, p < 0.01). Physicians who believed the family physician and cardiologist should share the responsibility of prescribing anticoagulants were also more likely to prescribe anticoagulants (OR 3.28, 95% CI 1.01–10.5, p = 0.05).
Patient factors predicting anticoagulation with at least 6 min of device-detected atrial fibrillation.
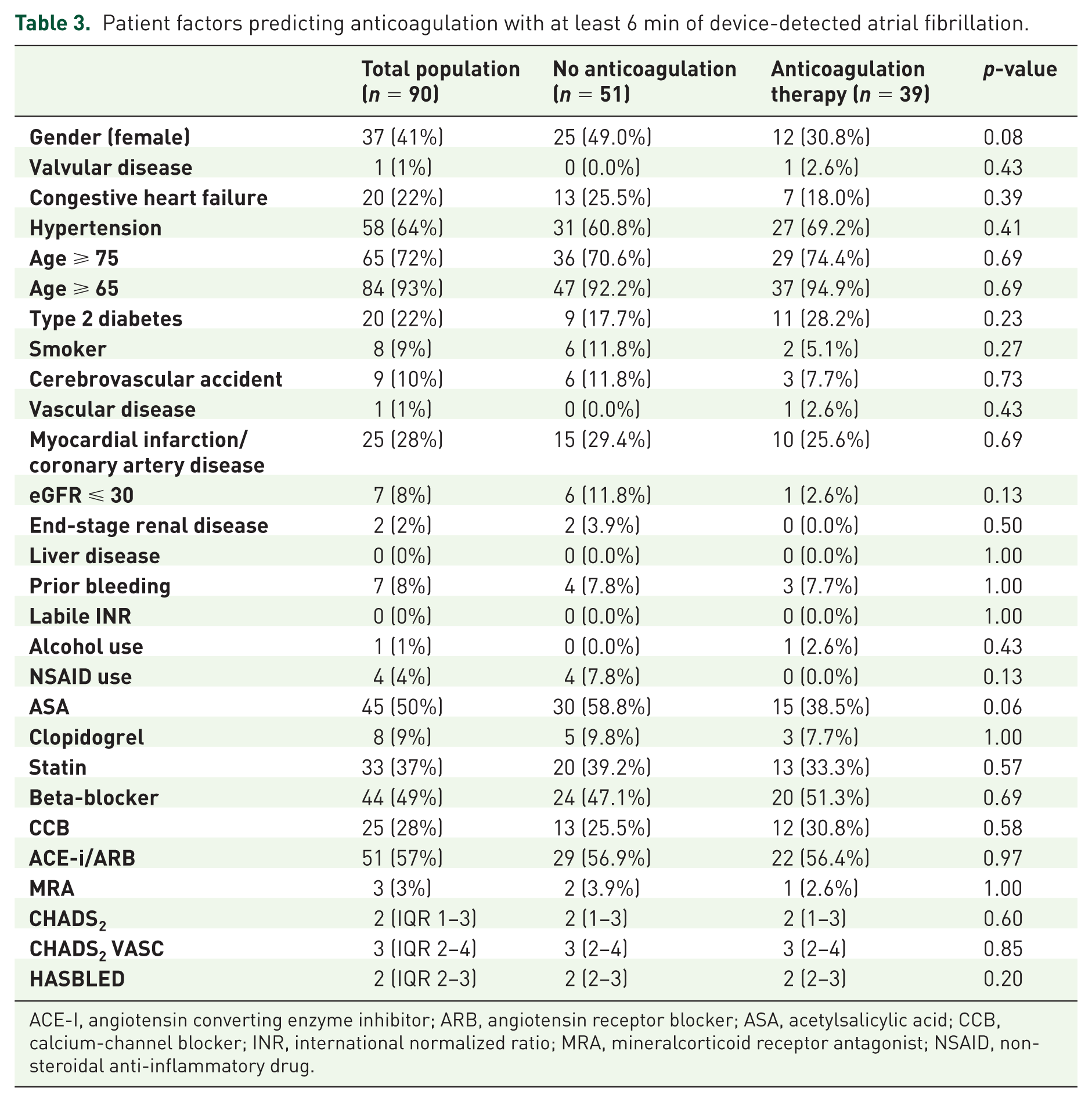
ACE-I, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; ASA, acetylsalicylic acid; CCB, calcium-channel blocker; INR, international normalized ratio; MRA, mineralcorticoid receptor antagonist; NSAID, non-steroidal anti-inflammatory drug.
Predictors of anticoagulation in patients with 6 min or more of device-detected atrial fibrillation (n = 99 surveys).
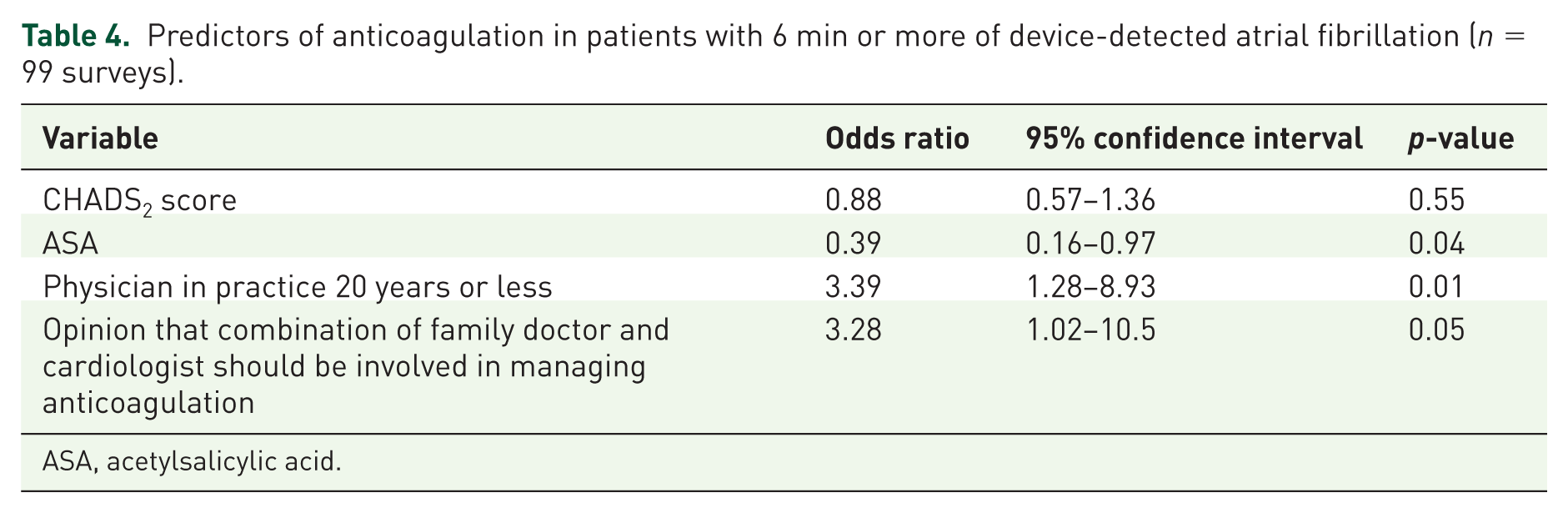
ASA, acetylsalicylic acid.
Discussion
We evaluated the effectiveness of a system alerting physicians to the presence of device-detected AF in a cohort of patients with elevated stroke risk. We found that our notification was widely received by the primary care providers, and that fewer than half of patients were started on anticoagulation. Stroke risk as indicated by CHADS2 was not associated with a higher rate of anticoagulation. Aspirin use predicted a lower rate of anticoagulation, while physicians who were of a collaborative belief regarding anticoagulation (involving both cardiologist and family physician), and physicians in practice <20 years, were more than three times more likely to prescribe anticoagulation to patients with device-detected AF. Our results suggest that there remains a belief in primary care that aspirin is adequate in preventing stroke in AF, despite data showing that it carries minimal to no benefit, with similar bleeding risk.11–13
Many patients worldwide with AF who have an increased risk of stroke and low risk of bleeding are not anticoagulated and remain at excessive risk of stroke.8,14–16 Reports have been published assessing factors that influence physician decision making in anticoagulating AF through case vignettes or general attitudes,17–30 with far fewer publications examining real-world practices and decision making at the individual patient level.31–33 Patient factors such as previous stroke,16,18,31 hypertension, 16 valvular disease, 16 and CHF 16 have been associated with a higher rate of anticoagulation in real-world studies. Previous bleed or risk of bleeding,18,31–33 paroxysmal AF,16,32 non-white ethnicity,16,31 younger16,31 and older age, 32 dementia, 31 lower functional status, 31 recurrent falls, 28 expected poor patient compliance, 18 perception of a high risk–benefit, patient contraindications, 17 and perceived low risk of stroke 18 have been associated with a lower rate of anticoagulation. In case vignettes and surveys of general attitudes, 20 bleeding risk,20,21,24 fall risk,18,24 monitoring18,20 and irreversibility 20 have been associated with a lower rate of anticoagulation use. With regards to physician factors, studies have identified physician experience with previous stroke 18 with a higher likelihood of prescribing anticoagulants. Primary care physicians have previously identified lack of time, laboratory result delays, medication interactions, fear of litigation and space constraints as barriers to anticoagulation. 23
There have been no published reports on physician attitudes toward anticoagulation of device-detected AF. We received a good response rate to our survey, and had a captive sample of patients in a large academic center with a catchment area of over one million patients. Limitations of our study include using pharmacy dispensary records as a surrogate for anticoagulant use, which would not account for medication samples. Furthermore, our study is a single-center experience, and the sample size was small, which may further bias results. Additionally, dispensary records were audited over a 12-month period, which might underestimate the rate of anticoagulation if the patient was prescribed anticoagulants after 12 months.
Although patients with device-detected AF are at increased risk of stroke, there is a lack of conclusive evidence to support widespread anticoagulation of device-detected AF, though randomized trials are underway. 34 Despite clinical equipoise, anticoagulation of patients with device-related AF and a high CHADS2 score is common practice.35,36
Current recommendations for anticoagulation of symptomatic AF do not differ based on duration. In patients with high stroke risk, it is reasonable to prescribe anticoagulation to patients with device-detected AF. 37 One recent randomized trial 38 evaluated the efficacy of using device-detected atrial arrhythmias to guide anticoagulation compared to routine clinical practice. They found no difference in their composite endpoint of stroke, major bleeding and systemic embolism. 38 However, the patients in this cohort were of relatively low stroke risk, anticoagulation was discontinued after freedom from device-detected AF for 30–90 days, and many of the subjects in the control group were started on oral anticoagulation. 38 On the other hand, a recent subgroup analysis from the ASSERT trial showed that only episodes of device-detected AF longer than 24 h were associated with increased risk of stroke. 39 Individualizing a patient’s risk–benefit ratio when considering anticoagulation in this patient population is a reasonable practice, given the often-devastating outcome of stroke.
In conclusion, we found that a large proportion of patients with device-detected AF were not started on oral anticoagulation and remain at increased stroke risk. A belief that aspirin is adequate in reducing stroke risk in AF persists. Physicians in practice longer than 20 years and who believe that anticoagulants should be managed without the input of a cardiologist were less likely to prescribe anticoagulation. As we learn more about the benefits of anticoagulation of device-detected AF, these results can guide future education programs and policy to increase uptake of anticoagulation in device-detected AF.
Footnotes
Appendix A. Physician Survey
1. Did you receive the communication from the pacemaker clinic at St Boniface Hospital regarding the detection of atrial fibrillation on patient X’s device?
____________________________________________________________________________________________________________________
□ Yes □ No
2. If you received the communication, was the diagnosis of atrial fibrillation and recommendations for considering anticoagulation clearly documented?
____________________________________________________________________________________________________________________
□ Yes □ No
3. Physician information
Which of the following best describes your area of specialty? (Circle): Family/general practice Internal Medicine Nurse practitioner Cardiology (nonEP vs EP) Other:______________
4. Have you attended a CME session on atrial fibrillation in the last 5 years?
____________________________________________________________________________________________________________________
□ Yes □ No
4a. How many years have you been in practice
____________________________________________________________________________________________________________________
□ Less than 5 years □ 5-10 years □ 10-20 years □ More than 20 years
4b. How many patients with atrial fibrillation have you seen in the past year?
____________________________________________________________________________________________________________________
□ Less than 10 □ 10-50 □ 50-100 □ More than 100
4c. Who do you think should be in charge of anticoagulation of atrial fibrillation?
____________________________________________________________________________________________________________________
□ Family physician □ Cardiologist □ Other (please describe): ________________
4d. How is anticoagulation monitoring handled in your practice?
5. Decision regarding oral anticoagulation
5a. What was the primary reason that you did not start oral anticoagulation on this patient
5b. Did you consider using a novel oral anticoagulant on this patient such as rivaroxaban (Xarelto), dabigatran (Pradaxa), or apixaban (Eliquis)? Why not?
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.