
Abstract
Background:
Control of blood pressure and reduction of cardiovascular risk factors are mandatory in patients with hypertension. The aim of this study was to determine the proportion of patients with controlled hypertension and to describe the cardiovascular risk profile in hypertensive patients followed by general practitioners (GPs) in Morocco.
Methods:
This national, observational, multicentre, prospective, longitudinal study of patients with newly diagnosed hypertension was carried out between September 2011 and December 2011. The use of antihypertensive drugs was evaluated at inclusion and after 3 months of follow up. Uncontrolled hypertension was defined as systolic blood pressure (SBP) ⩾ 140 mmHg or diastolic blood pressure (DBP) ⩾ 90 mmHg at 3 months of follow up. The SCORE scale issued by the European Society of Cardiology (ESC) was used to assess overall cardiovascular risk and probability of experiencing a cardiovascular event within 10 years.
Results:
A total of 909 hypertensive patients were recruited (62.4% female). Mean age was 56.8 ± 10.6 years. More than half of the patients (53.0%) were between 40–60 years and more than one-third (34.1%) were obese [body mass index (BMI) ⩾ 30 kg/m2]. There were significantly more obese females than males (p < 0.001). Over half of the patients (52.5%) had a high or extremely high cardiovascular risk. Abdominal obesity (measured as waist circumference) was the most common cardiovascular risk factor (61.7%) followed by age (40.5%), dyslipidaemia (36.3%) and diabetes (34.3%). Mean SBP decreased from 168.1 ± 14.8 to 138.3 ± 13.2 mmHg (p < 0.001) and mean DBP decreased from 93.0 ± 10.5 to 81.0 ± 8.6 mmHg (p < 0.001) after 3 months of treatment. Control of blood pressure was achieved in only 46.8% of patients. Poor compliance (17.1%) and a lack of treatment efficacy (16.9%) were the two main reasons for not achieving the blood pressure target.
Conclusions:
More than half (53.2%) of the hypertensive patients in our study did not achieve adequate blood pressure control during the 3-month follow-up period and had a high cardiovascular risk. More effective management of hypertension is required in primary care.
Introduction
Hypertension is extremely common worldwide and is one of the most important risk factors for cardiovascular disease including acute heart disease, myocardial infarction, cerebrovascular accidents, congestive heart failure, renal disease and peripheral vascular disease [Editorial, 2011; Kintscher, 2013; Girerd et al. 2012; Yoon et al. 2012].
In Morocco, the prevalence of hypertension in adults is 33.6% (30.2% in men and 37.0% in women) [Tazi et al. 2003]. The incidence of hypertension is increasing worldwide. Data from the National Health and Nutrition Examination Survey indicate that the prevalence of hypertension in adult Americans increased from 24.0% between 1988–1991 [Burt et al. 1995] to 33.5% between 2005–2008 [Roger et al. 2011]. According to the report of the American College of Cardiology, the prevalence of high blood pressure [systolic blood pressure (SBP) ⩾ 140 mmHg or diastolic blood pressure (DBP) ⩾ 90 mmHg] worldwide increased from 600 million individuals in 1980 to 1 billion in 2008 [Laslett et al. 2012].
Antihypertensive treatment reduces the risk of cardiovascular complications [Mancia et al. 2013]. Good efficacy and tolerability have been demonstrated for many antihypertensive drugs. However, several studies have shown that despite progress in the treatment of hypertension, adequate control of blood pressure remains poor [Ibrahim and Damasceno, 2012].
Scientific recommendations advise treatment strategies and the use of different classes of antihypertensive drugs depending on the profile of the patient [Blacher et al. 2013; Centre d’Hémodialyse de Meknès, 2010; Mancia et al. 2007; WHO, 1999]. The aim of this study was to describe the cardiovascular risk profile of patients with newly diagnosed/treated hypertension who consulted general practitioners (GPs) in Morocco. The study also evaluated the proportion of patients who achieved their blood pressure target after 3 months of follow up.
Methods
Study design and population
This national, epidemiological, observational, multicentre, prospective, longitudinal study was carried out in adult patients with newly treated mild-to-moderate hypertension between September and December 2011. Exclusion criteria included secondary hypertension.
GPs were randomly selected to participate in the study based on a national list of GPs. Each GP was asked to recruit 10 consecutive patients meeting the inclusion criteria. Taking into account an expected control rate of 25%, 3% precision and 20% drop out, the calculated sample size was 1000 patients. No treatment protocol was imposed on investigators. They prescribed antihypertensive treatments according to their usual practice.
Data collection
Sociodemographic and clinical data were collected from each patient at inclusion using a self-administered questionnaire. A follow-up visit was arranged for approximately 3 months later to evaluate treatment efficacy for each patient. This timeframe corresponds to the mean time between two routine visits for follow up in Morocco. At the follow-up visit, sociodemographic, anthropometric and blood pressure data were recorded. According to blood pressure measurements, the GPs made their own decision on whether to adapt or continue the antihypertensive treatment for each patient.
Patient confidentiality was respected according to local rules in force in Morocco. Written informed consent was obtained from each patient before inclusion.
Definition of hypertension and cardiovascular risk
Hypertension was defined and classified according to the 2007 recommendations of the European Society of Hypertension (ESH) and European Society of Cardiology (ESC) [Mancia et al. 2007]. Investigators were asked to measure blood pressure in both arms after a rest period of at least 10 min using a sphygmomanometer, according to World Health Organization (WHO) recommendations [WHO, 1999]. An average of three measurements were taken with an interval of 5 min between each. Hypertension was defined as SBP ⩾ 140 mmHg or DBP ⩾ 90 mmHg. The WHO classification of body mass index (BMI) was used to define obesity [WHO, 2000]. Abdominal obesity was defined by waist circumference measurement (males ⩾ 102 cm; females ⩾ 88 cm).
Patients were classified according to the severity of hypertension, but also in terms of overall cardiovascular risk, taking into account the presence of risk factors or presence of target organ damage and underlying disease. The risk factors influencing prognosis were defined according to ESC-ESH 2007 guidelines [Mancia et al. 2007]. Overall cardiovascular risk is split into four categories: low, moderate, high or extremely high. The antihypertensive drugs used were evaluated at inclusion and then after 3 months of therapy. The overall risk indicates the probability of experiencing a cardiovascular event within 10 years.
Statistical analysis
A descriptive analysis was performed on the sociodemographic, clinical and therapeutic characteristics of the patients. Classic tests for paired samples (Student’s t-test and Chi-square test) were used to compare qualitative and quantitative variables between baseline and follow-up visits. A p value <0.05 was considered statistically significant. SPSS version 17.0 (SPSS Inc., Chicago) was used for all statistical analyses.
Results
Study population
A total of 909 patients were included in the study. The characteristics of these patients at inclusion are shown in Table 1. The majority of the patients were female (62.4%). Mean age was 56.8 ± 10.6 years (range, 24–90) without any significant difference between the sexes. More than half of the patients (53.0%) were between 40–60 years of age and more than one-third (34.1%) were obese (BMI ⩾ 30 kg/m2). There were significantly more obese females than males (41.0% versus 22.5%; p < 0.001).
Characteristics of the study population at inclusion.

Data are presented as the mean ± standard deviation, or n (%).
p < 0.001 and ‡p < 0.05.
BMI, body mass index.
Cardiovascular risk and blood pressure
Table 2 shows the cardiovascular risk factors for the patients at inclusion. Abdominal obesity (measured as waist circumference) was the most common risk factor (61.7%) followed by age (male > 55 years; female > 65 years) (40.5%), dyslipidaemia (36.3%) and diabetes (34.3%). Cardiovascular or renal diseases were uncommon (2.2–3.3%) in the hypertensive patients in this study (Table 3). Clinical damage to target organs was also uncommon in our patients and did not exceed 6.1%.
Distribution of patients according to cardiovascular risk factor(s).
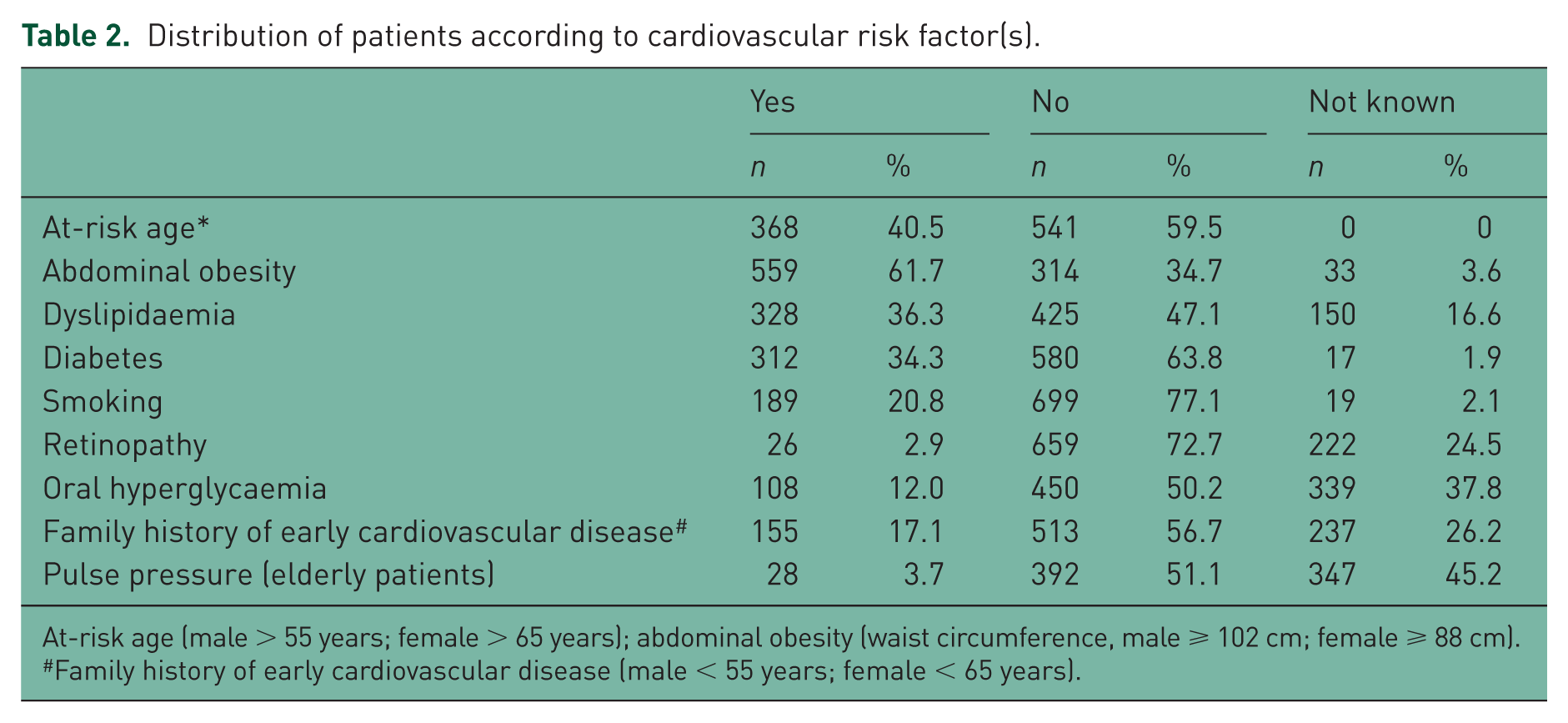
At-risk age (male > 55 years; female > 65 years); abdominal obesity (waist circumference, male ⩾ 102 cm; female ⩾ 88 cm).
Family history of early cardiovascular disease (male < 55 years; female < 65 years).
Distribution of patients according to the presence of proven cardiovascular or renal diseases and damage to target organs.

Cerebrovascular accident-ischaemic, haemorrhagic, transitory ischaemic; cardiopathy-infarct, coronary revascularization angina, heart failure; nephropathy-diabetic nephropathy, altered renal function (creatinine, male > 133; female > 124) or proteinuria (>300 mg/24 h); severe retinopathy-haemorrhages, exudates, œdema, papillary; LVH, electric-left ventricular hypertrophy, electric (Sokolow–Lyon>38 mm; Cornell>2400 mm*ms); LVH, echographic-(myocardial velocity gradient, male ⩾ 125 g/m2; female ⩾ 110 g/m2); carotid intima-media thickness > 0.9 mm or atheroma plaque; carotid-femoral pulse wave velocity > 12 m/s; ankle/brachial index < 0.9; glomerular filtration, estimated < 60 ml/min/1.73 m2 or clearance < 60 ml/min; microalbuminuria 30–300 mg/24 h or albumin/creatinine > 22 (male) and 31 (female) mg/g creatinine. It refers to the albumin/creatinine ratio i.e. albumin > 22 or 31 mg/g creatinine.
LVH, left ventricular hypertrophy.
The cardiovascular risk in our hypertensive patients according to ESH/ESC 2007 criteria is shown in Table 4. More than one-quarter of the population (29.4%) had an extremely high cardiovascular risk, 23.1% had a high risk and nearly half (45.3%) had a moderate risk. This shows that the majority of patients had the probability of developing a cardiovascular disease within the next 10 years.
Stratification of cardiovascular risk in the hypertensive patients according to ESH/ESC 2007 recommendations.

Data are shown as n (%).
DBP, diastolic blood pressure; ESC, European Society of Cardiology; ESH, European Society of Hypertension; HT, hypertension; SBP, systolic blood pressure.





SBP and DBP in our patients decreased significantly during the 3-month follow up with no significant difference between sexes (Tables 5). Mean SBP decreased from 168.1 ± 14.8 to 138.3 ± 13.2 mmHg, with an overall decrease of 29.9 ± 16.1 mmHg (p < 0.001), and mean DBP decreased from 93.0 ± 10.5 to 81.0 ± 8.6 mmHg, with an overall decrease of 12.2 ± 10.3 mmHg (p < 0.001).
Evolution of blood pressure after the 3-month follow up.

Data are presented as the mean ± standard deviation, or n (%).
p > 0.05 according to sex; ‡p < 0.001 comparison of mean blood pressure values between the inclusion visit and after the 3-month follow up.
DBP, diastolic blood pressure; SBP, systolic blood pressure.
At inclusion, the majority of patients had grade 3 (23.8%) or grade 2 (41.5%) hypertension and only 17.1% had grade 1 hypertension. After 3 months of treatment, 0.7% and 7.1% of patients had grade 3 and grade 2 hypertension, respectively. Isolated systolic hypertension decreased from 17.0% to 3.6% of patients during the 3-month follow-up period.
According to the GPs, the blood pressure target was reached in 57.2% of patients. However, according to ESH/ESC guidelines [Mancia et al. 2007], the blood pressure target, defined as SBP < 140 mmHg and DBP < 90 mmHg, was met by only 46.8% of patients (46.7% of females and 47.0% of males). At the 3-month follow up, if the blood pressure target had not been reached, investigators had to give their interpretation of the reason for noncontrol based on the anamnesis. Poor compliance (17.1%) and a lack of treatment efficacy (16.9%) were the two main reasons noted by the GPs (Table 6). The majority of patients (67.5%) continued with their treatment unchanged and the dose was increased in only 15.6% of patients. A switch to another treatment as monotherapy occurred in 13.8% of patients (Table 6).
Distribution of patients according to achievement of target objectives and actions taken by the GP.

Data are presented as n (%); *the target objective was chosen by the treating GP; **ESH/ESC 2007 recommendations.
ESC, European Society of Cardiology; ESH, European Society of Hypertension; GP, general practitioner.
Discussion
In this observational, prospective study of newly diagnosed patients with hypertension, control of blood pressure was achieved in less than half (46.8%) of our patients after 3 months of follow up. Over half of the patients (52.5%) had a high or extremely high cardiovascular risk.
In 2007, the WHO and International Society of Hypertension (ISH) published charts for risk prediction in hypertensive patients in 14 epidemiological subregions of the world [WHO, 2007]. The aim of these charts is to provide approximate estimates of cardiovascular disease risk in people who do not have established coronary heart disease, stroke or other atherosclerotic disease. Charts 12 and 14 in this publication show the 10-year risk of a fatal or nonfatal cardiovascular event according to sex, age, SBP, total blood cholesterol, smoking status and presence or absence of diabetes mellitus for patients in the eastern Mediterranean subregion D, which includes Morocco, with risk level ranging from <10% to >40% [WHO, 2007]. We could have selected this tool to estimate the risk factors in our patients but instead we choose to use the criteria defined by the ESH/ESC [Mancia et al. 2007].
The most recent data concerning hypertension control in North Africa come from the Epidemiological trial of hypertension in North Africa (ETHNA) study [Nejjari et al. 2012]. In this study, only 35.7% of patients had controlled hypertension. It was more common in younger than in older patients (p < 0.01), in females than in males (p = 0.01) and in patients from urban compared with rural areas (p = 0.00001). A higher level of education was also linked to better blood pressure control (p < 0.00001) [Nejjari et al. 2012]. In our study, we had a focus on newly diagnosed patients with mild-to-moderate hypertension. In this population, after 3 months of treatment, only 46.8% of hypertensive patients had normal blood pressure. According to current European recommendations [Mancia et al. 2013], the initial plan of care requires control of blood pressure between 3–6 months. The actions taken by the treating GPs during the second visit in our study (increasing the treatment dose in 15.6% of patients and changing to another monotherapy in 13.8%) could have resulted in an increase in number of patients with normal blood pressure. Conversely, poor control of blood pressure was probably due to poor compliance and lack of efficacy in 17.1% and 16.9% of our patients, respectively. The disparities in our series could also explain the results. A total of 40.5% of patients had an at-risk age. More than half of patients had a high or very high CV risk (respectively 23.1% and 29.4%). The prevalence of dyslipidaemia (36.3%) and diabetes (34.3%) is also a possible explanation for the poor control of blood pressure in our study.
In our study, a high cardiovascular risk was noted in over half of our hypertensive patients. This has been observed particularly in low and middle-income countries [Arima et al. 2011], but has less impact in developed countries. This shows the lack of education or awareness of the harmful consequences of hypertension in developing countries. Intensification of treatment in general practice and the search for ways of improving compliance will be key in preventing the increase in cardiovascular risk. To achieve this, increasing therapeutic education and the use of fixed-dose combinations could be solutions.
In Morocco, hypertension is one of the main reasons for consultation in outpatient services. As the cost of treatment of cardiovascular diseases is expensive, medical societies in collaboration with the Ministry of Health have developed recommendations for good medical practice in order to harmonize and optimize professional practices and to prevent cardiovascular complications by targeting risk factors and treating hypertension [Centre d’Hémodialyse de Meknès, 2010]. Nevertheless, our current study shows the discrepancies that exist between blood pressure targets considered by GPs, national and international recommendations. This can in part be explained by the weak implementation of local recommendations and the large number of different international guidelines.
Our study has several limitations. First, a single visit after the initiation of treatment (at 3 months) was probably insufficient to evaluate the degree of blood pressure control. Secondly, ‘smoking’ was not defined in this study. However, as we evaluated treatment following ESH/ESC guidelines, it can be assumed that the definition of ‘nonsmoking’ was the absence of smoking for more than 1 month. Thirdly, living conditions and level of education of the patients were not determined in this study. These factors could have affected our results since it has already been shown that an urban environment, consumption of salt and level of education can all affect the figures for blood pressure control [Arima et al. 2011; Ziyyat et al. 2014].
Conclusion
Our study, assessing newly diagnosed patients with mild-to-moderate hypertension over a 3-month treatment period, shows that blood pressure was not controlled in over half of our patients according to international recommendations. These findings, along with the high cardiovascular risk in the studied population, highlight the need for better management of hypertension in general practice in Morocco.
Footnotes
Acknowledgements
The authors would like to thank all of the physicians and patients who participated in this study. Editorial assistance with the preparation of the manuscript was provided by Newmed Publishing Services (Paris, France).
Funding
This survey was supported by Sanofi-Aventis (Sanofi Maroc, Casablanca, Morocco). Support for editorial assistance was also provided by Sanofi-Aventis.
Conflict of interest statement
MA, ME-A, AA and MB-G declare that there is no conflict of interest. MS and JS are employees of Sanofi-Aventis (Sanofi Maroc, Casablanca, Morocco).