
Abstract

Goal blood pressure in hypertension – current controversies
Data from observational studies suggest that cardiovascular morbidity and mortality is rising progressively starting at systolic blood pressure (BP) values as low as 115 mm Hg [Prospective Studies Collaboration, 2002]. Consequently, it would seem appropriate and logical to aim for such low BP values when managing hypertensive patients. However, to date, evidence for such a strategy is lacking since achieved systolic BP levels in the vast majority of the published hypertension intervention trials rarely reached significantly below 140 mm Hg [Mancia et al. 2013]. Furthermore, two recent treatment trials in which lower BP targets were investigated could not demonstrate an overall advantage of the intense treatment strategy.
Recent hypertension treatment trials with standard versus intense BP lowering
In the Secondary Prevention of Small Subcortical Strokes (SPS3) study, 3020 normotensive or hypertensive patients with a recent (within 180 days), symptomatic, magnetic resonance imaging (MRI) confirmed lacunar stroke were randomly assigned to a systolic BP target of 130–149 mm Hg or <130 mm Hg [SPS3 Study Group, 2013]. No significant reduction in the primary endpoint of that study, recurrent stroke [hazard ratio (HR) 0.81, 95% confidence interval (CI) 0.64–1.03, p = 0.08], as well as secondary endpoints such as myocardial infarction or total or cardiovascular mortality, were documented by the intense treatment strategy. However, the rate of intracerebral hemorrhage was reduced significantly with the lower BP target. In that study, treatment-related serious adverse events were infrequent [SPS3 Study Group, 2013].
Probably the strongest support against aggressive BP goals has been provided by the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial [ACCORD Study Group, 2010]. In that study, 4733 patients with type 2 diabetes were randomly assigned to intensive antihypertensive therapy, targeting a systolic pressure of <120 mm Hg or to <140 mm Hg (standard therapy) over a mean of 4.7 years. The primary composite outcome was nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes. No difference in the composite endpoint between the two treatment groups could be observed, but serious adverse events were significantly more common in the intensive therapy group. However, stroke rate, a prespecified secondary outcome, was significantly lower in patients randomized to intensive therapy [ACCORD Study Group, 2010].
It should be acknowledged, however, that the results of the SPS3 and ACCORD trials have been criticized, indicating that both studies were underpowered because of either an insufficient number of patients enrolled (SPS3) or a lower than expected event incidence (ACCORD) [Zanchetti et al. 2016].
The J-shaped curve
A possible rationale against more aggressive BP targets than presently recommended, as could be derived from the cited observational data, is based on the concept that longstanding hypertension may induce damage to the cardiovascular system necessitating higher perfusion pressures. Early evidence for such a J- or U-shaped curve relationship of BP and cardiovascular events in patients with long-standing hypertension was provided by data from the Framingham Heart Study demonstrating a J-shaped correlation for diastolic BP and coronary heart disease deaths in patients with myocardial infarction but not for low risk subjects without myocardial infarction [D’Agostino et al. 1991]. Similar findings, among others, were documented in a retrospective analysis of the International Verapamil-Trandolapril Study (INVEST) which included hypertensive patients with documented coronary artery disease [Bangalore et al. 2014; Messerli and Panjrath, 2009; Messerli et al. 2006].
It should be noted, however, that the method of plotting outcome against (achieved) BP may not be proof of a causal relationship of these two variables, but could rather be due to the fact that in elderly patients low diastolic BP may indicate more severe atherosclerotic disease and, consequently, a higher cardiovascular risk [Williams, 2009].
Taken together, current knowledge suggests that the relationship of BP and cardiovascular disease events obtained from observational studies cannot be reproduced in hypertension intervention trials published to date (Figure 1). Available evidence instead indicates that BP lowering will significantly reduce cardiovascular risk down to systolic BP values in the range of 130–150 mm Hg and that a lower target BP such as <120 mm Hg may selectively reduce stroke risk in certain subgroups such as patients with diabetes. However, aggressive BP lowering may carry the danger of increasing the risk of myocardial infarction, at least in patients with pre-existing coronary heart disease, and is associated with the risk of serious adverse events.
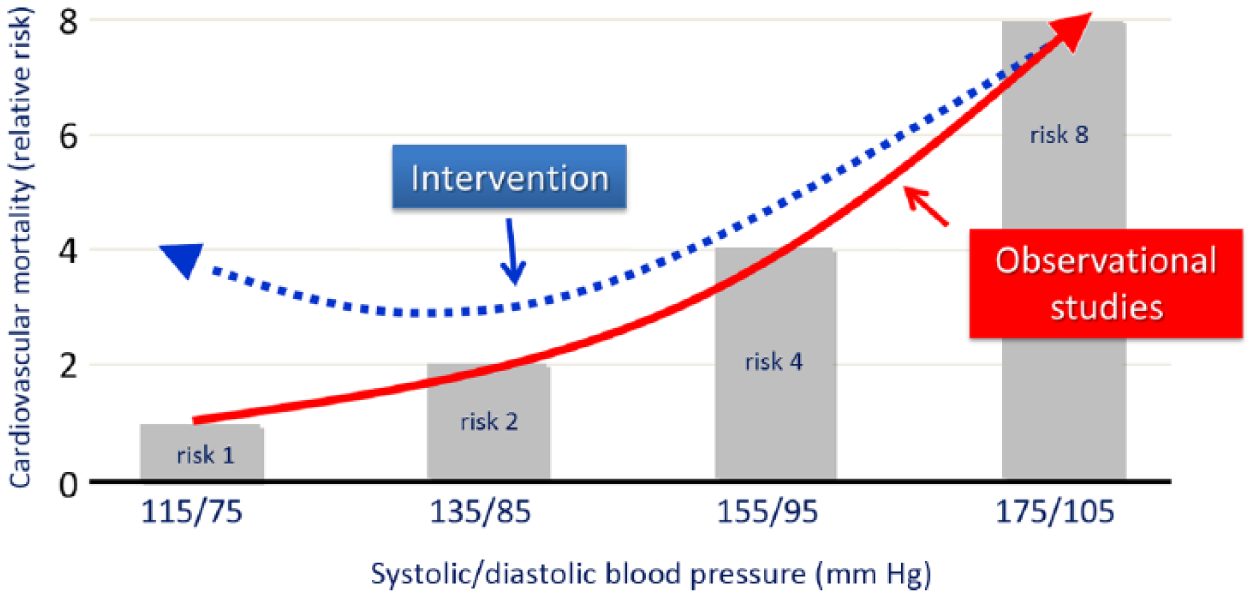
In observational studies, at ages 40–69 years, starting with blood pressure (BP) values as low as 115/75 mm Hg, each difference of 20 mm Hg systolic BP (or, approximately equivalently, 10 mm Hg diastolic BP) is associated with more than a 2-fold difference in the stroke death rate and with 2-fold differences in the death rates from coronary heart disease and from other vascular causes [Prospective Studies Collaboration, 2002]. In contrast, intervention studies have mostly shown that the prognostic benefit of BP lowering is usually achieved with BP values <140 mm Hg, with some variable additional stroke reduction with lower values.
Current guideline recommendations on BP goals
Consequently, on the basis of the available evidence from hypertension intervention trials, guidelines from all over the world recommend a target BP of <140/90 mm Hg in the general hypertensive population and even higher or modestly lower targets in certain subgroups. In this context, both the 2013 guidelines of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC) [Mancia et al. 2013] and the report of the panel appointed to the 8th Joint National Committee (JNC 8) [James et al. 2014] have recently recommended an increase in the target BP for patients ⩾60 years of age (without diabetes or chronic kidney disease) from <140 mm Hg to <150 mm Hg, arguing that the evidence for the <140 mm Hg goal in that particular age group was insufficient. However, this recommendation has created significant debate and has been criticized even by some members of the JNC 8 panel [Wright et al. 2014].
Systolic Blood Pressure Intervention Trial (SPRINT)
The global consensus on ‘conservative’ BP goals in the treatment of hypertension has recently been questioned by the results from a randomized trial of intensive versus standard blood pressure control (SPRINT) in which a goal BP of <140 mm Hg was compared with <120 mm Hg in 9361 persons (mean age 68 years, with 28% of participants ⩾75 years) with a systolic BP of ⩾130 mm Hg and an increased cardiovascular risk, but without diabetes [SPRINT Research Group, 2015]. The primary composite endpoint was myocardial infarction, other acute coronary syndromes, stroke, heart failure, or death from cardiovascular causes. The intervention was stopped early after a median follow up of 3.26 years owing to a 25% lower rate of the primary composite outcome in the intensive compared with the standard treatment group.
All-cause mortality was also significantly lower in the intensive treatment group, although significantly higher rates of some adverse events were observed with the lower target BP. Of special interest is the finding that intensive BP control reduced the primary endpoint at least as effectively in patients ⩾75 years of age compared with patients aged <75 years [SPRINT Research Group, 2015].
Congestive heart failure as an endpoint in hypertension trials
It should be noted that intense BP lowering in SPRINT had no effect on several secondary cardiovascular endpoints such as myocardial infarction, acute coronary syndrome and stroke, which have been part of a combined primary endpoint in most previous hypertension trials. This may, at least in part, be due to the premature interruption of the trial reducing its statistical power to detect differences between the two treatment arms [Zanchetti et al. 2016]. In SPRINT, the difference in the combined endpoint was essentially driven by the marked effect of the intense BP lowering protocol on heart failure, an endpoint more difficult to assess than other events that has been measured in only approximately half of the intervention trials in hypertension [Thomopoulosa et al. 2016]. In a recent meta-analysis of all published randomized treatment trials, stroke and heart failure were the outcomes most effectively prevented by BP lowering. No difference could be observed in the relationship of BP pressure reduction and the relative reduction in stroke and heart failure risk [Thomopoulosa et al. 2016].
The relative protection from heart failure compared with other cardiovascular endpoints may, among other factors, depend on the age of the patients included in a given trial. In the Hypertension in the Very Elderly Trial (HYVET), 3845 patients ⩾80 years of age with a sustained systolic BP of ⩾160 mm Hg were randomized to either placebo or antihypertensive drug treatment to achieve a target BP of <150/80 mm Hg. In these aged patients, drug treatment reduced myocardial infarction by 28%, stroke by 30% and new-onset heart failure by a remarkable 52% (intention-to-treat population) [Beckett et al. 2008]. Similarly in the Systolic Hypertension in the Elderly Program (SHEP), which randomized patients with isolated systolic hypertension aged ⩾60 years to either active treatment or placebo, BP lowering reduced heart failure by 49% with smaller effects on cerebrovascular and coronary heart disease events [Kostis et al. 1997; SHEP Cooperative Research Group, 1991].
The SPRINT study obviously adds new information to the complex interrelation of hypertension and congestive heart failure, showing that reducing BP to a lower than currently recommended goal will further reduce the incidence of that particular endpoint without significantly affecting coronary or stroke events.
Role of antihypertensive drugs
In the SPRINT trial, an average of 1.8 antihypertensive drugs in the standard treatment group and 2.7 drugs in the intensive treatment group were employed in the attempt to get patients to the respective goal BP. When looking at the details of the differences in drugs usage in the two treatment arms, diuretics were part of the treatment regimen in 42.9% of patients in the standard therapy and in 67.0% of patients in the intensive therapy group, mostly due to differences in the use of thiazide-type diuretics. Smaller differences were also present in the use of angiotensin converting enzyme (ACE) inhibitors (28.2% versus 37.0%), angiotensin receptor blockers (27.0% versus 39.7%) and beta-blockers (30.8% versus 41.1%) [SPRINT Research Group, 2015]. Therefore, it seems reasonable to speculate that the considerably higher use of diuretics and possibly also of other treatment options well documented in the treatment of congestive heart failure may have contributed to the marked reduction of this particular endpoint observed in SPRINT [Kjeldsen et al. 2016].
Generalizability of the SPRINT results
Including congestive heart failure as an endpoint and the differences in the use of diuretics and other cardiovascular therapeutics may help to explain why the SPRINT results differ from those obtained in other intervention studies, and especially the ACCORD trial restricted to patients with type 2 diabetes, which had a similar design as SPRINT.
However, in order to establish the clinical significance of the SPRINT trial, several additional factors should also be considered. Throughout the 3.26 years of follow up, mean systolic BP averaged 121.5 mm Hg in the intensive treatment and 134.6 mm Hg in the standard treatment group. Thus, it is obvious that the BP goal of <120 mm Hg was not achieved in the majority of patients in the intensive treatment group.
From the data published, it is impossible to construct precise distribution curves for on-treatment BP in the two groups of patients. A hypothetical curve is depicted in Figure 2. Despite all the possible uncertainties of this proposed BP distribution, a simple message may be conveyed. With the intensive BP lowering, a broad range of BP values was achieved around the mean value of 121.5 mm Hg with the majority of patients reaching a BP of 120–130 mm Hg rather than <120 mm Hg.

Hypothetical distribution of on treatment blood pressure (BP) values in the two treatment arms of SPRINT. The average on-treatment systolic BP values were 134.6 mm Hg in the standard treatment and 121.5 mm Hg in the intense treatment group.
Furthermore, it should be acknowledged that the BP measuring protocol in SPRINT was probably different from the procedure performed in many other hypertension trials and especially in everyday clinical routine. Patients were seated in a quiet area for 5 minutes. Then, BP was recorded by an automated unit that recorded three readings, separated by several minutes, with no clinician in the room. Decisions were based on the average of the three readings. It is obvious that this method of BP measurement yields lower readings than more rushed procedures taken by ‘white coat’ clinical personnel [Pickering et al. 2005].
Another important question reflects on the possibility of aggravating the decline in cognitive function by BP lowering, especially in elderly patients, which has been suggested from smaller studies with even less aggressive BP goals [Mossello et al. 2015; Peng et al. 2014]. Therefore, in addition to investigating cardiovascular endpoints, a SPRINT substudy (SPRINT-MIND) attempts to determine the effects of the two treatment strategies on cognitive function. The primary hypothesis of SPRINT-MIND is that the incidence of all-cause dementia will be lower in SPRINT participants assigned to the intensive BP treatment arm compared with their counterparts assigned to standard treatment. This hypothesis will be tested in all SPRINT participants. In addition, in a subgroup of 2800 patients, over an average of 48 months, the rate of decline in cognition will also be determined in the two treatment arms [https://www.nia.nih.gov/alzheimers/clinical-trials/systolic-blood-pressure-intervention-trial-memory-and-cognition-decreased; ClinicalTrials.gov identifier: NCT01206062].
An ongoing study, the European Society of Hypertension–Chinese Hypertension League Stroke in Hypertension Optimal Treatment randomized trial (ESH-CHL-SHOT) will help in clarifying some of the controversies with respect to BP targets [Zanchetti et al. 2014]. ESH-CHL-SHOT is a prospective multinational, randomized trial comparing three different systolic BP targets (<145–135, <135–125, <125 mm Hg). The trial is being conducted on 7500 patients aged at least 65 years (2500 in Europe, 5000 in China) with hypertension and a stroke or transient ischemic attack 1–6 months before randomization. Primary outcome is time to stroke (fatal and nonfatal). Secondary outcomes include cardiovascular events, cognitive decline and dementia.
Taken together, a careful approach to the generalizability of the SPRINT results seems critical. The majority of the SPRINT patients were not treated to below a systolic BP goal of <120 mm Hg, but rather <130 mm Hg. Also, when adjusting guideline recommendations on the basis of the office BP readings from SPRINT, the details of the BP measurement procedure in this study should be acknowledged and communicated. However, although not specifically investigated, SPRINT puts further doubt on current guideline recommendations from Europe and the USA to increase the systolic BP target in patients ⩾60 years of age from <140 mm Hg to <150 mm Hg [James et al. 2014; Mancia et al. 2013].
The outcome of the secondary endpoints of SPRINT, myocardial infarction and stroke, give further support to the concept that these two important events may not generally follow the rule of ‘the lower the better’. Why aggressive BP lowering markedly reduced strokes in patients with type 2 diabetes in ACCORD and not in patients without diabetes in SPRINT, at present, remains largely unexplained. However, SPRINT further supports the concept that, in elderly patients, heart failure may be the clinical event most effectively prevented by BP lowering and that this effect may even extend to lower on-treatment BP values than previously assumed.
Of great importance is the marked reduction in overall and cardiovascular mortality in the intensive therapy group with biggest differences in coronary heart disease mortality and sudden cardiac death. Whether these observed effects are consequence of the intensive BP lowering possibly mediated via a reduced heart failure risk, or mediated by some specific action of the drugs employed, remains unclear.
It should also be considered that the observed rates of serious adverse events of hypotension, syncope, electrolyte abnormalities, and acute kidney injury or failure observed in the intensive treatment group may be even more clinically relevant in a real world setting in which patient management is less tight than in a clinical trial.
Finally, before making far reaching decisions about more aggressive BP goals, the results of SPRINT-MIND and ESH-CHL-SHOT should be awaited.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares no conflicts of interest in preparing this article.