
Abstract
Background:
Hypertensive disorders of pregnancy (HDP) are the most important cause of maternal and fetal death and pregnancy complications in Latin America and the Caribbean.
Objectives:
The objective of this study was to characterize the epidemiological profile of women with HDP admitted to a Brazilian tertiary reference hospital, and to evaluate maternal and fetal outcome in each HDP and the impact of prenatal care on the maternal and fetal outcome.
Methods:
HDP in 1501 women were classified according to usual definitions as chronic hypertension (n = 564), pre-eclampsia (n = 579), eclampsia (n = 74) and pre-eclampsia/eclampsia superimposed on chronic hypertension (n = 284). Adverse maternal and fetal outcomes registered as maternal death and near miss and fetal outcomes documented as stillbirth, neonatal death and newborn respiratory complications were compiled. Prenatal care was classified as complete (⩾6 visits), incomplete (<6 visits) or not done.
Results:
Women with eclampsia were younger (15 years), 68% were on their first pregnancy, had higher blood pressure, higher mortality and greater number of near miss cases and their children had lower birth weight, higher intra-uterus and neonatal mortality, and more respiratory distress. Women with pre-eclampsia/eclampsia superimposed on chronic hypertension and their fetuses had intermediate outcome and those with chronic hypertension and pre-eclampsia the better outcome among those with HDP. Women who had incomplete prenatal care or prenatal not done had progressive higher mortality rates and greater frequency of near miss cases, and their children had higher mortality rates.
Conclusion:
In a tertiary reference hospital, eclampsia and chronic hypertension superimposed on pre-eclampsia are associated with a worst outcome for mothers and fetuses, whereas complete prenatal care is associated with a better maternal and fetal outcome in HDP.
Keywords
Introduction
Hypertensive disorders of pregnancy (HDP) are among the leading causes of maternal mortality, hospitalization due to clinical complications and deterioration of maternal and fetal prognosis [Hutcheon et al. 2011; Khan et al. 2006; Moussa et al. 2014; Say et al. 2014]. It is estimated that hypertension complicates about 5–10% of all pregnancies, although the incidence may vary according to the characteristics of the studied population and the criteria used for diagnosis [Abalos et al. 2014; Hutcheon et al. 2011; Moussa et al. 2014; Say et al. 2014]. In addition, low socioeconomic levels are associated with increased risk of complications related to HDP [Abalos et al. 2014; Hutcheon et al. 2011; Khan et al. 2006; Moussa et al. 2014; Say et al. 2014].
According to the World Health Organization (WHO), hypertensive disorders are the cause of most of the maternal deaths (25.7%) in Latin America and in the Caribbean and are, therefore, considered the main complications for pregnant women in these areas [Abalos et al. 2014; Khan et al. 2006]. In addition, the incidence is influenced by existing previous gestations. In nulliparous, it ranges from 3% to 7% and in multiparous from 0.8% to 5% [Abalos et al. 2014; Khan et al. 2006]. Ethnic, individual, environmental and socioeconomic factors, as well as the inherent factors of pregnancy, also have an influence on the incidence [Abalos et al. 2014].
HDP are usually classified as chronic hypertension existing before the pregnancy, those induced by pregnancy such as pre-eclampsia/eclampsia and gestational hypertension, and those aggravated by pregnancy such as pre-eclampsia superimposed on chronic hypertension [Brown et al. 2001; Magee et al. 2014; Moussa et al. 2014].
Eclampsia is the most severe form of the HDP. It is accompanied by high maternal and fetal mortality and morbidity, especially in underdeveloped or developing countries. According to some studies, eclampsia is responsible for nearly 50,000 annual maternal deaths [Bhutta and Black, 2013; Khan et al. 2006; Say et al. 2014]. It is estimated that, in developed countries, the incidence of eclampsia is around 1: 330 births, while in university hospitals in Brazil it occurs in approximately 1% of pregnancies [Abalos et al. 2014; Khan et al. 2006; Zanette et al. 2014]. Complications depend on several variables directly linked to mother and neonate, as well as quality of care, whether in primary, secondary or tertiary centers, where there is intensive care [Souza et al. 2013].
Some potentially serious conditions such as placenta previa, disseminated intravascular coagulation, cerebral hemorrhage, pulmonary edema, hepatic insufficiency and acute renal failure are often associated with HDP, worsening the maternal prognosis. Regarding the fetus, perinatal complications include prematurity, fetal growth restriction, fetal distress and perinatal death.
Despite all the recent progress in medicine, especially related to HDP, in developing countries there are still high rates of maternal death and complications associated to HDP. This is in contrast with developed countries where these events have progressively decreased, mainly due to the quality of prenatal care [Bhutta and Black, 2013; Lozano et al. 2011; Saleem et al. 2014; Souza et al. 2013; Say et al. 2014].
This study aims to evaluate the maternal epidemiological profile and the impact of proper prenatal care on the fetal and maternal outcomes of women with HDP assisted in a tertiary university hospital that covers an area with about 3 million inhabitants.
Methods
This was a retrospective cohort study that included all women with HDP admitted to a tertiary hospital in a 4-year period. HDP were classified as chronic hypertension when blood pressure (BP) >140/90 mmHg was diagnosed prior to the onset of pregnancy or before the 20th week of gestation. Pre-eclampsia was defined as the presence of hypertension (BP > 140/90 mmHg) associated with proteinuria (>300 mg/24 hours or 300 mg/g creatinine) in previously normotensive women. Eclampsia was defined as the occurrence of convulsions and/or coma not associated to other cerebral disorders in women with pre-eclampsia. Seizures were of grand mal type and could be present before labor, during labor or up to 48 hours postpartum. Pre-eclampsia/eclampsia superimposed on chronic hypertension was defined as chronic hypertension accompanied by pre-eclampsia or eclampsia [Brown et al. 2001]. Maternal near miss was defined as mothers who survived a severe gestational complication characterized by any clinical or laboratorial vital organ dysfunction (cardiovascular, respiratory, neurological, renal, coagulation, hepatic, uterine) [Say et al. 2009]. Although potentially reversible with appropriated treatment, seizures were considered a life-threatening condition and included as neurological dysfunction. Maternal and fetal perinatal outcomes were monitored and registered by a single investigator (J.L.G.N.) from the admission to hospital discharge or death.
Gestational age was calculated from the date of last menses. Reported BP values are those obtained 6 hours after hospital admission.
The study was conducted according to Helsinki Declaration principles and was approved by an independent ethics committee.
For statistical analysis of normal distribution parametric data, we used analysis of variance (ANOVA) to evaluate if there were any differences between groups; when differences where present, the Tukey–Kramer test to identify the differences. Test of proportions we used to evaluate if there were differences between two proportions. Odds ratio were used to compare the association of maternal and fetal complications with prenatal care. All statistical calculi were performed in MedCalc® statistical software [MedCalc Software, 2015]
Results
During the 4-year period, a total of 1501 women with hypertension disorders of pregnancy were admitted and followed up. Chronic hypertension was diagnosed in 564, pre-eclampsia in 579, eclampsia in 74 and pre-eclampsia/eclampsia superimposed on chronic hypertension in 284. Table 1 shows a summary of their demographic, clinical and gestational parameters. As one may observe, pregnant women with chronic hypertension were older and those with eclampsia, the youngest, only 15 years old on average. In addition, there was a smaller proportion of white women in the eclampsia group than in the group of women with chronic hypertension and superimposed pre-eclampsia. Gestational age at delivery was higher in the pre-eclampsia group and lower in the eclampsia group compared with those with chronic hypertension alone or with superimposed pre-eclampsia. The proportion of women in their first pregnancy was different among all groups, and expressively higher in the groups with pre-eclampsia and eclampsia. Diastolic BP at admission differed between groups, being lowest in the chronic hypertension group and highest in the eclampsia group.
Demographic parameters of the women admitted with hypertensive disorders of pregnancy.

Mean ± standard deviation.
p < 0.0001 versus other groups.
p < 0.01 versus other groups.
p = 0.04 versus superimposed pre-eclampsia.
Gestational age at delivery.
Diastolic blood pressure at admission.
Table 2 shows maternal and fetal outcomes related to HDP. Women with isolated pre-eclampsia had the lowest proportion of maternal death (<1%), not different from chronic hypertension. Those with eclampsia had the highest maternal mortality (about 8%) and women with superimposed pre-eclampsia an intermediary proportion of maternal death (approximately 2.5%). All groups of women with HDP had high proportion of stillbirth (close to 10%), being lowest in the group of mothers with pre-eclampsia compared with the other groups, which differ statistically only from the group of mothers with chronic hypertension (p = 0.02). When we consider fetal loss, stillbirth plus neonatal mortality (up to 28 days after birth), it is possible to observe the vulnerability of the neonates of women with eclampsia, being close to 27%, higher than all other groups of mothers with HDP. Respiratory newborn complications (anoxia and/or respiratory distress) were also high in all groups (14–23%) and differed statistically only when comparing newborns of mothers with pre-eclampsia with those of mothers with chronic hypertension. The average birthweight of neonates was low for all groups of women with HDP (about 2800 g), and statistically different in the group of women with eclampsia (about 2100 g, p < 0.0001).
Maternal and fetal outcomes related to hypertensive disorders of pregnancy.
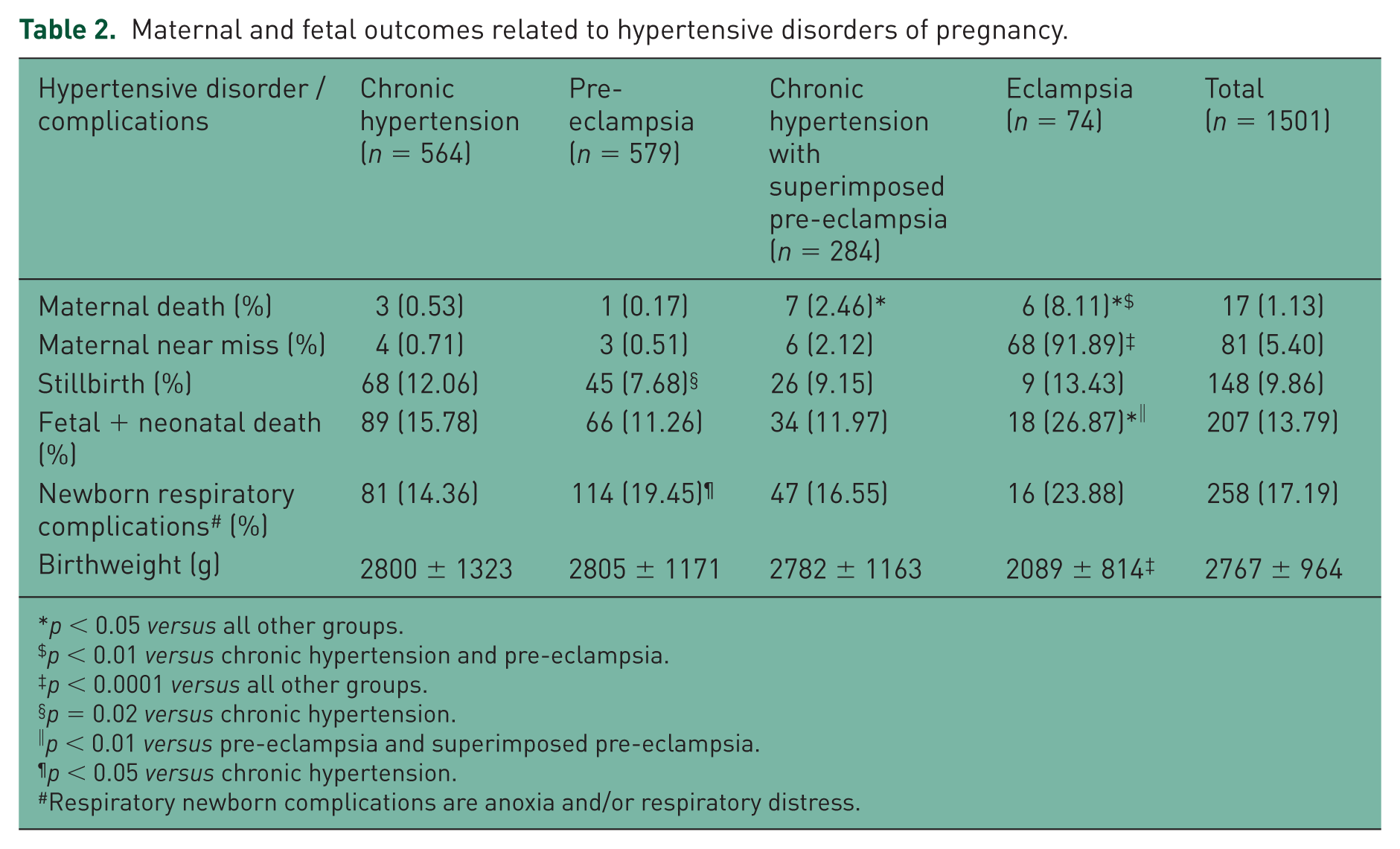
p < 0.05 versus all other groups.
p < 0.01 versus chronic hypertension and pre-eclampsia.
p < 0.0001 versus all other groups.
p = 0.02 versus chronic hypertension.
p < 0.01 versus pre-eclampsia and superimposed pre-eclampsia.
p < 0.05 versus chronic hypertension.
Respiratory newborn complications are anoxia and/or respiratory distress.
Table 3 shows maternal and fetal outcome of women with HDP in relation to prenatal care. The proportion of women with complete prenatal done (⩾6 visits) was low (about 57%). About 8% of them did not have any prenatal care. One may observe that, compared with those with complete prenatal care (reference), women with incomplete prenatal care or prenatal care not done had progressive risk of death and severe clinical complications (near miss), and their children had a higher chance of stillbirth or neonatal death.
Maternal and fetal outcome of women with hypertensive disorders of pregnancy: relationship to prenatal care.

p values as compared with complete prenatal care (reference).
CI, confidence interval.
Discussion
As expected, our study showed that women with eclampsia were very young (mean age of 15 years) and those with chronic hypertension the oldest, about 33 years old (Table 1). Women with eclampsia were also more frequently nonwhite, predominantly in their first pregnancy (68%), had the highest BP and the lowest gestational age at delivery compared with the other HDP groups. Some aspects of this study differ from populational studies, particularly the frequency of the different HDP, probably because our data were collect exclusively in a single tertiary hospital, reference for a region of about 3 million inhabitants. We had predominance of chronic hypertension isolated or superimposed on pre-eclampsia, whereas in populational studies, particularly in Latin America, pre-eclampsia is usually the more frequent HDP in general hospitals [Abalos et al. 2014].
According to WHO 2013 report, maternal mortality in Brazil at the time of this study was 0.07% [Say et al. 2014]. Our study shows that, even in this relatively well developed area in Brazil, (São Paulo state), HDP continue to be an important cause of maternal, intra-uterus and newborn death (Table 2). In this study, maternal deaths (⩽0.53%) and near miss cases are relatively low in women with chronic hypertension or pre-eclampsia compared with those with eclampsia (8%) or pre-eclampsia/eclampsia superimposed on chronic hypertension (about 2.5%), but still 10 times higher than in women without HDP (0.05%) (Table 2) [Abalos et al. 2014]. Women with eclampsia had a 16 times higher mortality than those with chronic hypertension and almost 50 times higher mortality compared with those with pre-eclampsia. The WHO populational study also showed a very high mortality rate in women with eclampsia (3.66%) [Abalos et al. 2014].
Fetal and neonatal mortality, as well as newborn respiratory distress, was very high in all HDP, being highest in eclampsia (Table 2). Chronic hypertensive disorder of pregnancy, frequently unvalued, is a very important risk factor for fetal death and newborn respiratory complications. Also, birthweight was particularly lower in children of women with eclampsia. In addition, several other recent studies also observed high maternal and fetal mortality associated with HDP in Brazil [Abalos et al. 2014; Say et al. 2014; Zanette et al. 2014].
Finally and most important, the study demonstrated that complete prenatal care is associated with lower risk of severe maternal, fetal and newborn morbidity and mortality (Table 3). About 8% of gestations had no prenatal care at all, whereas 35% had incomplete prenatal care (<6 visits) and 57% had complete prenatal care. Roughly, two-thirds of cases of maternal death, stillbirth or perinatal death occurred in women with prenatal incomplete or not done. Thus, maternal and fetal outcome are strikingly influenced by prenatal care. Unfortunately, our study did not collect socioeconomic data that could allow their correlation to maternal and fetal outcomes in each HDP. However, the study findings confirm an important observation to reinforce the key role of the prenatal care, an inexpensive, feasible and effective strategy to save lives.
In 2000, the United Nations General Assembly adopted the ‘United Nations Millennium Declaration’ in which all leaders had a commitment that, by the year 2015, eight crucial world problems should be minimized; these became known as the ‘Millennium Development Goals’ [United Nations, 2000]. Reducing maternal mortality by three-quarters and the mortality of children under 5 years old by two-thirds are among these goals [United Nations, 2000].
Some working groups are proposing interventions to reduce maternal and fetal mortality and life-threatening complications related to HDP, among them, use of low-dose aspirin, calcium supplementation, adequate treatment of severe high BP and management of HDP, and a continuum care during pregnancy and at delivery, including an integrated model to estimate the risk [Henderson et al. 2014; Lassi et al. 2014; Magee et al. 2014; Moussa et al. 2014; Payne et al. 2014; Vogel et al. 2014]. Although consistent progress has been achieved due to local and global initiatives, HDP continue to be a major contributor to maternal deaths in developing countries, particularly in Latin America and the Caribbean [Bhutta and Black, 2013; Lozano et al. 2011; Saleem et al. 2014; Souza et al. 2013; Say et al. 2014]. Thus, our study shows that providing an appropriated prenatal care may decisively contribute to achieve this important global goal.
Footnotes
Acknowledgements
IRCB, WBMS and GSGC received scholarship from the Brazilian National Research Council (CNPq) and Pontifícia Universidade Católica de São Paulo (PUC-SP).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.