
Abstract
Background:
Blood viscosity has a role in modulating cardiovascular homeostasis; changes in this parameter have been associated with cardiovascular mortality and morbidity. However, it remains unclear whether these changes are (1) involved in the pathophysiology of disease, (2) an epiphenomenon, or (3) the expression of counterregulatory mechanisms. We report data on the normal values of blood viscosity and its association with cardiovascular risk factors, prevalent cardiovascular disease, and blood pressure in a large population-based cohort study.
Methods and results:
Viscosity was calculated using validated formulae and its associations were explored in 15,010 participants (mean 55.0, min–max: 35–74 years old; 49.5% women) from the Gutenberg Health Study as well as in a subgroup of 3223 subjects (61.1% women, mean age 49.2, min–max 35–74 years old) without risk factors or self-reported cardiovascular disease. Age- and gender-adjusted mean values for viscosity were defined. Regression models showed a relationship between classical risk factors and blood viscosity measures; the overall R2 of the multiple linear regression model was however as low as 0.067 and 0.049 for high and low shear stress viscosity, respectively. After correction for cardiovascular risk factors, there was a very mild association between viscosity and prevalent coronary artery disease and heart failure. Systolic, mean and diastolic blood pressure increased with increasing blood viscosity after correction for age and gender.
Conclusions:
We provide reference values for viscosity in a population-based cohort. Blood viscosity decreases in older subjects and shows a very mild association with cardiovascular risk factors and prevalent disease in our cohort. There is a linear positive association between viscosity and blood pressure.
Introduction
The impact of blood viscosity on cardiovascular homeostasis remains incompletely understood. In the traditional view, abnormalities in blood viscosity have been associated with decreased tissue perfusion and with the development of atherosclerosis and arterial hypertension, such that it has long been proposed that blood viscosity should be considered among cardiovascular risk factors [Lowe, 1986; Forconi et al. 1987; Lowe, 1992; Becker, 1993; Kesmarky et al. 1998; Yarnell et al. 2004; Jeong et al. 2010; Sloop et al. 2014]. Increased blood viscosity has been associated with hypertension, peripheral vascular disease, diabetes mellitus, coronary artery disease, and it has been proposed that it might act synergistically with atherosclerosis and microvascular dysfunction in determining an increase in vascular resistances associated with a decrease of capillary perfusion, thus promoting myocardial, cerebral and/or peripheral ischemia and increasing cardiovascular mortality (see the review and meta-analysis in Danesh et al. 2000). Some controversy however still exist, and some authors have proposed that a more complex relationship between blood viscosity and cardiovascular disease might exist [Forconi et al. 1987; Forconi and Gori, 2009]. For instance, small changes in viscosity above the normal values have been associated with a decrease in blood pressure, an observation that has been explained as the result of the stimulation of endothelium-dependent vasodilation mediated by the increased shear stress [Salazar Vazquez et al. 2010]. Similarly, increased viscosity is associated with longer erythrocyte transit time through the microvascular bed, which also improves tissue oxygen extraction [Salazar Vazquez et al. 2009]. Based on these considerations, it has been proposed that the increased blood viscosity observed in the presence of cardiovascular disease (secondary hyperviscosity syndromes) might represent a compensatory mechanism finalized at activating endothelial function and improving tissue perfusion.
Blood viscosity is usually neither directly measured nor indirectly calculated in clinical practice. Further, the distribution of the reference values of this parameter stratified by age, gender, and for the presence of cardiovascular conditions has not been defined. Few studies have investigated the relation of whole blood viscosity (WBV) with standard cardiovascular risk factors at a population level, and data on the association between WBV and demographic and laboratory variables in large cohorts are not available. Finally, the association between WBV and arterial blood pressure remains controversial. We report data from 15,010 participants in the Gutenberg Health Study, a population-based cohort study designed to examine the prevalence, determinants and risk factors of cardiovascular disease.
Methods
Participants
WBV and its determinants were studied in 15,010 individuals of the Gutenberg Health Study. From April 2007 until April 2012, residents of the city of Mainz and the region Mainz/Bingen, Germany aged between 35 and 74 years have been invited to participate in this study. The selection of the participants from the city register offices is stratified based on gender (1:1 male/female), residence (urban versus rural) and age (equal number of participants across decades of age). Insufficient knowledge of the German language, unwillingness or physical or psychological inability to participate in the examinations are exclusion criteria. The project was approved by the local Ethics Committee and all participants provided written, informed consent. All data underwent quality control by a central data management unit and were checked for completeness and correctness by predefined procedures and plausibility controls.
A reference sample of 3223 apparently healthy subjects with a low risk for cardiovascular disease was identified from the 15,010-subject cohort. This subgroup included all subjects without (self-reported) medical history of myocardial infarction, chronic heart failure, or coronary artery disease and without observed cardiovascular risk factors (except for age; risk factors are defined below).
Definitions
Subjects who never smoked or were former (>6 months) smokers were classified as nonsmokers. Occasional and daily smokers were classified as smokers. Obesity was defined as a body mass index ⩾30 kg/m2. Diabetes mellitus was defined as blood glucose level of ⩾126 mg/dl at the baseline examination after an overnight fast of at least 8 hours, a blood glucose level of ⩾200 mg/dl in the baseline examination after a fasting period <8 hours or a previous physician’s diagnosis of diabetes. Dyslipidaemia was defined as a diagnosis of dyslipidaemia by a physician, or as a low-/high-density lipoprotein (LDL/HDL) ratio of >3.5. Antihypertensive medication, a mean sitting systolic blood pressure of ⩾140 mmHg or a mean diastolic blood pressure of ⩾90 mmHg were defined as hypertension. A positive family history of myocardial infarction was defined as history of myocardial infarction in female first-degree relatives <65 years old or in male first-degree relatives <60 years old. Blood pressure was measured three times in each subject, the values reported correspond to the average of the 2nd and 3rd standardized measurements after 8 and 11 minutes of rest. Medical history was collected through a computer-assisted personal interview performed by specifically trained and certified interviewers and, when available, from medical records.
Blood viscosity
WBV for two different levels of shear stress was calculated using previously validated formulae that take into account haematocrit and plasma proteins:

where Hct is haematocrit (%) and p is plasma protein concentration (g/dl). The two relationships provide an estimation of WBV measured in centipoise (cP, corresponding to the ratio of the shear rate of blood to the shear rate of water) at the level, respectively, of the microcirculation and of large conduit arteries. The above formulae were derived and previously validated through a range of haematocrit (32–53%) and plasma protein concentrations (5.4–9.5 g/dl) values [De Simone et al. 1990].
Statistical methods
WBV variables were plotted by gender and by 10-year age increments in the overall population and in the reference sample. The Jonkheere–Terpstra test for trend was used to compare viscosity (both low and high shear rate) between genders and across age strata. Spearman correlation coefficients adjusted for age and sex were calculated for the relationship between WBV (both low and high shear rate) and the following parameters, which are known to be associated with cardiovascular disease: body mass index (BMI), mean platelet volume (MPV), platelet counts, fibrinogen, glucose, HbA1c, creatinine, HDL, LDL, triglycerides and total cholesterol. Multiple linear regression models were used to investigate the association between the above cardiovascular risk factors and measures of WBV. The association between viscosity variables and the Euro Score (German Version) (calculated as described by Conroy et al. 2003) was assessed in a multiple linear regression model including age and gender. The relation of viscosity (high and low shear rate) with blood pressure (systolic, diastolic and mean) normalized by age and gender was studied in three different multiple linear regression analyses. Finally, the impact of a history of congestive heart failure, coronary artery disease, previous myocardial infarction, chronic obstructive lung disease and atrial fibrillation on WBV parameters was studied using multiple logistic regression analysis adjusted for gender, age, BMI, diabetes, hypertension, smoking, dyslipidaemia and family history of myocardial infarction. Analyses were performed separately in the whole population and in the reference sample of participants without risk factors or reported cardiovascular disease. Data are presented as mean ± standard deviation (SD), median with interquartile range or number (%) as appropriate. Skewed variables were logarithmically transformed to achieve near normal distribution. Given the multiplicity of endpoints tested, all analyses have to be considered exploratory. Complete case analysis was performed. For the analysis, R software, Version 2.10.1 (R Development Core Team, 2009, http://www.R-project.org) was used.
Results
The characteristics of the study population are presented in Table 1. Briefly, mean age was 55.0 (range 3–74) years, 49.5% were women. Men tended to have a higher prevalence of all risk factors for cardiovascular disease when stratified by age. Similarly, the age-adjusted prevalence of self-reported cardiovascular diseases, except for congestive heart failure, tended to be higher in males. Age was associated with increased prevalence of cardiovascular risk factors (except for smoking). The group of subjects without prevalent risk factors or cardiovascular disease was composed of 3223 individuals. While the distribution with respect to age and gender was uniform in the overall population, the reference sample had a skewed distribution, with a lower proportion of older subjects and a larger percentage of women.
Demographics and classical risk factors of the overall cohort and the reference sample without cardiovascular disease or risk factors for cardiovascular disease.

BMI: body mass index. Data are presented as mean ± standard deviation or median (Q1/Q3), or number (%) as appropriate.
The distribution of viscosity in the population
Age- and gender-adjusted values of WBV are presented in Tables 2 and 3. Women tended to have lower viscosity at both high and low shear rate (Table 2). Viscosity (both high and low shear rate) tended to decrease with age, a trend that was clearer in the group without risk factors for cardiovascular disease (Table 3). This trend was however not present in women (p = 0.28 and p = 0.86). Of the components of WBV, men had higher haematocrit and lower thrombocyte counts than women (43.7 ± 2.95 versus 40.3 ± 2.76 and 258 ± 62.3 versus 292 ± 71.6, respectively). Total proteins did not differ between genders. Haematocrit did not change with age; thrombocyte counts and total proteins decreased with increasing age (data not shown). After adjustment for age and gender, viscosity measures showed a moderate (Spearman correlation coefficient >0.1) positive association with thrombocyte counts, fibrinogen, LDL, total cholesterol and triglycerides. The correlation was weaker with HDL, glucose, HbA1c, creatinine and MPV. Pearson correlation coefficients are presented in Table 4.
Whole blood viscosity (WBV) in the overall cohort and the reference sample.

IQR, interquartile range; SD, standard deviation.
Distribution of whole blood viscosity (WBV) across decades of age.
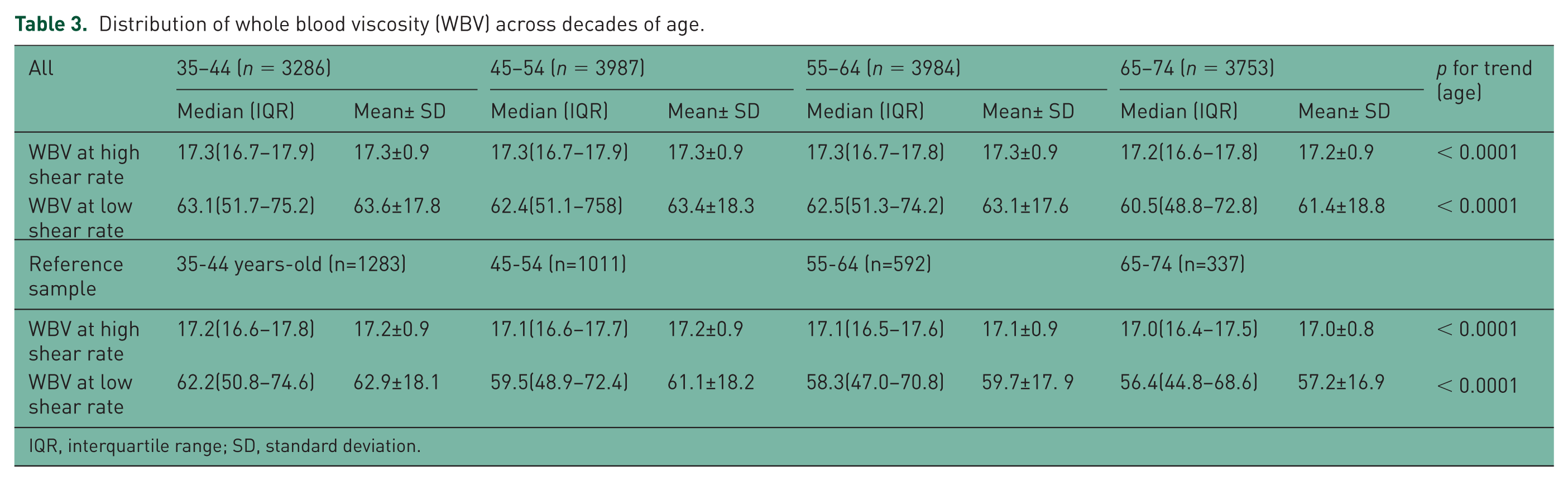
IQR, interquartile range; SD, standard deviation.
Partial correlations of whole blood viscosity (WBV) measures adjusted for age and sex. Spearman’s correlation coefficients.

BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SD, standard deviation.
Association with cardiovascular risk factors
In the overall population, multiple linear regression analysis showed a negative relationship between both measures of WBV and female gender, BMI and smoking. History of hypertension and hyperlipidaemia were positively correlated with viscosity parameters, while diabetes and family history of myocardial infarction showed no relationship (Tables 5 and 6). Together, risk factors explained only 6.7% of the variability of the viscosity at high shear rate and 5.0% of the variability of the viscosity at low shear rate. A positive relationship was shown between haematocrit and dyslipidaemia, smoking and hypertension, and a negative one between diabetes and haematocrit (all p < 0.0001). Collectively, risk factors explained as much as 28% of the variability in this parameter. In contrast, risk factors explained less of the variability in thrombocyte counts (7.8%). Finally, total protein levels showed a relationship with all risk factors for cardiovascular disease, which explained 3.4% of the variability in this parameter. A model including the Euro Score (German Version), age and gender explained 5.4% and 3.4%, respectively, of the variability in WBV at high and low shear rate.
Correlations of whole blood viscosity at high shear.

BMI, body mass index; CI, confidence interval.
Correlations of whole blood viscosity at low shear.

BMI, body mass index; CI, confidence interval.
The relationship between arterial blood pressure and viscosity
In both the overall and the reference populations, multiple linear regression analysis showed a linear positive association between WBV variables and systolic, diastolic and mean blood pressure (Table 7, Figure 1(a)–(f)). The statistical models including viscosity (either low or high shear rate), age and gender explained between 4% and 18% of the variability in blood pressure.
Multiple linear regression model describing the relationship between WBV and blood pressure. Data are presented as estimate and lower/upper 95% confidence interval.

CI, confidence interval; DBP, systolic and diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure; WBV, whole blood viscosity

The relationship between different measures of arterial blood pressure and whole blood viscosity (WBV). For all parameters considered, there was a linear positive association (high shear, upper panels; low shear, lower panels).
The relationship with cardiovascular diseases
Multiple logistic regressions adjusted for gender, age, BMI, diabetes, hypertension, smoking, dyslipidaemia, family history of myocardial infarction showed a very mild negative association between the diagnosis of congestive heart failure and measure of WBV at high shear rate: odds ratio 0.845, 95% confidence interval 0.716–0.998, p = 0.047; measures at low shear rate showed no association. Similar data were shown for coronary artery disease (viscosity at low shear rate: odds ratio 0.992, 95% CI 0.988–0.997, p=0.0013; high shear rate: odds ratio 0.838, 95% CI 0.761–0.923, p = 0.00034). Stroke, myocardial infarction and chronic obstructive lung disease were not associated with either measure of viscosity. Atrial fibrillation accordingly adjusted revealed a slight negative association to WBV at high shear rate (odds ratio 0.901, 95% CI 0.812–0.999, p = 0.047).
Discussion
The concept that an increased viscosity might be associated with worse tissue perfusion, hypertension and atherogenesis has long been postulated [Replogle et al. 1967]. While this hypothesis appears to be justified in the setting of the so-called primary hyperviscosity syndromes (e.g. polycytaemia vera, sickle cell disease), in which an extreme increase in WBV has been associated with microvascular plugging and impaired tissue perfusion, the pathophysiological significance of the increases in WBV previously observed in patients with coronary artery disease or congestive heart failure and no known blood disease is insufficiently understood. To date, despite a reported association between viscosity and cardiovascular morbidity and mortality [Becker, 1993; Danesh et al. 2000], this parameter is usually not assessed in clinical routine.
The distribution of viscosity in the population
We report data on the distribution of WBV, calculated using a validated formula from haematocrit and total protein levels, in a large, unselected, community-based cohort and in a reference sample of subjects with no cardiovascular risk factors and no known cardiovascular disease. The present data may help identify reference values of WBV and its determinants across genders and decades of age. Women tended to have lower viscosity both in the overall population and in the subgroup of subjects without risk factors for cardiovascular disease. Also, viscosity progressively declined with increasing age, and showed an association with most cardiovascular risk factors, except for diabetes and a family history of myocardial infarction. Although statistically significant given the size of the study, however, it needs to be acknowledged that these differences between genders and among decades of age were very small compared with the interindividual variability.
Viscosity as a marker or predictor of cardiovascular disease
The existence of an association between WBV and its major determinants (haematocrit, plasma viscosity and fibrinogen) with an increased cardiovascular risk has been reported. In the PIVUS (Prospective investigation of the Vasculature in Uppsala Seniors) study [Sandhagen and Lind, 2012], WBV was positively related to the Framingham Risk Score in a population of 1016 subjects aged 70. In the WOSCOPS study (West of Scotland COronary Prevention Study, enrolling 6595 hypercholesterolaemic men aged 45–64 years with no prior myocardial infarction), plasma and WBV were associated with an increased prevalence of cardiovascular risk factors and with coronary and peripheral atherosclerosis [Lowe et al. 2000]. This association remained significant in a multivariate analysis including baseline coronary artery disease and risk factors. De Simone and colleagues developed and validated the formulae used in the present paper, and showed a positive relationship between WBV and male sex, obesity, dietary Na+ intake, and increasing age, triglycerides, obesity, and cholesterol levels [De Simone et al. 1990]. Finally, in the MONICA (MONItoring CArdiovascular disease) survey an association was shown between WBV and mortality; however, this association was lost after adjustment for major cardiovascular risk factors [Woodward et al. 1999].
The present database is the largest available to date reporting data on the relationship between WBV, cardiovascular risk factors, and prevalent cardiovascular disease. In our dataset, parameters of viscosity showed a negative correlation with age, gender, BMI and smoking. In contrast, history of hypertension and hyperlipidaemia were positively correlated with viscosity parameters. Importantly, these associations were at best mild, and the risk factors represented a minor component of the variability in viscosity. The correlation with parameters of renal function, glucose homeostasis, and plasma lipids was also weak. WBV was negatively associated with the presence of congestive heart failure or coronary artery disease, but this relationship was also very weak. Finally, the association with the Euro Score (German Version) was also weak. The present data appear thus to suggest that, at a population level, viscosity is not associated cardiovascular risk factors and cardiovascular disease.
The relationship between viscosity and blood pressure
The Hagen–Poiseuille’s law stipulates that peripheral vascular resistances (and therefore blood pressure) are directly proportional to WBV. While this is valid for a system of rigid tubes, however, a number of considerations complicate this relationship in vivo [Jung, 2010]. In vivo, increases in WBV produce two opposite effects: a direct increase in haemodynamic hindrance, and an indirect decrease in vascular resistances mediated by endothelium-mediated, shear rate-dependent, vasodilation. The perfusion with high-viscosity plasma expanders is associated with increased perfusion, and increases in WBV are associated with lowered mean arterial blood pressure, reduced peripheral resistances and increased cardiac output [Martini et al. 2005; Tsai et al. 2005]. In line with this evidence, we and others recently proposed that the Poiseuille’s law should be reinterpreted in the context of the complex nature of cardiovascular homeostasis [Forconi and Gori, 2009].
In line with the complexity of this relationship, data in the literature are controversial. In the MONICA survey, blood pressure was positively associated with plasma viscosity [Koenig et al. 1991]. In the paper by Smith and colleagues, WBV, haematocrit and plasma viscosity positively correlated with blood pressure independently of age, BMI and smoking status [Smith et al. 1992]. In the paper by Fossum and colleagues, WBV correlated with systolic blood pressure and with lipid parameters [Fossum et al. 1997], while in the paper by De Simone and colleagues WBV correlated positively with systolic, mean and diastolic blood pressure [De Simone et al. 1990]. In contrast, systolic blood pressure was negatively related to WBV in Indian Americans in the Strong Heart Study even after adjustment for gender, age, smoking status, presence of obesity, diabetes, and plasma creatinine. No relation was found in this paper between WBV and diastolic blood pressure [De Simone et al. 2005]. Finally, in the paper by Irace and colleagues in 103 healthy volunteers, no association was shown between WBV and systolic blood pressure, while a positive relationship was found with diastolic blood pressure [Irace et al. 2012].
In the present database WBV was linearly and positively associated with systolic, diastolic and mean blood pressure, and this relationship was not changed after correction for age and gender. While this evidence cannot absolutely be used to propose WBV as a surrogate measure of blood pressure, it appears to suggest that the vascular hindrance determined by viscosity, and the resulting increase in peripheral vascular resistances, prevails over the effects of WBV on endothelium-dependent vasodilation. Whatever its’ meaning, the association between blood pressure and viscosity was however mild, and the statistical models including age, gender and WBV explained only between 4% and 18% of the variability in blood pressure. Notably, blood pressure increased with viscosity at all levels of viscosity in both subjects with cardiovascular risk factors or prevalent cardiovascular disease as well as in the reference group.
Limitations
An important limitation of the study is the absence of a direct measurement of WBV. It needs to be acknowledged the formula applied here provides only an indirect quantification of viscosity, even though it has been validated in large studies and has been shown to provide a valid alternative in settings where logistical considerations complicate the direct measurement of viscosity [Hoieggen et al. 1998; De Simone et al. 1990; Moan et al. 1994]. Among others, one important limitation of the formulae employed here is that they do not take into account blood cell aggregability and deformability.
We only measured the parameters under study once in every individual, which obviously does allow taking into account circadian rhythms and seasonal variability.
Importantly, we recognize that causality cannot be inferred from association. In the present paper, compatible with previous reports, a positive relationship was shown between WBV and arterial blood pressure. Whether increased viscosity is the cause or the effect of increased blood pressure cannot however be determined. Blood pressure increased with viscosity at all levels of viscosity, suggesting that the vascular hindrance determined by viscosity prevails over endothelium-dependent vasodilation. Neither the negative relationship observed by De Simone and colleagues in healthy volunteers [De Simone et al. 2005] nor the parabolic relationship observed by Martini and colleagues in a murine experimental setting were observed here [Martini et al. 2005]. Notably, the cross-sectional nature of this large-scale study does not allow investigating the causality relationship between the observed variability in viscosity and the observed variability in blood pressure and it allows no conclusions on the acute effect of experimental increases in hematocrit (and therefore viscosity). As well, we did not study the effect of drugs on viscosity. Finally, the large majority of the population enrolled in the Gutenberg Health Study is Caucasian of European ancestry. No conclusion can be drawn on the reported associations in other ethnic groups.
Although the p values have to be interpreted carefully given the size of the population under study, our study is the largest to date reporting the association of WBV with cardiovascular parameters in a large, well-characterized population based cohort and in a subset of individuals without cardiovascular risk factors. The present data provide age- and gender-specific values for WBV and further information on the relationship between viscosity and blood pressure.
WBV remains a simple parameter with complex implications. Further studies are necessary to investigate the implications of changes in this parameter on endothelial function, markers of vascular inflammation, development of carotid and coronary atherosclerosis, and mortality.
Footnotes
Conflict of interest statement
The authors have received research funding and speaker’s honoraria from several companies and institutions including: Federal Institute for Occupational Safety and Health (BAuA): Initiative ‘Health Economy’, Ministry of Health and Ministry of Economics, Rhineland-Palatinate; Federal Ministry of Education and Research; Federal Ministry of Health, Rhineland-Palatinate (MSAGD); Mainz Heart Foundation; DFG (no. WI 3881/2-1); EU (grant agreement nos 278913 and 278397), none in conflict with the content of this manuscript.
Funding
The Gutenberg Health Study is funded through the government of Rhineland-Palatinate (‘Stiftung Rheinland Pfalz für Innovation’, contract number AZ 961-386261/733), the research programs ‘Wissen schafft Zukunft’ and ‘Center for Translational Vascular Biology (CTVB)’ of the Johannes Gutenberg-University of Mainz and its contract with Boehringer Ingelheim and PHILIPS Medical Systems, including an unrestricted grant for the Gutenberg Health Study. PSW and TG are partially funded by the Federal Ministry of Education and Research (grant number BMBF 01EO1003).