
Abstract
Objectives:
The Middle East has a high prevalence of noncommunicable chronic diseases. The objective of this article was to quantify the research activity in cardiovascular disease (CVD) in the Middle East over the last 10 years.
Methods:
A Medline search was conducted using medical subject headings and author affiliation to retrieve research articles published from the Middle East between 2003 and 2012 (inclusive).
Results:
Middle Eastern countries produced only 3% of the total number of CVD research articles in the world. However, the overall trend showed an increase in the number of articles over the years, mainly from Turkey and Iran. Within this region, the ratio of CVD to non-CVD publications was highest in Qatar (0.23). Lebanon ranked first in the number of CVD publications per million persons (PMP) averaging 194.2 publications PMP and Turkey ranked highest in the number of CVD publications per US$1000 gross domestic product (GDP) per capita averaging 954 CVD publications per US$1000 GDP per capita.
Conclusions:
Although there has been a drive towards greater publication of CVD papers in the last decade, research activity in the Middle East still lags behinds developed countries. Greater productivity is anticipated to emerge to accompany the recent significant investment in research in Gulf countries.
Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide. Globally, it is estimated that 17.3 million people died from CVD in 2008 constituting 30% of all causes of mortality and the number of cardiovascular deaths is expected to increase to 23.3 million by 2030 [Myers and Mendis, 2014]. Major drivers for increasing cardiovascular deaths include smoking, hypertension, diabetes mellitus (DM) and obesity [Beaglehole et al. 2011].
In the Middle East, the continued increase in CVD burden is partially driven by accelerated epidemiological transition secondary to lifestyle change and urbanization [Akala and El-Saharty, 2006]. In this particular area of the world, patients with CVD are often younger in age, have a higher prevalence of risk factors, and more CVD severe complications [Akala and El-Saharty, 2006; Almahmeed et al. 2012; Gehani et al. 2014], notably DM. It is already known that patients with DM develop more cardiovascular complications, which consequently lead to a higher mortality rate than individuals without DM [Abi Khalil et al. 2012]. In a case-control study in a coronary care unit in Qatar, Mushlin and colleagues showed that the odds ratios associated with DM in patients admitted with acute myocardial infarction was estimated to be 4.01 (95% confidence intervals [CIs] 2.51–6.42) compared with 1.75 (95% CIs 0.94–3.29) for North America [Mushlin et al. 2012].
The Institute for Health Metrics and Evaluation in 2012 reported a significant increase in ischemic heart disease, DM, and stroke-related mortality between 1990 and 2010 all over the world, and the Middle East was not an exception [Lozano et al. 2012]. This was also confirmed by Mokdad and colleagues who recently showed that 7 out of the 14 top causes of death in the Arab world in 2010 were due to CVD, whereas 20 years ago infectious-related pathologies and other diseases were more prevalent [Mokdad et al. 2014]. Given the high burden of CVD in the Middle East, there is a major need for further research. In this study, we provide the first comparative bibliometric analysis of CVD research publications in the Middle East compared with the USA and UK.
Methods
We conducted a Medline search using the database website PubMed (available from the National Institutes of Health, Bethesda, MA, USA) during the month of August 2013. We employed the medical subject headings service (MeSH), a comprehensive controlled medical vocabulary that provides indexing for articles within MEDLINE. To search for CVD publications, we used the following MeSH terms:
For the purposes of this study, PubMed filters were set to include all of the following types of articles: case reports; clinical conference; clinical trial; clinical trial, phase I; clinical trial, phase II; clinical trial, phase III; comparative study; controlled clinical trial; journal article; letter; meta-analysis; multicenter study; randomized controlled trial; review; systematic reviews; validation studies.
To locate the primary institution of publication, we employed the search criteria of the first author affiliation country. The strategy included the name of the country (or modified name in case of disambiguation/different names for countries as noted in Table 1). For the purposes of this study, the Middle East includes the following 14 countries: Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi Arabia, Syrian Arab Republic, Turkey, United Arab Emirates, and Yemen.
Population estimates and gross domestic product per capita.

Our search included combining the strategies using the Boolean parameters (AND, OR). For example, to look for CVD publications from Iraq, we used the following search keywords: ‘cardiovascular diseases’ [mesh] AND ‘Iraq’ [ad]. We used 2012 as the end year as articles need processing time to be indexed in Medline after being published.
After applying the filters above, we conducted a search on CVD publications during the month of August 2013 for each country. For correction of the number of publications per gross domestic product (GDP), we divided the number of publications retrieved by US$1000 GDP per capita [World Bank, 2012a]. We also divided the number of publications by population size [Heston et al. 2012].
Results
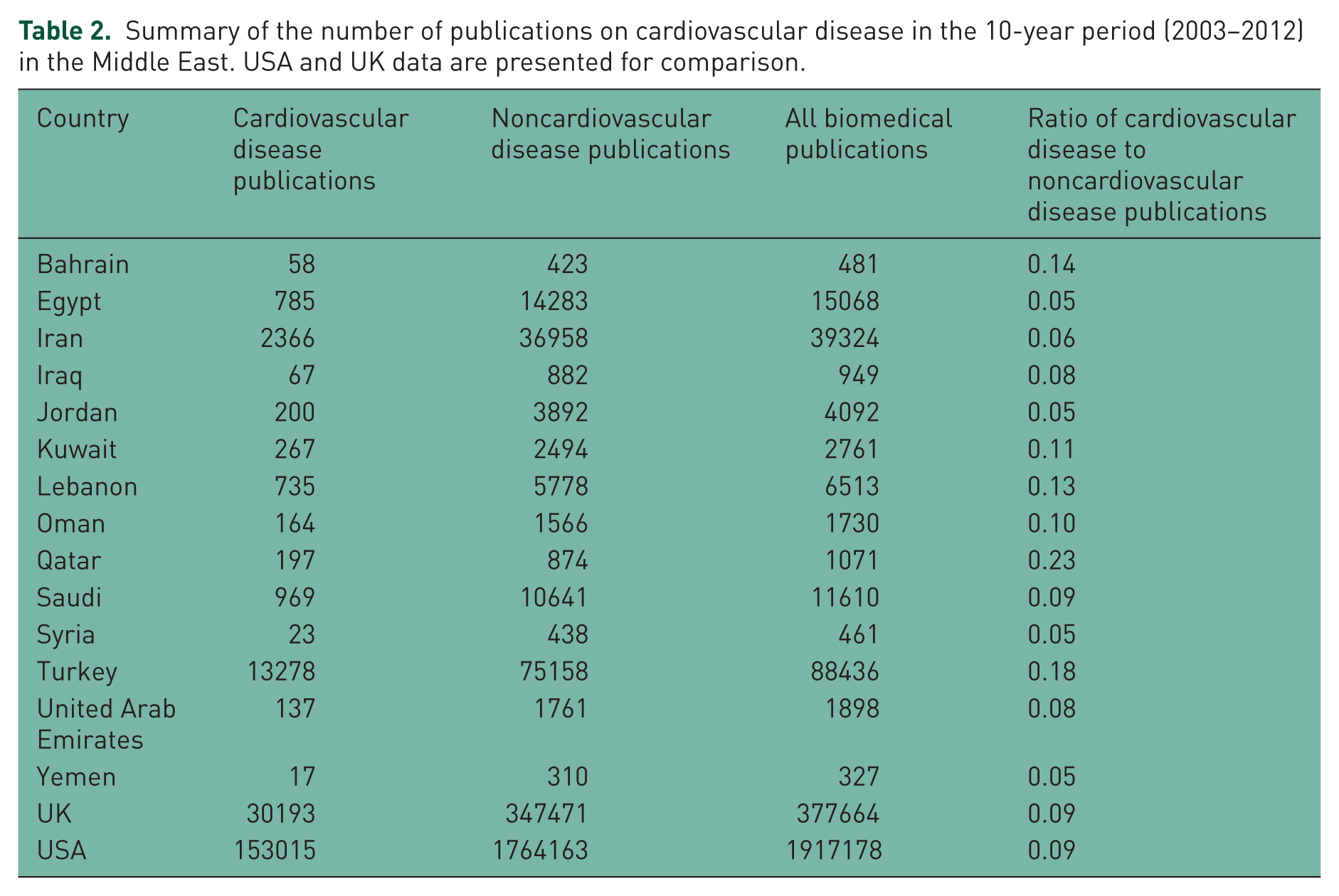
Data for GDP per capita and population size are shown in Table 1. Over the 10-year study period, there were a total of 641,704 CVD publications registered in PubMed. Of those results, 19,263 (3.0 %) CVD publications were from the Middle East (Table 2). There was an overall upward trend for the number of CVD publications in all Middle Eastern countries, mainly from Turkey and Iran (Figure 1). The ratio of CVD to non-CVD publications over the 10-year period ranged between 0.05 (Egypt, Jordan, Syria, and Yemen) to 0.23 (Qatar) compared with 0.09 (USA and UK). Figure 2 provides visual representation of these percentages by country.
Summary of the number of publications on cardiovascular disease in the 10-year period (2003–2012) in the Middle East. USA and UK data are presented for comparison.

Trend of cardiovascular disease (CVD) publications (2003–2012) by country.

Ratio of cardiovascular disease (CVD) publications to publications on non-CVD disease by country.
From the Middle Eastern countries, Turkey had the highest number of CVD publications with 13,278 reported, whereas Yemen had the smallest number with only 17 (Table 2). To avoid the bias of a ‘population mass effect’ on the number of publications, we corrected our results for population size (Figure 3). Lebanon ranked first in the region at 194.2 publications per million persons (PMP), but Yemen still had the lowest number of CVD publications at 0.73 publications PMP. For comparison, USA had 494.6 publications PMP and UK had 486.8 PMP.
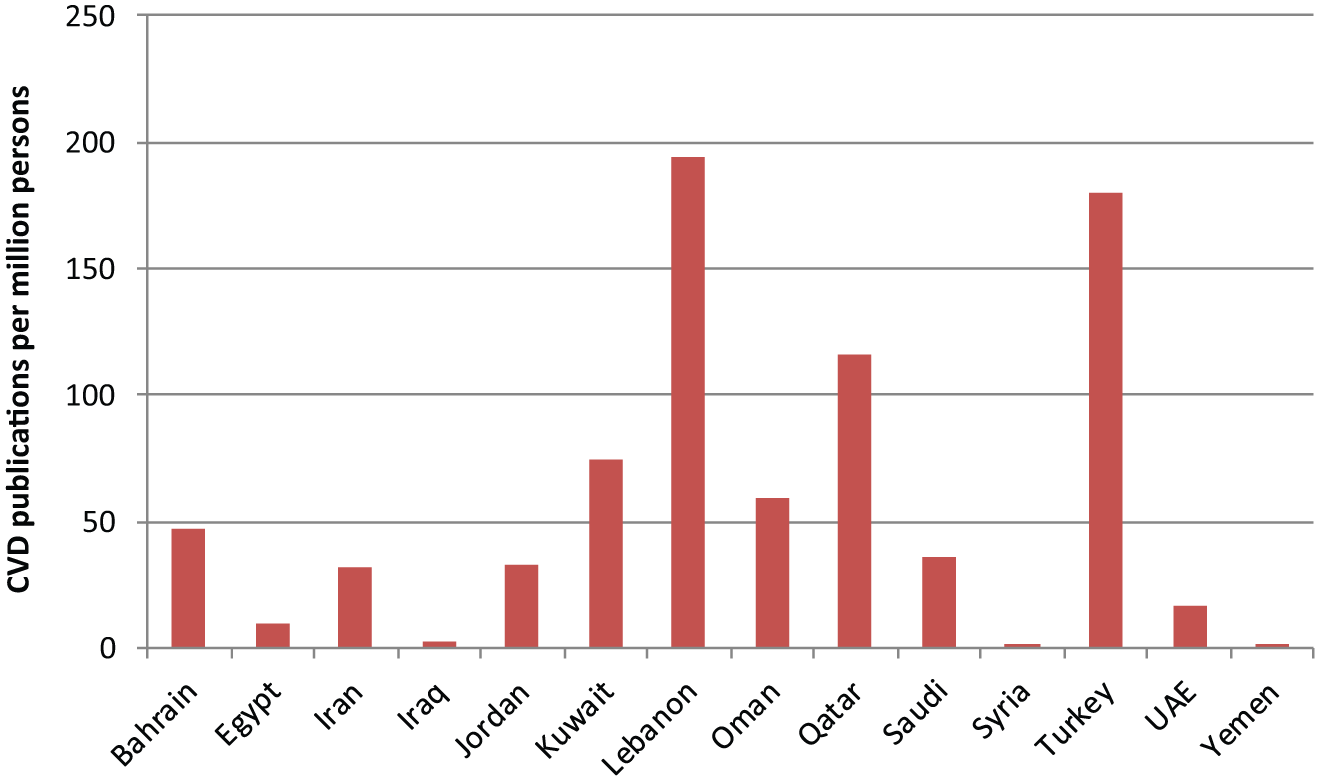
Numbers of cardiovascular disease (CVD) publications per million persons by country.
When corrected for GDP per capita (Figure 4), Bahrain had the lowest number of CVD publications at 2.5 publications per US$1000 GDP per capita, whereas Turkey ranked first, averaging 954.4 CVD publications per US$1000 GDP per capita (Figure 4). This compares with 3409.7 CVD publications per US$1000 GDP per capita for USA and 878.7 CVD publications per US$1000 GDP per capita for UK.

Numbers of cardiovascular disease (CVD) publications per US$1000 of gross domestic product (GDP) per capita by country.
Discussion
Our results show that Middle Eastern countries produced only 3.0 % of the total number of CVD research articles as registered in PubMed. The overall trend showed an increase in the number of articles from the Middle East over the last 10 years. Our results are in line with a recent global cardiovascular bibliometric analysis that showed a 36% increase in CVD publications during the last 10 years [Huffman et al. 2013].
The low research productivity in Middle Eastern countries might be attributed to multiple factors. The medical schools and hospitals in the Arab world are patient-care oriented, with a fledgling clinical research culture. Only in recent times has clinical research been emphasized. In addition, there is a general lack of research infrastructure within hospitals and academic centers in some of these countries. There is also a general lack of funding for biomedical research, except in some Gulf Cooperation Council (GCC) countries, and most published studies are independent retrospective studies. Another explanation for the low productivity could be the absence of grey literature in our bibliometric analysis as research does not always progress to the publication of manuscripts. Political instability contributes to the absence of biomedical research funding and opportunities in some Middle Eastern countries [Kahan et al. 1996]. The recognition of these barriers has resulted in countries such as Qatar developing an academic health science program accompanied by a restructuring of healthcare to embed research activity. Furthermore, collaborations with established institutions have supported a rapid expansion in research activity. Other initiatives include research training for clinicians and the establishment of medical journals [Chouchane et al. 2011].
GCC countries rank among the highest income countries, but are only recently investing in medical research and establishing successful research institutions. Qatar and Saudi Arabia are among the first to allocate large funds for biomedical research activity and attract international researchers [Giles, 2006]. Qatar, for example, has allocated 2.8% of its annual domestic income for research support, compared with 2.7% in USA [World Bank, 2012b]. Over the past 10 years, Qatar has produced many CVD papers and has ranked first in terms of publications PMP in GCC countries, but ranks lower when assessed per GDP. This might be attributed to a lag between initiation of research institutions and research activity and publication; therefore, more time is required to reflect the number of research publications. Initiatives, such as the academic health sciences program in Qatar [Hillhouse et al. 2012], are likely to expedite a greater number and better quality of CVD papers. Saudi Arabia produced a notable number of research papers on CVD, and this is probably due to the longer establishment of research activity in the field as it started its research programs earlier. The larger population, appropriate fund allocation towards scholarships, and citizens traveling abroad to attain their education could also be contributing factors. Turkey and Iran have had their research and academic institutions for a significant time and this is reflected in the high number of CVD publications. Countries with lower income (i.e. Syria, Yemen, Iraq, and Jordan) still have low production of CVD publications, probably due to their previous low gross income, which limits research investment.
Research activity in the Middle East has been evaluated in various biomedical specialties. Most reports concluded that productivity is very low and insufficient compared with surrounding and western countries [El-Azami-El-Idrissi et al. 2013]. Benamer and Bakoush reported earlier that Arabic Middle Eastern countries produced less than other non-Arabic Middle Eastern countries [Benamer and Bakoush, 2009], a finding we are able to confirm when looking at the data from Iran and Turkey. The Middle East produced only 0.75% of global DM publications between 1996 and 2012 [Sweileh et al. 2014a], and 1% of the global obesity research output at all times [Sweileh et al. 2014b]. The research activity related to priority interventions for noncommunicable disease prevention in low- and middle-income countries showed that the Middle East published fewer research articles than the Latin America and Caribbean region, the East Asia and Pacific region, or Europe and Central Asia [Jones and Geneau, 2012]. To our knowledge, no study has analyzed CVD publications in this region despite the increased burden of CVD. Our data are close to those published by Jahangir and colleagues who reported that Latin America published 4% of CVD publications compared with 26% from the USA with a slow upward trend over time [Jahangir et al. 2011].
There are some limitations related to our study. We recognize that bibliometric analysis is not a perfect representation of research productivity. This has been demonstrated in different areas of medicine, particularly in cardiovascular medicine [McAlister et al. 2011]. Bibliometric analysis cannot represent the impact of a scientific work or its quality using current standardized methods such as impact factors of the journal, article’s citations, or h-index.
Research in CVD, especially clinical research, requires multicenter participation, and thus, requires organized research groups with coordination between the different centers. With the recent cardiovascular research initiatives, more publications are expected to appear, especially from the GCC countries where local and international research institutes have recently increased their collaborative research activity, aiming to develop cutting-edge translational medicine research [Chouchane et al. 2011]. This would also enhance patient care as it has been shown that participating in clinical research is linked to improvement of clinical outcomes [Krzyzanowska et al. 2011]. A correlation has also been shown between disease epidemiology and volume of research activity [Somogyi and Schubert, 2005].
Conclusion
Currently, most Middle Eastern countries are lagging behind in biomedical and cardiovascular research activity. Given the high burden of CVD in the Middle East, and given the different genetic backgrounds and composition of these populations, more high-quality research is essential. We expect that several Gulf countries will see significant research productivity in the next decade. This will, in turn, improve healthcare outcomes in very high-risk populations.
Footnotes
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.