
Abstract
We describe a case of a giant left anterior descending coronary artery pseudoaneurysm presenting with acute coronary syndrome and projecting as a paracardiac mass on chest X-ray.
A 35-year-old gentleman with no past medical history of significance and no risk factors for coronary artery disease presented to the emergency room complaining of a 1-month history of recurrent episodes of anginal chest pain associated with shortness of breath. Cardiac examination showed a displaced apical impulse, and an S3 gallop. Chest X-ray (CXR) (Figure 1) showed an abnormal contour in the cardiomediastinal silhouette with an outward bounded bulge of the left heart border, measuring approximately 6 cm. Electrocardiogram (Figure 2) revealed coved ST-segment and biphasic T waves in the anterior chest leads that were dynamic, suggestive of anteroseptal ischemia. The patient had a mild troponin leak that peaked at 0.28 ng/ml with normal creatine phosphokinase (CPK) and creatine kinase MB (CKMB) enzymes. Echocardiography showed a dilated left ventricle with an ejection fraction of 35% and global hypokinesia. Coronary angiography revealed a large pseudoaneurysm approximately 7 cm × 7 cm of the left anterior descending (LAD) coronary artery with mass effect on the mid LAD (Figure 3) and an intra-aneurysm blood clot. Surgical excision of the pseudoaneurysm was performed with coronary artery bypass grafting (CABG) of saphenous vein graft (SVG) to the distal LAD and suture occlusion of the proximal LAD at its entry point into the pseudoaneurysm. Histopathology confirmed the diagnosis of LAD pseudoaneurysm with multiple blood clot fragments and showed no pathological evidence of vasculitis. On further interrogation, the patient had a prior history of chest trauma 10 years earlier and this was thought to be the cause of the pseudoaneurysm. He was discharged symptom free from the hospital.

Chest X-ray showing an abnormal contour in the cardiomediastinal silhouette with an outward bounded bulge of the left heart border, measuring approximately 6 cm.

Electrocardiogram performed during chest pain showing coved ST-segment and biphasic T waves in the anterior chest leads.
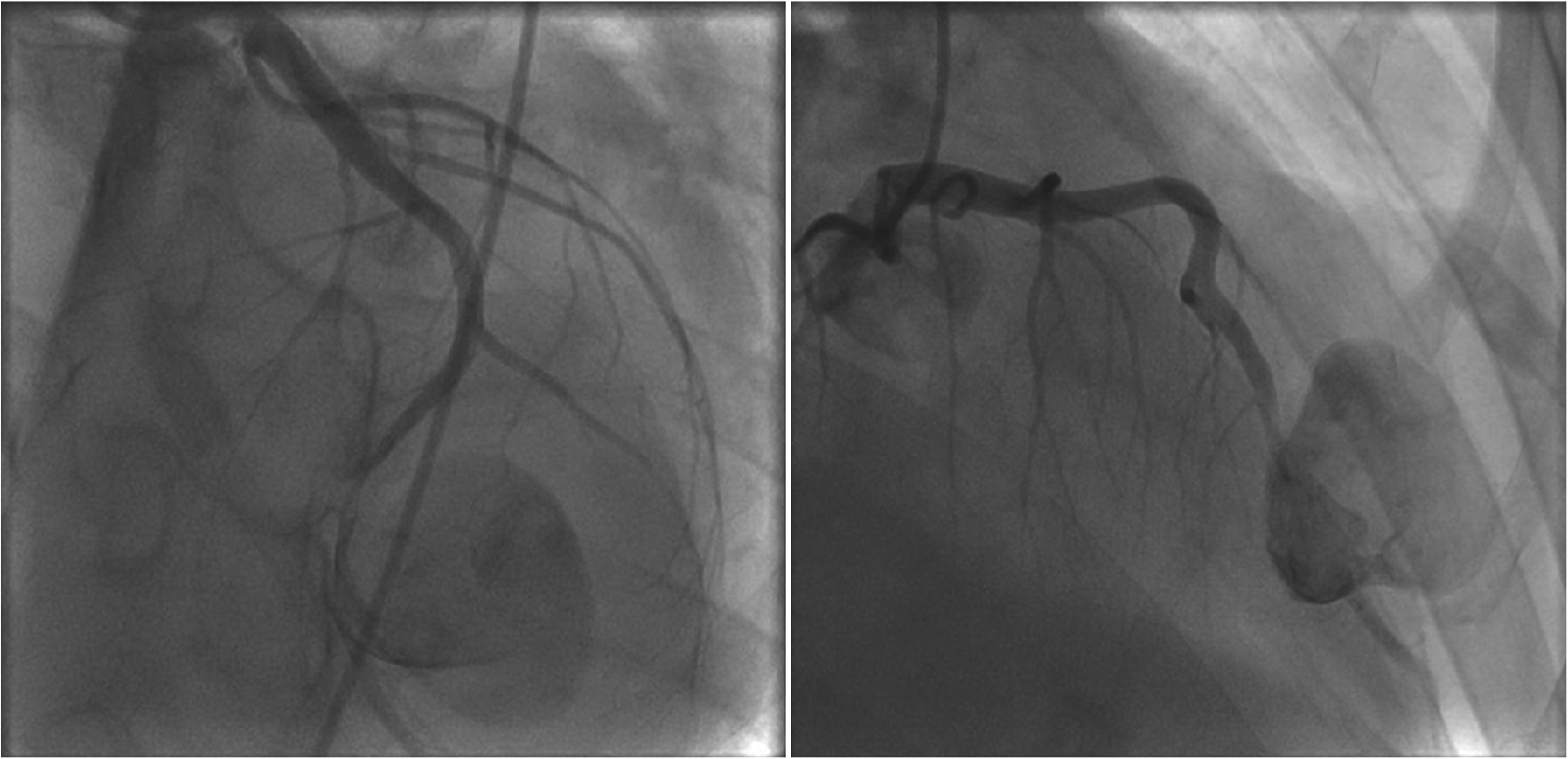
Left coronary angiography showing a large pseudoaneurysm (approximately 7 cm × 7 cm) of the left anterior descending (LAD) coronary artery with mass effect on the mid LAD.
Coronary artery aneurysms (CAAs) usually develop due to atherosclerotic disease [Keyser et al. 2012; Daoud et al. 1963], congenital [Li et al. 2005], Kawasaki disease [Kato et al. 1975], connective tissue disorders, following percutaneous coronary intervention [Hill et al. 1983] or trauma. Giant CAAs are rare, with an estimated prevalence of 0.02% in a large surgical series [Li et al. 2005]. CAA can be silent, discovered accidentally during cardiac imaging, or can present with myocardial ischemia (either from coronary compression or embolism from thrombi formed inside aneurysm), fistula to cardiac cavities, cardiac tamponade, rupture or sudden death. Giant CAA can be associated with fatal complications and hence the general consensus is aneurysm resection and concomitant CABG surgery [Li et al. 2005; Holinski et al. 2009; Lazar et al. 2013]. In the presented case, the absence of evidence of atherosclerosis or other clear explanation for the pseudoaneurysm favors that prior chest trauma might have been responsible. The report highlights that CAA should be in the differential diagnoses of a paracardiac mass found on the CXR.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors have no conflicts of interest to declare.