
Abstract
Background:
Knowledge of hemodynamic factors accounting for the development of hypertension should help to tailor therapeutic approaches and improve blood pressure control. Few data exist regarding sex differences of hemodynamic factors contributing to hypertension progression among patients with untreated nondiabetic stage I and II prehypertension (PreHyp) as defined by the Joint National Committee-7 guidelines (JNC-7).
Methods:
We utilized noninvasive impedance cardiography, applanation tonometry and plasma measures of angiotensin II, angiotensin (1–7), serum aldosterone, high-sensitivity C-reactive protein (hs-CRP) and cytokine biomarkers of inflammation to characterize the hemodynamic and hormonal profile of 100 patients with untreated hypertension (39 women).
Results:
Despite there being no differences between women and men in terms of office blood pressure, heart rate and body mass index, men demonstrated lower values of pulse pressure, systemic vascular resistance, brachial artery pulse wave velocity and augmentation index. In each of the three hypertension categories, the increased blood pressure in men was associated with significant augmentations in stroke volume and cardiac output compared with women. Sex-related hemodynamic differences were associated in women with higher plasma levels of leptin, hs-CRP, plasma angiotensin II and serum aldosterone, and no differences in the serum concentrations of cytokinins. In women but not men, hs-CRP correlated with plasma concentrations of transforming growth factor β1 (TGFβ1) and body weight; in addition, plasma TGFβ1 correlated with levels of serum vascular cell adhesion molecule 1.
Conclusion:
The impact of sex differences in the hemodynamic factors accounting for the elevation in arterial pressure in subjects with essential hypertension has been poorly characterized or this information is not available. We suggest that this gap in knowledge may adversely influence choices of drug treatment since our study shows for the first time significant differences in the hemodynamic and hormonal mechanisms accounting for the increased blood pressure in women compared to men.
Keywords
Introduction
Cardiovascular disease (CVD) in women is a major public health issue, ranking first among all disease categories in hospital discharges, and surpassing men in terms of the absolute number of deaths due to diseases of the heart and the blood vessels [Mosca et al. 2010, 2011, 2013]. Although 70% of deaths in women are attributable to modifiable risk factors such as hypertension, the question of whether antihypertensive therapy should take into consideration potential differences in mechanisms between sexes has not been answered. Women have lower blood pressure control rates [Abuful et al. 2005], they are less likely to be appropriately treated [Ferrario et al. 2013; Joyner et al. 2012; Lloyd-Jones et al. 2005a, 2005b] and data suggest that treatment efficacies differ between the two sexes [Turnbull et al. 2007, 2008a, 2008b]. In an investigation of the response rates to different drug regimens, Thoenes and colleagues found a higher use of thiazides and β blockers in women [Thoenes et al. 2010]. Another study reported a greater efficacy of aldosterone antagonists in reversing endothelial dysfunction in postmenopausal women [Rossi et al. 2011]. A post hoc analysis of the data obtained in the Losartan Intervention For Endpoint reduction in hypertension (LIFE) study showed less regression of electrocardiographic indices of left ventricular hypertrophy in women even after correction of cofactors such as treatment effects and blood pressure changes [Okin et al. 2008].
Consistent with our previous studies that underscored the importance of tailoring antihypertensive therapy based on the hemodynamic characteristics derived from noninvasive assessments [Abdelhammed et al. 2005; Ferrario et al. 2007; Ferrario and Smith, 2006; Smith et al. 2006a], we evaluated the characteristics of men and women with untreated hypertension in terms of the hemodynamic mechanism contributing the hypertension together with a direct assessment of renin angiotensin system components and inflammatory cytokines previously reported to be biomarkers of vasoconstriction, salt retention and vascular inflammatory response. In accomplishing these objectives we agree with Safar and Smulyan, who proposed that an understanding of the diverse mechanisms participating in the blood pressure elevation could ‘reduce the therapeutic trial and error now necessary for the selection of an individual patient’s antihypertensive regimen’ [Safar and Smulyan, 2004].
Methods
The study included 100 subjects without diabetes who had essential hypertension and were clinically free from overt atherosclerosis, other cardiovascular renal disease and other major diseases. General chemistries, urinary sodium, noninvasive hemodynamic measurements and plasma/serum biomarkers were obtained in subjects fasting for 24 h. Basic demographic data and the effects of 12-month treatment with either an atenolol-based or an olmesartan-based therapy on vascular hypertrophy have been published [Smith et al. 2008]. Other than the office blood pressure, the previous publication did not include any of the data reported here.
Patient eligibility was based on the absence of the following exclusion criteria: seated diastolic blood pressure less than 90 mmHg or greater than 109 mmHg, or systolic pressure less than 140 mmHg or greater than 179 mmHg; a secondary cause of hypertension; diabetes mellitus; a history of myocardial infarction, transient ischemic attack, or cerebrovascular accident within the prior 3 months; congestive heart failure, ejection fraction less than 50%, or other significant heart disease; active autoimmune disease; a body mass index (BMI) of at least 35 kg/m2; malignancy; azotemia (serum creatinine > 3.0 mg/dl); serum potassium less than 3.3 mEq/liter; significant hematologic or hepatic test abnormality; alcohol or substance abuse; or known hypersensitivity to all blood pressure medications. The study was approved by the Institutional Review Board of Wake Forest University School of Medicine as a component of the trial that investigated the effects of an atenolol-based therapy versus an olmesartan-based therapy on blood pressure control and peripheral vascular remodeling [Smith et al. 2006a, 2006b]. All patients signed an informed consent.
Hemodynamic measures
Noninvasive hemodynamic measures were obtained using the BioZ impedance cardiography (ICG) hemodynamic Monitor (CardioDynamics, San Diego, CA, USA) by a technician after 5–10 min of rest in the supine position. As validated in a number of publications from our laboratory [Abdelhammed et al. 2005; Ferrario et al. 2007; Ferrario and Smith, 2006; Smith et al. 2006a], the device measures changes in impedance by injecting a high-frequency (60 kHz minimum), low-amplitude (4.0 mA root mean square maximum) alternating electrical current through the subject’s thorax between a pair of sensors placed on the neck and another pair placed on the mid-axillary line at the xiphoid process level. Changes in thoracic impedance as a function of time allow the noninvasive determination of stroke volume, cardiac output and thoracic fluid volume. Concurrent oscillometric measures of arterial pressure allow for the calculation of vascular resistance and the secondary determination of systemic vascular resistance index.
Brachial artery pulse wave velocity (baPWV) was obtained using an automatic waveform analyzer (VP-2000, Colin Medical Technology, Komaki, Japan) while the patient was lying in a supine position 5–10 min after occlusion cuffs were placed snugly around each arm and ankles. Brachial-tibial artery pressure waveforms were then recorded simultaneously. The central arterial pressure and the derived augmentation index were determined with the technique of applanation tonometry (SphymoCor Pulse Wave Analysis System, PVW Medical Pty Ltd, Sidney, Australia). We [Abdelhammed et al. 2005] and others [Asmar et al. 1995, 2001; Chemaly et al. 2002] have documented the inter- and intravariability indexes for these measures previously.
Biochemical assays
Laboratory measures were assessed at the completion of the washout period in the fasting state. The measures included determinations of plasma glucose, insulin, serum creatinine and electrolytes (sodium, potassium and bicarbonates). Plasma concentrations of angiotensin peptides [angiotensin II (Ang II) and angiotensin (1–7) [Ang (1–7)] were determined by radioimmunoassay (RIA) from venous blood collected in ethylenediaminetetraacetic acid (EDTA) tubes containing a cocktail of protease inhibitors including 0.44 mM 1, 20 ortho-phenanthrolene monohydrate (Sigma, St Louis, MO, USA), 0.12 mM pepstatin (Peninsula Labs, Belmont, CA, USA) and 1 mM Na p-hydroxymercuribenzoate (Sigma), as described by us elsewhere [Ferrario et al. 1998, 2002; Kohara et al. 1991]. Recoveries of radiolabeled angiotensin added to the sample and followed through the extraction were 92% (n = 23). The minimum detectable levels of the assays were 0.9 fmol (0.8 pg/tube). The intra-assay coefficient of variation is 12% for Ang II. RIA measures of serum aldosterone were determined from venous blood collected in antibody-coated tubes. The assay sensitivity was 1 ng/dl and the intra-assay precision was 5% coefficient of variation (CV) at a mean of 25 ng/dl; the CV of the interassay precision was 6.6% at a mean of 25 ng/dl.
Serum concentrations of the inflammatory markers: intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1), P selectin, high-sensitivity C-reactive protein (hs-CRP) and the cytokines transforming growth factor β1 (TGFβ1) and tumor necrosis factor α (TNFα) were measured by enzyme linked immunosorbent assay (ELISA) using reagents from R&D Systems (Minneapolis, MN, USA). The assay sensitivity for ICAM-1 is 0.35 ng/mL and the intra-assay precision is 7.8% CV at a mean of 125.6 ng/mL. Interassay precision is 10.2% CV at a mean of 254 ng/mL. The assay sensitivity for VCAM-1 is 2.0 ng/mL. Intra-assay precision (CV) is 10.7% at a mean of 212 ng/mL. Interassay precision is 9.5% CV at a mean of 1236.4 ng/mL. The assay sensitivity for P selectin is 0.5 ng/mL. Intra-assay precision is 5.0% CV at a mean of 20.2 ng/ml. Interassay precision is 9.9% CV at a mean of 94 ng/mL. The sensitivity of the ELISA TGFβ1 is 7 pg/mL. The intra-assay CV is 4.9% and the interassay CV is 7.7%. TNFα assay sensitivity is 3 pg/mL. The intra-assay CV is 5.2% and the interassay CV is 8.0%.
Statistical analysis
Unless noted otherwise, all data are expressed as mean ± 1 standard errors of the mean. Comparisons between sex groups were performed by analysis of variance and post hoc multiple comparisons were made by the unpaired Student’s t test with appropriate correction of the significance level for multiple comparisons. Statistical significance was set to a p value less than 0.05.
Results
The study population comprised 100 patients with untreated hypertension and without diabetes (39% women) age 53 ± 1 year. Grouped average office seating systolic and diastolic blood pressures were 147 ± 1 and 93 ± 1 mmHg respectively. No differences were observed in baseline office arterial pressure and heart rates between the sexes. While on average women had lower body weights than men, their BMI was not significantly different (Table 1). Women had lower serum creatinine values and higher plasma leptin concentrations compared with men (Table 1) while no sex differences were demonstrated in plasma glucose and insulin concentrations (Table 1).
Baseline values.
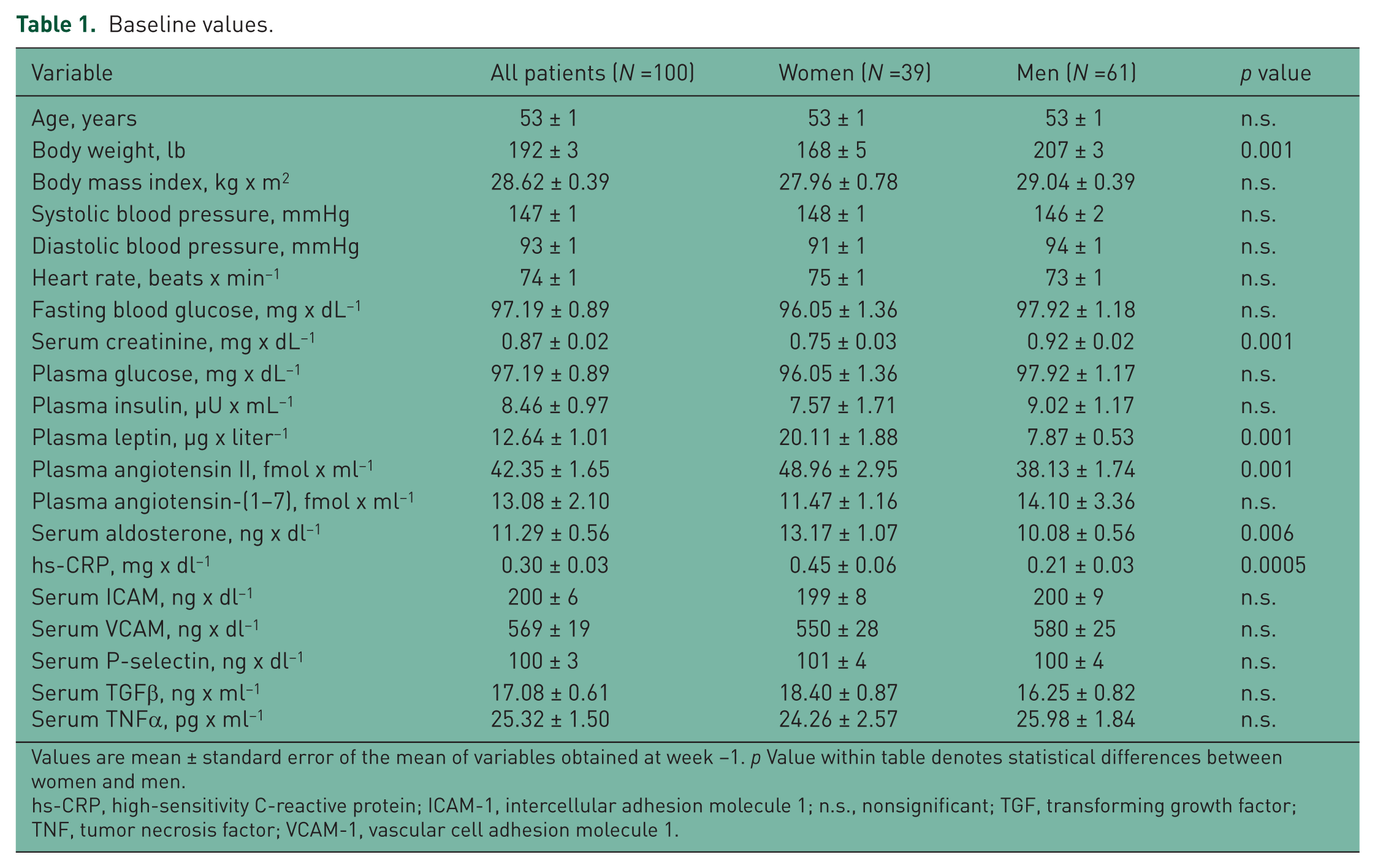
Values are mean ± standard error of the mean of variables obtained at week −1. p Value within table denotes statistical differences between women and men.
hs-CRP, high-sensitivity C-reactive protein; ICAM-1, intercellular adhesion molecule 1; n.s., nonsignificant; TGF, transforming growth factor; TNF, tumor necrosis factor; VCAM-1, vascular cell adhesion molecule 1.
Hemodynamic differences between women and men with untreated hypertension
Figure 1 illustrates the hemodynamic patterns found in the 61 men and 39 women with untreated hypertension at the time of noninvasive hemodynamic measures. Although mean arterial pressure and heart rate values were similar in both groups, men showed lower values of pulse pressure and systemic vascular resistance while their cardiac output and thoracic fluid content is higher compared with the women. Figure 2 shows that men with hypertension had lower values of baPWV and augmentation index (AG/PP) than women, which was associated with a higher Buckberg index (diastolic pressure–time index/systolic pressure–time index) [Saito and Kasuya, 2003; Sharma et al. 1999; Siebenhofer et al. 1999] (Figure 2). The higher pulse pressure measured in women (60 ± 14 mmHg) compared with men (51 ± 12, p < 0.0001) was correlated with age (r = 0.52, p < 0.05). Pulse pressure did not correlate with age in men.

Group average hemodynamic values determined in 39 women and 61 men with untreated hypertension. Values are mean ± standard error of the mean.

Brachial-ankle pulse wave velocity values in 39 women and 61 men with untreated hypertension. Values are mean ± standard error of the mean.
Because hemodynamic differences found in the two groups could be influenced by the magnitude of the blood pressure elevation, we proceeded to analyze the data according to the Joint National Committee guidelines (JNC-7) blood pressure categories (Figure 3). Six women and 15 men were defined as having prehypertension based on blood pressure average values of 130 ± 4/84 ± 3 mmHg and 131 ± 2/91 ± 2 mmHg respectively (p > 0.05) at the time of hemodynamic measures. Blood pressure in subjects with stage I hypertension (20 women and 35 men) was 149 ± 1/91 ± 2 mmHg and 149 ± 1/98 ± 2 mmHg respectively. An additional 14 women and 20 men fell into stage II hypertension with average blood pressure values of 173 ± 2/103 ± 3 mmHg and 172 ± 2/110 ± 2 mmHg respectively. Throughout the hypertension stages, sex differences in cardiac output pulse pressure, stroke volume, cardiac output, systemic vascular resistance and thoracic fluid volume are still present. When the data were broken down in terms of hypertension stages, women with stage I and II hypertension were heavier than those with prehypertension (78 ± 3 versus 65 ± 6 kg) and this was associated with increased pulse pressure (63 ± 2 versus 46 ± 4 mmHg) and higher systemic vascular resistance index (3390 ± 123 dynes x s2 x /cm-5 x m2 versus 2739 ± 227 dynes x s2 x /cm–5 x m2). There were no differences in either cardiac output or cardiac index among hypertension stages in women (Figure 3). Similarly, men with stage I and II hypertension differed from those with prehypertension in being heavier (94 ± 2 kg versus 90 ± 3 kg) and manifesting higher values for pulse pressure (55 ± 2 mmHg versus 40 ± 1 mmHg) and systemic vascular resistance index (3262 ± 112 dynes x s2 x cm–5 x m2 versus 2793 ± 98 dynes x s2 x cm–5 x m2). At all stages of blood pressure, men had higher stroke volumes and cardiac output, lower values of systemic vascular resistance, pulse pressure and increased thoracic fluid content (Figure 3). baPWV was higher in women with stage II hypertension while it was increased in men with either stage I or stage II hypertension (Figure 4). Men with hypertension had lower values of the augmentation index throughout all stages of hypertension compared with women (Figure 4).

Hemodynamic characteristics by sex and blood pressure stages between female (F-) and male (M-) subjects. Data are mean ± standard error for 21 subjects with prehypertension (PreHyp) (6 women and 15 men), 55 subjects with stage I hypertension (20 women and 35 men), and 28 subjects with stage II hypertension (14 women and 14 men). *p < 0.05 compared with subjects with PreHyp of the same sex; ◆ p < 0.05 compared with male subjects.

Data are mean ± standard error of brachial-ankle pulse wave velocity and augmentation index measurements in women and men with untreated hypertension by stages of high blood pressure. *p < 0.05 compared with subjects with prehypertension (PreHyp) of the same sex; ◆ p < 0.05 compared with male subjects.
Sex differences in biomarkers between women and men with hypertension
Women with hypertension had higher plasma concentrations of Ang II, serum aldosterone and hs-CRP compared with men with hypertension. Baseline values for serum ICAM-1, VCAM-1 and P selectin were similar in men and women (Table 1). In women, but not men, significant correlations were found between systolic blood pressure and age, serum concentrations of TGFβ1 with VCAM-1 and hs-CRP, and hs-CRP and weight (Figure 5). Serum aldosterone correlated with stroke volume (r = 0.43, p = 0.006), cardiac output (r = 0.44, p = 0.004) and ICAM-1 (r = 0.40, p = 0.01) in women, but not in men.

Scatterplots and 95% confidence limits of the relations in women with untreated hypertension between systolic blood pressure and age, serum concentrations of vascular cell adhesion molecule 1 (VCAM-1), high-sensitivity C-reactive protein (hs-CRP) and transforming growth factor β1 (TGFβ1) and body weight.
Table 2 shows the presence of statistical gender differences in plasma concentrations of Ang II, serum aldosterone and hs-CRP in the subjects with both prehypertension and stage I hypertension. Baseline values for serum glucose, serum insulin, serum ICAM-1, VCAM-1 and P selectin were not different among women and men with different degrees of hypertension. Similarly, there were no differences in serum levels of TNFα and TGFβ1 between women and men at various stages of hypertension.
Profile of humoral biomarkers in women and men.

Values are mean ± standard error of the mean from 100 patients at baseline. p Values within table denote statistical difference between women and men for each of the three blood pressure categories.
hs-CRP, high-sensitivity C-reactive protein.
Discussion
Seldom, if ever, approaches to hypertension therapy consider sex as an element in the selection of antihypertensive agents or base the choice of a specific antihypertensive class in terms of the hemodynamic factors accounting for the blood pressure elevation. The present study provides a comprehensive noninvasive hemodynamic and hormonal assessment of hypertension in untreated men and women. The study documents important sex-driven differences in the contribution that cardiac output and peripheral vascular resistance make to the elevation of arterial pressure. Our study demonstrates that for equivalent levels of systolic and diastolic blood pressure elevations, women with untreated hypertension had higher pulse pressures, lower cardiac output values, higher systemic vascular resistance and reduced thoracic fluid content compared with men. This hemodynamic pattern in women was associated with higher baPWV and augmentation index. Since the hemodynamic characteristics found in women with hypertension did not change as a function of the hypertensive stages, these data suggest that these phenotypes are sex specific. However, differences in cardiac output and vascular resistance between men and women with hypertension were no longer significant after adjustment for body weight as the average weight of the male population was significantly higher. Since BMI in women and men with hypertension were not different, these findings suggest that normalization by weight is masking the higher degree of vascular constriction shown in women with hypertension. The differential hemodynamics of the two sexes extended to hormonal biomarkers of the hypertensive process since women displayed lower values of serum creatinine and higher circulating concentrations of leptin, Ang II, serum aldosterone and hs-CRP.
ICG is a simple accurate noninvasive method for measurement of stroke volume, cardiac output and thoracic fluid volume [Smith et al. 2006a]. Coupled with oscillometric measures of arterial pressure, peripheral vascular resistance is calculated from the cardiac output values determined by ICG. A number of studies have validated the sensitivity and reproducibility of this technique [Abdelhammed et al. 2005; DeMarzo, 2009; Ferrario et al. 2007; Ferrario and Smith, 2006; Siebenhofer et al. 1999; Smith et al. 2006a]. In a comparative study of healthy subjects with and without hypertension [Abdelhammed et al. 2005], we validated the differences in the hemodynamic factors accounting for the blood pressure elevation and showed the prospective value of this noninvasive technique in therapeutic decision-making in subjects with hypertension [Smith et al. 2006a]. DeMarzo reported on the value of ICG in detecting subclinical vascular disease in women [DeMarzo, 2009] while we showed that impedance cardiography guided therapy was more effective than standard care in achieving hypertension control in subjects on more than one antihypertensive medication [Smith et al. 2006a]. Pulse wave velocity and the augmentation index are now accepted methods for assessment of vascular stiffness [Hitsumoto, 2012; Rabkin et al. 2012; Salmi et al. 2012; Simova et al. 2011; Tomiyama and Yamashina, 2011; Yang et al. 2011; Zhang et al. 2013]. The strength of our current research is based on having combined hemodynamic measures with noninvasive indexes of vascular compliance in concert with concomitant measures of hypertension-related biomarkers. This approach provided a comprehensive picture of vascular disease in men and women and a glance at disease progression based on hypertensive stages.
Among the hypertensive participants, more men than women met the JNC-7 criteria for prehypertension and stage 2 hypertension. Despite the numerical differences in the sampled population, stroke volume and cardiac output were consistently lower in women with prehypertension and stage 1 hypertension compared with men. The higher degree of vasoconstriction found in women was no longer present in women with stage 2 hypertension. At these levels of arterial pressure, increased peripheral vascular resistance became the main mechanism accounting for hypertension. While it may be argued that the lower values of stroke volume and cardiac output found in women are an expression of the fact that their weight was less than that found in men, no statistical differences were found in BMI between men and women. In keeping with the suggestion that a higher vascular resistance contributes to the early stages of hypertension in women, baPWV and the augmentation index were higher in women compared with men. Reanalysis of these indices as a function of the hypertensive stages showed persistence of higher pulse wave velocity in women compared with men throughout the JNC-7 classification of hypertension. Differences were most notable in the augmentation index which was markedly less in men compared with women. Pulse pressures were higher in women with stage 1 and 2 hypertension. Altogether, these findings demonstrate a higher compromise of vascular elasticity in the early stages of hypertension in women compared with men. While our findings in general agree with previous studies of hemodynamic changes in subjects with prehypertension and hypertension [Drukteinis et al. 2007], partitioning of hemodynamic variables as a function of sex and hypertensive stages are not reported in the previous literature. Higashi and colleagues found a stronger association of the augmentation index with parameters of diastolic function in women with normotension compared with men [Drukteinis et al. 2007; Higashi et al. 2013]. While the mechanisms for this association remain to be investigated, a structural difference in the aortic tree in women may contribute to an earlier reflected pressure wave return and account for augmentation of the first forward wave during late systole [Hayward and Kelly, 1997]. In an earlier, well conducted study, Messerli and colleagues assessed the hemodynamic profile of men and women with essential hypertension in whom antihypertensive medications were discontinued 4 weeks beforehand [Messerli et al. 1987]. In their study, women were characterized as displaying higher cardiac index, left ventricular ejection time and pulse pressure, and a lower total peripheral resistance compared with men [Messerli et al. 1987]. The difference between our findings and those reported by Messerli and colleagues [Messerli et al. 1987] may be explained in part by the fact that our study was carried out in a patient population who were an average of 10 years older than those reported in their study; in addition, the hypertension in their study was less severe. This interpretation agrees with our findings of a significant correlation between systolic blood pressure and age in women (Figure 5), and the disappearance of the differential in cardiac output values between men and women with stage 2 hypertension (Figure 3).
The hemodynamic pattern found in women with essential hypertension suggests a higher more severe degree of vascular remodeling compared with men for the same levels of arterial pressure. This interpretation is supported by the demonstration of a pattern of hormonal biomarkers reflective of increased vascular inflammation and injury. The presence of significantly higher plasma Ang II concentrations, serum aldosterone and hs-CRP in women parallel a hemodynamic profile of higher vascular resistance and reduced vessel elasticity. The observation that circulating TGFβ1, a cytokine stimulating the production of various extracellular matrix proteins, correlated in women but not in men with serum VCAM-1 and hs-CRP is a novel finding that further reinforces the interpretation of significant loss of vascular elasticity as reflected by the increased pulse wave velocity and augmentation index. hs-CRP is an accepted biomarker of both acute and chronic inflammation [Tsimikas et al. 2006]. Although elevated levels of hs-CRP appear to be more predictive of mortality hazards in men compared with women [Doran et al. 2013], these findings do not negate its value as a marker of existent cardiovascular injury or inflammatory processes.
In this nondiabetic population of men and women with normal levels of fasting glucose and plasma insulin, we confirmed the existence of a large sex difference in plasma leptin values. This adipocytokine has an important role in energy homeostasis and circulating levels are reported to be higher in men than in women [Jeppesen and Asferg, 2010; Ugrinska et al. 2013]. In addition, recent studies showed that leptin is a biomarker of the amount of body fat and an important determinant of hypertension risk [Jeppesen and Asferg, 2010; Shankar et al. 2012]. In our subjects with untreated hypertension plasma leptin values were 2.5-fold higher in women than in men. In addition, plasma leptin correlated with both weight (r = 0.48, p < 0.05) and plasma insulin (r = 0.46, p < 0.05) in women, but only with weight (r = 0.56, p < 0.05) in men. Although a correlation between plasma leptin and BMI has been reported in healthy overweight women [Ugrinska et al. 2013], our findings of an additional sex difference in terms of its relation with plasma insulin is a new observation, the mechanism of which will require further investigation. Because our study showed that the higher leptin values were associated in women with other biomarkers of inflammation, our findings agree with the observations of Shankar and colleagues [Shankar et al. 2012] that high plasma leptin values are associated with a higher risk of hypertension.
Although differences in the prevalence, clinical presentation and development of hypertension-related complications in women are documented in numerous epidemiological and observational studies [Doumas et al. 2013], the applicability of this knowledge has not been fully translated in specific therapeutic strategies. Inclusion of women in antihypertensive trials is limited, while morbidity and mortality outcomes suggest that they receive less benefit from antihypertensive therapies [Kaplan, 1995]. Hypertension and impaired diastolic function with preserved left ventricular ejection fraction are seen more often in women, particularly after estrogen loss during menopause. Women develop diastolic heart failure twice as often as men and trials suggest angiotensin-converting enzyme inhibitors may be less effective in women than men receiving treatment for hypertension and heart failure. The differential hemodynamic and hormonal characteristics of untreated hypertension in the men and women included in our study suggest a need to better understand the female sex-specific underpinnings of the hypertensive processes to tailor optimal interventions for this vulnerable, yet expanding population.
Our hemodynamic and biochemical findings document a consistent pattern of a higher degree of vascular compromise and vasoconstriction in women compared with men for the same level of arterial pressure, most notably in prehypertension and stage I hypertension. These data lead us to hypothesize that the increased risk of cardiovascular events associated with the postmenopause stage may be anteceded or be accompanied by functional and structural vascular changes that may in part be a result of the differences in body habitus, body fat composition and shorter, narrower blood vessels compared with men.
Footnotes
Funding
We acknowledge partial support of these studies through an unrestricted grant provided by Daiichi Sankyo, Inc. (Parsippany, NJ, USA); from the National Heart, Blood, Lung Institute of the NIH through grant number HL-051952; and the former CardioDynamics Corporation (San Diego, CA, USA) for their generous gift the BioZ com equipment to CMF.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article. CM Ferrario has received funding from Daiichi Sankyo Inc., and has served as a member of their Speaker’s bureau.