
Abstract
Background:
Exposure to cold has been shown to cause cardiovascular stress and increased morbidity and mortality. Inhalation of cold, dry air can increase blood pressure and induce myocardial ischemia, particularly in people with preexisting hypertensive cardiovascular disease. Face masks that can warm and humidify inhaled cold air may reduce these cold air pressor effects.
Method:
We compared blood pressure measurements using a heat and moisture exchange mask (HME), a placebo mask (PL), and no mask (NM) in 53 patients with hypertension exposed to a cold chamber environment at −5°C for 1 h. Blood pressure and heart rate were recorded at baseline, and at 15 min intervals from 0 to 60 min of chamber exposure. All patients were taking antihypertensive medications with drug and dosage determined by their own physicians. Data were analyzed by a one-way analysis of variance test with repeated measures, and significant interactions were analyzed by Fisher’s least significant differences tests. A post hoc subgroup analysis for the effect of age was performed using Wilcoxon matched-pair rank tests.
Results:
Wearing the HME resulted in significantly lower systolic and mean arterial blood pressures than the PL and NM conditions. Diastolic blood pressures were significantly lower for the HME than the NM, but not the PL condition.
Conclusion:
Subgroup analyses suggested that the effect of the HME in mitigating systolic blood pressure increase from inhalation of cold air was significantly greater for patients aged 60 years or over than for those under 60 years.
Introduction
Exposure to cold imposes stress upon the cardiovascular system. It has been well documented that a decrease in ambient temperature is associated with increased cardiac morbidity and mortality [Boulay et al. 1999; Bull and Morton, 1975; Douglas et al. 1995; Gyllerup et al. 1991; Ornato et al. 1996; Sheth et al. 1999], stroke [Sheth et al. 1999; Hong et al. 2003], and all-cause mortality rates [Keatinge et al. 1989; Mackenbach et al. 1992]. This hypothermic-induced morbidity and mortality appears to center on an increase in blood pressure (BP), particularly in people with preexisting hypertension or ischemic heart disease [Brennan et al. 1982; Giaconi et al. 1989; Jehn et al. 2002; Korhonen et al. 2006; Kunes et al. 1991; Psaty et al. 2001; Woodhouse et al. 1993; Flack et al. 1995; Rabkin et al. 1978].
Our upper airway serves to warm and humidify inspired cold dry air, but at a physiologic cost [Regnard, 1992; Latvala et al. 1995]. At rest in a cold ambient environment, almost 10% of the body’s heat is lost via our respiratory system [Brebbia et al. 1957]. In addition, studies directed at exposure of the tracheobronchial tree to cold air have shown an increase in BP with the potential to induce episodes of angina [Lassvik and Areskog, 1980]. Furthermore, inhalation of cold air has been shown to produce myocardial ischemic diagnostic changes on single-photon emission computed tomography and thallium scanning, as well as a release of endothelin 1, a potent vasoconstrictor that notably has proved to be a marker in exercise-induced ischemia [Petersen et al. 1994; Lubov et al. 2001]. With decreasing temperatures of inspired air, this cooling effect can further potentiate the release of vasoconstrictors [Jaeger et al. 1980; Petersen et al. 1994; McFadden, 1983; McFadden et al. 1985; Zawadski et al. 1988; Watt et al. 1989]. Warming of inspired air might reduce these untoward effects [Petersen et al. 1994; Romet et al. 1988].
A heat and moisture exchange mask (HME) captures heat lost, as well as trapping water vapor upon exhalation. This trapped heat and water vapor can then be used to warm the cold dry inspired air via latent heat transfer. This state of exhaled heat and water vapor could help to achieve less cardiovascular stress by mitigating the effects of breathing cold and dry air. Besides the effect on cardiovascular diseases, the use of an HME in people with cold-induced asthmatic symptoms has been shown to be effective in reducing forced expiratory volume in 1 s, which some studies have reported to be more effective than inhaled albuterol treatments [Millqvist et al. 1995; Beuther and Martin, 2006]. To warm and humidify inspired air, a mask must contain an exchange medium that is freeze resistant. To date, no studies have reported findings using an HME, specifically assessing cold-air-induced increases in BP. Therefore, the purpose of this study was to evaluate the effect of an HME mask on BP during cold air inhalation in patients with hypertension.
Materials and methods
This study enrolled 53 patients with hypertension (30 women and 23 men) between 18 and 80 years of age (mean 56.7
Per protocol, the elapsed time between taking their hypertensive medication in the morning and data collection in the afternoon was standardized for all patients based on their procedural schedule. Three different treatment conditions during an exposure to cold inhalation were tested: the use of an HME (CT Mask, Airguard Medical Products, Memphis, TN, USA), a placebo mask without heat and moisture exchange capabilities (PL), and no mask (NM). Three separate assessments were performed for each patient with a minimum of 3 days between evaluations. The experimental design entailed 15 min of seated rest at an ambient room temperature of 23°C. During this rest interval, baseline BP, heart rate and peripheral oxygen saturation (SpO2) were measured. BP was measured with a calibrated Welch Allyn/Tycos TR-2 aneroid sphygmomanometer (Skaneateles Falls, NY, USA) and standard adult-sized arm cuff by an experienced technician of the Human Performance Laboratory. Duplicate measurements were obtained at each evaluation. Mean arterial pressure (MAP) was calculated. Heart rate and SpO2 were measured with a Nonin Medical pulse oximeter, model 8000H (Plymouth, MN, USA). Patients, dressed in winter clothing to minimize the convective and radiant cooling, then entered the cold chamber at −5°C and the same parameters were recorded in duplicate at 0, 15, 30, 45, and 60 min.
Statistics
Data were analyzed by a one-way analysis of variance with repeated measures. When a significant interaction was observed, comparative testing for significant F ratios was performed using Fisher’s least significant difference test. The α level of significance was established at 0.05. Subgroup analyses using Wilcoxon matched-pair tests were conducted to evaluate the relationship between age and the effects of the HME, PL, and NM treatment conditions on BP changes [LaVange and Koch, 2006]. These subgroup analyses were considered as exploratory and descriptive in accordance with accepted experimental design principles [Ellis et al. 2008].
Results
All 53 patients completed the study without experiencing any adverse events during the testing sessions. Baseline evaluation revealed no significant differences in mean systolic BPs or MAP between the HME, NM, and PL. However, during the cold exposure testing, there were significant differences between the groups. Systolic BPs, as well as MAP, were significantly lower for the HME than for the NM (p < 0.0001) and PL (p < 0.01) conditions (Table 1). There were no statistical differences in the MAP analysis between NM and PL conditions (p = 0.07). The lower systolic BP with the HME compared with either no mask or a placebo mask was immediate upon cold exposure. At 60 min, the difference was 12–13 mm, and the mean systolic pressure of HME wearers remained at or below 140 mm, not observed in either NM or PL evaluations.
Systolic and mean arterial blood pressure measurements during cold air inhalation.

One-way analysis of variance and Fisher’s least significant difference tests.
HME, heat/moisture exchange mask; SD, standard deviation.
Mean diastolic BP using HME was significantly lower than the findings in the NM condition (p < 0.0001), but did not differ from the PL condition (p = 0.15). Further data analysis revealed that the HME mask, in mitigating cold air induced systolic BP increases, may have a greater effect in older patients (Table 2). Post hoc subgroup comparisons of patients greater than 60 years of age demonstrated a significantly lower systolic BP effect with HME than with the NM and PL conditions at all measured time intervals. In patients under the age of 60 years, the HME was superior to the NM and PL treatment conditions only at 60 min. Tables 3 and 4 present the Wilcoxon matched pair results. No significant differences in heart rate or SpO2 were observed between any treatment conditions.
Systolic blood pressure during cold air inhalation: aged 60 years or over and aged less than 60 years.

BP, blood pressure; HME, heat/moisture exchange mask; SD, standard deviation.
Wilcoxon matched-pair two-tailed test for systolic blood pressure increase on cold air inhalation in treated patients with hypertension (aged 60 years and over; n = 25).
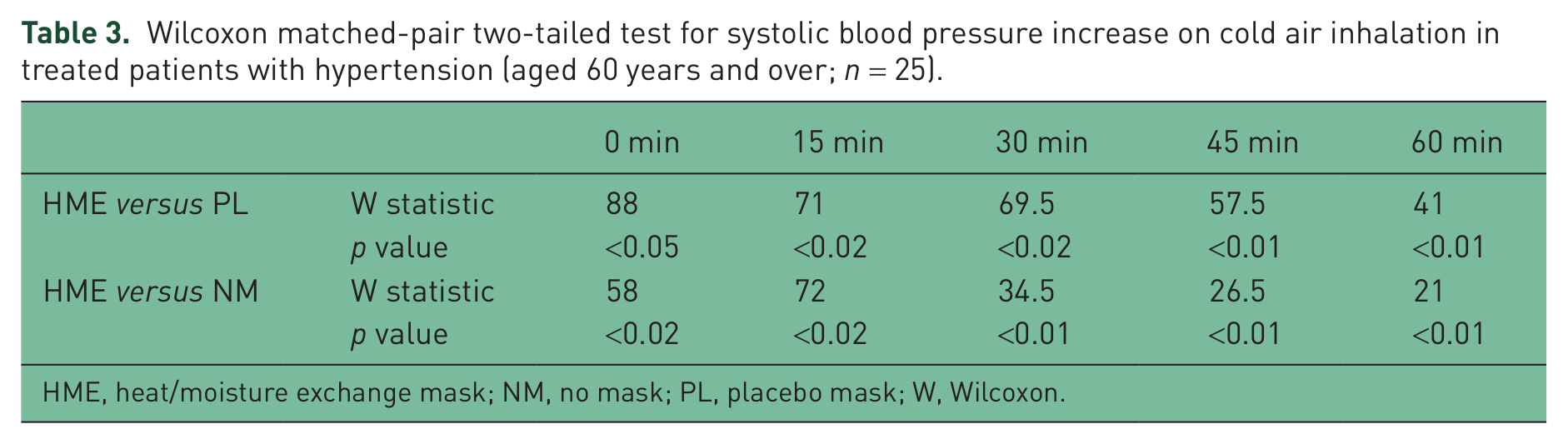
HME, heat/moisture exchange mask; NM, no mask; PL, placebo mask; W, Wilcoxon.
Wilcoxon matched-pair two-tailed test for systolic blood pressure increase on cold air inhalation in treated patients with hypertension (aged < 60 years; n = 28).

HME, heat/moisture exchange mask; NM, no mask; PL, placebo mask; NS, nonsignificant; W, Wilcoxon.
Discussion
Cold air exposure can pose significant health risks [Boulay et al. 1999; Bull and Morton, 1975; Douglas et al. 1995; Gyllerup et al. 1991; Ornato et al. 1996; Sheth et al. 1999; Hong et al. 2003; Keatinge et al. 1989; Mackenbach et al. 1992]. Our findings support this premise and support the results of Petersen and colleagues, reporting that cold air inhalation led to cardiovascular constriction [Petersen et al. 1994]. We observed that patients with known hypertension and treated effectively, in temperate environments, can experience significant elevations in systolic BP when inhaling cold air. Furthermore, we found a beneficial effect on BP when using an inhalation mask during exposure to the cold. The use of the HME mask significantly mitigated cold air induced increases in systolic BP, diastolic BP, and MAP in patients with hypertension. We found that the placebo condition exhibited a negligible effect on BP, such as using a scarf. A scarf can at least reduce the direct cold air effect on one’s face and may at best try to minimize the level of bronchoconstriction, but it does not provide the necessary warming and humidification of cold inspired air, which can be achieved with an HME mask.
A persistent elevation in systolic BP is associated with an increase in mortality due to events such as acute myocardial infarction and stroke. However, diastolic hypertension does not appear to have comparable risks or acute life-threatening events [Psaty et al. 2001; Lee et al. 1999]. Lassvik and Areskog reported that, during submaximal exercise, the inhalation of cold air can independently produce an elevation in BP [Lassvik and Areskog, 1980]. We found similar findings in our study population at rest. It is likely that if our study had used exercise, the positive findings might have been intensified, possibly due to an increase in minute volume ventilation with a subsequent increase in heat loss with vasoconstriction [Jaeger et al. 1980; McFadden, 1983; McFadden et al. 1985; Watt et al. 1989].
Inspired cold air directly affects our pulmonary airway. As cold air is inspired, levels of endothelin 1 are produced and released. Endothelin 1 stimulates peripheral vasoconstriction, as well as myocardial vasoconstriction with resultant ischemia [Petersen et al. 1994; Lubov et al. 2001]. Hemodynamically, peripheral vasoconstriction causes an increase in total peripheral resistance, placing increased stress on the heart with potentially elevating BP [Petersen et al. 1994; Jehn et al. 2002]. Millqvist and colleagues reported improvement in BP in patients wearing an HME mask during cold exposure [Millqvist et al. 1995]. An HME mask warmed inhaled cold air and significantly reduced pulmonary stress and heat loss, unlike the use of no mask or the use of a wool scarf. It is noteworthy that while a scarf may help minimize the level of bronchoconstriction, provided the dead air space is sufficient, the scarf does not offer the protection an HME mask provides. However, the problem with the HME mask that was used in the Millqvist study is that the thermal medium was made of a cellulose material which can absorb moisture and then has the potential to freeze as the environmental temperature drops below the freezing point or during prolonged exposure periods. Therefore, a mask should have a thermal medium resistant to freezing conditions.
The possibility of a greater benefit of the HME mask in patients over the age of 60 years definitely has additional clinical significance. The lower systolic BP with the HME versus the no mask and placebo mask conditions appeared rapidly on cold exposure. At 60 min, the difference was 12–13 mm, and the mean systolic BP of HME wearers remained at or below 140 mm, which was not the case for the NM and PL treatments. Post hoc analyses by Wilcoxon matched-pair rank tests revealed that for subjects older than 60 years, the HME was superior to the NM and PL conditions throughout the entire treatment session. For younger subjects the HME superiority was statistically significant at the 50 min time period. The incidence and degree of cardiovascular disease increases with age, therefore measures to minimize cardiopulmonary stress should be strongly considered. Subjecting an aging individual to cold situations has the potential to further stress an already compromised clinical condition. The use of an HME may have additional benefits beyond reduction in BP. Studies have reported that cold air inhalation in patients with coronary artery disease can precipitate myocardial vasoconstrictor peptide release, potentially precipitating ischemia [Dodds et al. 1995]. However, from a review of the literature and the findings in this initial study, the use of an HME should be strongly considered in individuals living in a cold climate and most importantly in those older than 60 years.
In another consideration, cold exposure may also lead to increased oxidative stress which, may lead to further complications in the clinical patient [Blagojevic et al. 2001; Marek et al. 2013]. Besides wearing an HME, one could argue that the use of nutraceutical supplements, such as various antioxidants and D-ribose, could offer a theoretical benefit to tissues subjected to ischemia or oxidative stress [Seifert et al. 2009; Jeserich et al. 1999; Ergonul et al. 2007]. Measured parameters of high-energy phosphates and oxidative stress metabolites may help in supporting this added dietary supplement premise. However, further research on this hypothesis is warranted.
Conclusion
An HME mask for cold exposure conditions can provide significant mitigation of cold air-induced increases in systolic BP, diastolic BP and MAP compared with NM and PL mask conditions in patients with diagnosed hypertension. While not isolating any certain pharmaceutical class, it is apparent that pharmaceuticals alone were not effective in minimizing hypertension during cold air inhalation. The benefit was greater in patients aged 60 years or over than in those under 60 years. Published reports centering on the increase in cardiovascular morbidity and mortality from cold, dry air inhalation would suggest that consideration in the use of an HME mask may provide a significant preventive benefit to people with hypertension, and the magnitude of this benefit may be more significant for those aged 60 years or over.
Footnotes
Funding
The study was funded by Polar Wrap, LLC, Memphis TN. Polar Wrap, LLC was not involved in the study design, data collection, analysis or interpretation of data, or in the preparation and writing of this manuscript.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.