
Abstract
Objectives
Aortic rupture may be second only to head injury as the primary cause of death following blunt trauma. The most common mechanisms include motor vehicle crash and the primary etiology is rapid acceleration/deceleration with shear forces applied at the ligamentum arteriosum, acute compression by the diaphragm, torsion of the aorta, and compression of the aorta between the sternum and spine [Baqué et al. 2006; Karmy-Jones and Jurkovic, 2004]. The likely outcome for patients sustaining these injuries is frequently fatal, with 85% of patients dying from massive hemorrhage at the scene. Owing to associated injuries, those that arrive at a hospital have mortality rates as high as 54% [Cook et al. 2006]. Traditionally such lesions has been treated with open repair (OR) and despite developments in operative techniques, there still remains considerable operative mortality and morbidity associated with a surgical approach [Razzouk et al. 2000]. Over the past decade more and more of these patients are being with endovascular stent grafts (endoluminal graft [ELG]). Several single-center studies have shown that ELG compares favorably with OR with respect to morbidity and mortality [Demetriades et al. 2008a, 2008b; Reisenman et al. 2007]. Most of these reports most likely represented best clinical outcome. We analyzed information from the National Trauma Databank (NTDB) of the United States of America to compare ELG versus OR for blunt aortic injury (BAI) with the belief that NTDB reported outcomes represent a contemporary national average and are free from reporting bias.
Methods
We queried the NTDB for the years 2002 to 2006. We selected patients who had one of their ICD (International Classification of Disease)-9 Diagnoses as 901.0, ‘injury to the thoracic aorta,’ whose mechanism of injury was motor vehicle accident, fall or other transport, whose discharge disposition was known, and who underwent endovascular or open repair (ICD-9 codes 39.73, ‘Endovascular repair of defect of thoracic aorta with graft(s) or device(s), stent graft(s) or device(s)’, or 38.45, ‘Resection of vessel with replacement, thoracic vessels’). Preoperative variables including Injury Severity Score (ISS) and Glasgow Coma Score (GCS) on presentation were collected. Outcomes analyzed included mortality, morbidity, ventilator days, total hospital and intensive care unit length of stay (LOS).
Morbidities analyzed were pulmonary adverse events, bacteremia, renal insufficiency or failure, surgical site infection, cardiac arrest or infarction, and nervous system adverse events (stroke/paraplegia). Preoperative risks and outcome rates were compared by repair type using Student’s t-tests or chi2 tests, p < 0.05 was considered significant.
Results
Survival rate, ICU and total hospital length of stay as well as ventilator days. Results were similar for patients undergoing open versus endoluminal repair for BAI.

ICU, intensive care unit; BAI, blunt aortic injury.
Morbidity outcomes. There were no significant differences in the complication rate after open versus endoluminal repair.
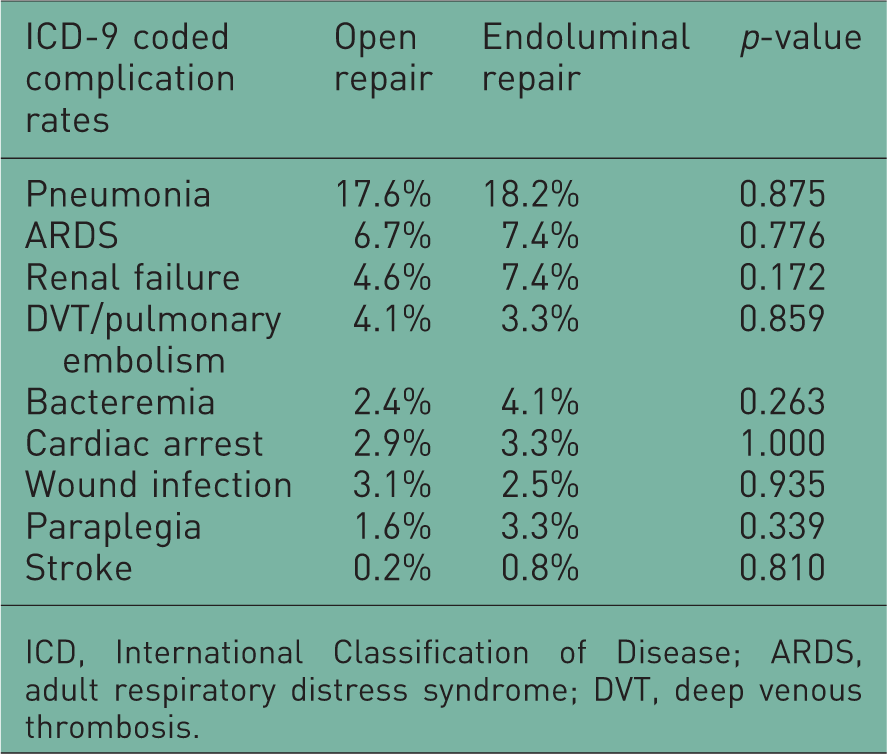
ICD, International Classification of Disease; ARDS, adult respiratory distress syndrome; DVT, deep venous thrombosis.
Discussion
Traumatic rupture of the thoracic aorta is often immediately fatal, approximately 80–90% of patients die in the field [Pierangeli et al. 2000; Galli et al. 1998; Gammie et al. 1998]. Patients who survive frequently have multiple system injuries, including pulmonary contusions, cranial injuries, multiple fractures, and solid organ injuries. Operative repair of a thoracic aortic injury in the setting of these other injuries is associated with significant morbidity and mortality; because of the high risk of immediate surgery, some have advocated delaying intervention with antihypertensive therapy until the patient is more stable [Maggisano et al. 1995; Pate et al. 1995]. Although this has enabled surgery after recovery from the acute trauma, complications remain high and delayed open surgery may lead to in-hospital death in 2–5% of patients [Jahromi et al. 2001]. The diagnosis and management of traumatic thoracic aortic injuries have undergone some major changes in the last few years. The replacement of chest X-rays and angiography by CT angiography, the introduction of beta blockers and delayed operation in selected cases, the liberal use of bypass techniques, the nonoperative management of selected cases and endovascular interventions has contributed to an earlier diagnosis and reduction of mortality and serious complications.
Following the initial reports of stent-graft repair of abdominal and thoracic aneurysm disease, surgeons have considered this minimally invasive approach for treatment of thoracic aortic disruptions [Dake et al. 1994]. Thoracic endovascular aortic repair is a rapidly applied, minimally invasive therapy that can be provided in conjunction with other major resuscitative procedures, and does not require resolution of comorbid injury. Although most studies are of limited numbers of patients with short-term follow up, data suggest that this is a safe and efficacious procedure. As the published evidence consists of nonrandomized small population studies there are no long-term data for this typically young patient population and the role of ELG for BAI has been evolving. Retrospective series have shown successful emergency repair of acute thoracic aortic disease by endovascular stent grafting [Czermak et al. 2000; Dake et al. 1999; Nienaber et al. 1999; Murgo et al. 1998; Semba et al. 1997]. Its use eliminates the need for extensive surgery with the attendant risks of anticoagulation, single-lung ventilation, aortic cross-clamping, and thoracotomy. There has been a rapidly increasing experience with endovascular repair of thoracic BAI and the ongoing development of improved commercially designed thoracic endograft devices. Two meta-analyses of BAI treated with endovascular repair have been reported with mortality rates of 7–7.6% and paraplegia rates of 0–0.7% [Tang et al. 2008; Xenos et al. 2008]. Both studies concluded that endovascular repair was superior to OR, and both of these reviews were based on a compilation of author-selected case series. Individual reports of BAI treated with endovascular repair are subject to reporting bias and often represent the best clinical outcomes from experienced operators. In our study, reporting bias does not have an influence on results, and we were unable to demonstrate a survival advantage for endovascular repair over OR. There was also no difference in the neurologic complication rate. Similarly, Demetriades and colleagues in a multicenter study of the AAST [Demetriades et al. 2008b] reported that OR was associated with a very low incidence of procedure-related paraplegia, which was not significantly higher than that with endovascular repair. This may be in part attributed to the very low incidence of paraplegia with OR in their study, only 2.9%. Based on the published literature, paraplegia is a very rare complication of BTA repair through the use of an endograft. In these cases of catheter and device manipulation and fixation at the arch, stroke remains a concern. However, the stroke incidence was 0.9% in the reviewed literature, which is more comparable to the rates accepted for cerebral angiography than the 3–4% rates reported in TEVAR for degenerative pathologic processes [Xenos et al. 2008]. In our study the incidence of stroke was 0.8% after ELG as compared with 0.2% after OR.
The following are potential limitations of our study. The NTDB, which is maintained by the American College of Surgeons, is a voluntary group of select trauma centers and is not a population-based sample. It is subject to potential coding and entry errors. Details of the exact operative procedures and techniques employed in a specific case as well as anatomic and radiologic information are not available. Reporting of postoperative complications (such as paraplegia) may differ among contributing centers. Furthermore, selection bias for determining whether ELG versus OR should be employed in each case could not be assessed. A randomized trial would be required to fully eliminate selection bias, which is unlikely for this patient population owing to the relatively small number of patients with these lesions, as well as ethical issues.
Conclusion
In summary, in a large, unselected patient population we were unable to establish a defined benefit for ELG versus OR for traumatic aortic thoracic injuries. Selected single-center studies have reported encouraging results with ELG; these centers typically have experience with both types of repair. After ELG potential concerns are stent graft failure, collapse due to the acute angle of the aortic arch in young patients, stent graft migration, and the need for repeat intervention. Obviously, the issue of durability of endovascular repair is highly relevant in younger patients, and patients with an endovascular graft for aortic rupture will have to be closely monitored for a long period of time. Nevertheless, many centers have reported a shift in the way thoracic aortic rupture is managed, using the endoluminal approach as the procedure of choice [Lebl et al. 2006]. Because it is not likely that randomized trials will be performed, prospective population-based studies including all patients with thoracic aortic rupture will provide the best attainable level of evidence on this issue but at this point it may be premature to adopt endoluminal repair as the new gold standard of thoracic aortic injury.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.