
Abstract
Poor early nutrition has varying effects on subsequent cardiometabolic disease (CMD) rates. Fetal and neonatal periods are critical for the development and growth of the systems involved in CMD. The increased rates of hypertension, metabolic syndrome, diabetes mellitus type 2, renal failure and heart failure observed nowadays in Latin America could be the result of the discrepancy between the nutritional environment during fetal and early life and the adult environment. This discrepancy causes a mismatch between the fetal programming of the subject and its adult circumstances created by the imposition of new life styles. The two largest international studies on cardiovascular risk factors for a first myocardial infarction (INTERHEART) and stroke (INTERSTROKE) demonstrated that in Latin America the factor with the highest attributable population risk was abdominal obesity. The conflict between the earlier programming and the later presence of abdominal obesity produced a higher sensitivity of this population to develop a state of low-degree inflammation, insulin resistance and the epidemic of CMD to lower levels of abdominal adiposity. The relative roles played by genetic and environmental factors and the interaction between the two are the still subjects of great debate. We have reviewed the relationship between maternal malnutrition, early growth restriction, epigenetic adaptations, and the later occurrence of abdominal obesity and CMD in Latin America.
Keywords
Introduction
Low birth weight remains an important public health problem in many regions of the World, especially in underdeveloped countries [Black et al. 2008; Fuller, 2000]. It may be a consequence of premature birth, genetic programming or intrauterine growth restriction. Intrauterine growth restriction is a consequence of maternal undernutrition, and placental dysfunction associated with preeclampsia and infections, factors that are related to the socio-economic status of the community [López-Jaramillo et al. 2008b, 2008c]. On the other hand, cardiometabolic diseases (CMDs) such as diabetes mellitus type 2 (DM2), metabolic syndrome (MS), myocardial infarction (MI) and stroke are the main causes of morbidity and mortality throughout the word [Murray and López, 1997; Murray et al. 1996] and have epidemic characteristics in underdeveloped countries [López-Jaramillo, 2008; López-Jaramillo et al. 2005, 2001]. It has been demonstrated that poor early nutrition has varying effects on subsequent CMD rates [López-Jaramillo, 2009; Gallou-Kabani and Junien, 2005]. The relative roles played by genetic and environmental factors and the interaction between the two remain the subject of much current debate. There is a growing body of evidence that suggests that epigenetic changes such as changes in histone modifications, chromatin structure and DNA methylation are a prime possibility [Gluckman et al. 2009; Gallou-Kabani and Junien, 2005]. Thus, the main goal of this article is to review the relationship between maternal undernutrition, early growth restriction, epigenetic adaptations, and the later occurrence of abdominal obesity and CMD in Latin America.
Fetal and neonatal development of systems involved in CMD under conditions of maternal malnutrition
Fetal and neonatal periods are critical for the development and growth of the systems involved in CMD. The human pancreas has already grown half of its adult beta-cell mass by 1 year of age [Rahier et al. 1981]. Thus, it may be anticipated that insults during these periods would be detrimental to glucose metabolism. Some years ago, Hales and colleagues demonstrated that men with a low birth weight were six times more likely to have diabetes at 64 years of age than men with a high birth weight [Hales et al. 1991]. Also, it was shown that the birth weight relationship was continuous across the normal birth weight range. In rats, detrimental effects on growth during fetal and early postnatal life can negatively affect both the number [Snoeck et al. 1990] and secretor function of pancreatic beta cells [Dahri et al. 1991]. Moreover, it has been demonstrated that children who had a low birth weight but had increased rates of growth from 7 years of age had a further increased risk of developing DM2 later in life [Barker et al. 1993]. Moreover, a series of studies have demonstrated a relationship between birth weight and child undernutrition and the presence of cardiovascular risk factors later in life [Laitinen et al. 2004; Forsen et al. 2000; Barker et al. 1990, 1989; Barker and Osmond, 1988; Forsdahl, 1979; Ravelli et al. 1976]. It is also known that individuals with low birth weights reduced kidney growth and a reduced number of nephrons [Sing et al. 2007; Brenner et al. 1988]. The result is a reduction in filtration area, which causes sodium retention and subsequently increased extracellular fluid volume, leading to increased cardiac output, total peripheral resistance and increased arterial blood pressure. Hence, individuals who suffered intrauterine growth restriction and thus have growth-restricted kidneys would be susceptible to hypertension in later life, especially if they became obese. Also, it has been reported that intrauterine growth restriction results in a decreased number of cardiomyocytes [Bubb et al. 2007; Corstius et al. 2005; Barbera et al. 2000; Samson et al. 2000]. So, it is interesting to speculate that the increased rates of hypertension, MS, DM2, renal failure and heart failure currently observed in Latin America could be the result of the discrepancy between the nutritional environmental during fetal and early life and the adult environment. This discrepancy causes a mismatch between the fetal programming of the subject and the adult circumstances created by the imposition of new life styles.
This proposal is supported in the thrifty phenotype hypothesis that was proposed by Hales and Barker suggesting that in response to poor fetal nutrition, the compromised fetus will adopt a number of strategies to maximize its chances of survival postnatally [Hales and Barker, 1992]. For instance, growth of the brain is spared at the expense of other tissues such as muscle, kidneys, cardiomyocytes, and pancreatic beta cells. Moreover, metabolic programming is proposed to occur in a manner beneficial to survival in conditions of poor postnatal nutrition. In this way, no problems arise if the fetus is born into conditions of poor postnatal nutrition and growth in the first years of the extra-uterine life under these conditions. The problems come if the malnourished fetus changes in the first years of life or in adolescence and the early adult life into conditions of adequate or overnutrition. The conflict between the earlier programming and the later presence of abdominal obesity associated with fast urbanization, the adoption of a sedentary lifestyle and a rich energy-food intake produce a state of low-degree inflammation, insulin resistance and a CMD epidemic.
The increased sensitivity to developing low-degree inflammation in response to abdominal obesity
Abdominal obesity is crucial in the adaptation process to the controversial situation between fetal programming and Western lifestyles [López-Jaramillo, 2009]. The relationship between obesity and the incidence of CMD was established several years ago. The Framingham cohort demonstrated that obesity is an independent predictor of CMD in both sexes [Hubert et al. 1983]. This relation became more evident in subsequent studies [Yusuf et al. 2005]. The IDEA study, performed in 63 countries with 170,000 subjects in primary care, concluded that, for an increase of 14 cm in waist circumference for men and of 14.9 cm for women, the probability of CMD rose from 21% to 40%.
Two cohort studies performed in Korea [Jee et al. 2006] and the United States [Adams et al. 2006] established that not only obesity but also being overweight are the main risk factors associated with the risk of death in subjects who have never smoked. The National Cholesterol Education Program Adult Treatment Panel III recognized being overweight and obesity as the major underlying risk factors for CMD, where adult obesity was more highly correlated with CVD than body mass index [National Cholesterol Education Program, 2001]. The International Diabetes Federation (IDF) established the presence of adult obesity as an obligatory criterion for the diagnosis of MS, which is strongly related to the development of CMD. Moreover, the IDF proposed a different threshold for waist circumference depending on regions and ethnic groups [Katzmarzyk et al. 2006].
In the Latin American population with no previous CVD history, our group reported that the criteria for MS proposed by the IDF are more useful for identifying subjects with MS than the Adult Treatment Panel III criteria [López-Jaramillo et al. 2007b]. In addition, several studies carried out in developing countries have reported lower waist circumference cutoff points associated with cardiovascular risk than those reported in developed countries. Misra and colleagues reported higher risks of cardiovascular events among Asian Indians with a waist circumference of 90 cm and greater and 80 cm and greater for men and women, respectively [Misra et al. 2006]. Similar results have been obtained in Latin American countries [Velasquez-Melendez et al. 2002; Berber et al. 2001]. In healthy young Colombian men, a waist circumference of 88 cm identified subjects with cardiovascular risk with a sensitivity of 83.7% and a specificity of 84.8% [Pérez et al. 2003]. In Ecuador [García et al. 2006], it was demonstrated that a waist circumference of 90 cm in men is the best cutoff point associated with the presence of at least two other MS criteria according to the National Cholesterol Education Program Adult Treatment Panel III.
Waist circumference has been demonstrated to be an easier parameter for evaluating the content of visceral fat, which is the main source of pro-inflammatory cytokines [Fain et al. 2004; Ahima and Flier, 2000; Fried et al. 1998]. These cytokines are elevated in the serum of obese subjects [Fontana et al. 2007], and it has been proposed that the systemic inflammation produced by adipose tissue participates in all stages of the development of CMD, such as endothelial dysfunction [Accini et al. 2007], atheroma formation, rupture of plaque, and acute thrombotic complications [Ross, 1999]. C-reactive protein (CRP), produced by the liver in response to the stimulus of tumor necrosis factor-alpha (TNF-α) and interleukin 6 (IL-6), is increased in subjects with multiple acute coronary events and is a strong independent predictor of new acute coronary events [Bogaty et al. 2001]. We have demonstrated in the Andean region that CRP is an independent risk factor for essential hypertension [Bautista et al. 2001] and preeclampsia [García et al. 2007a; Teran et al. 2001]. Moreover, the concentration of CRP is increased in dyslipidemic subjects with MS [García et al. 2007b] and in overweight children [López-Jaramillo et al. 2008a].
Regardless of the differences in the methods to quantify these inflammatory markers, we have observed that, in general, the concentration of pro-inflammatory cytokines is higher in the Latin American population than that reported in the population of developed countries, suggesting a higher sensitivity of this population to develop systemic low-degree inflammation as a response to abdominal obesity [López-Jaramillo et al. 2007a, 2002]. The importance of this observation was supported by the INTERHEART study [Lanas et al. 2007; Yusuf et al. 2004], which has identified risk factors associated with the presentation of a first acute myocardial infarction and has determined the population-attributable risk (PAR). Although the nine risk factors identified (changes in lipid profile, smoking, hypertension, abdominal obesity, psychosocial stress, changes in glucose metabolism, lack of physical activity, insufficient intake of fruit and vegetables, lack of moderate consumption of alcoholic drinks) explain more than 90% of the PAR in both men and women throughout the world, there was an important difference in the Latin American countries included (Chile, Colombia, Brazil, and Argentina). In those countries, AO was the most important risk factor (48.5%), a much higher figure than in the rest of the world (30.2%). In addition, in a similar population-based study in Costa Rica [Kabagambe et al. 2007], the PAR for acute myocardial infarction in 889 individuals without a history of DM2 who had not received any drugs, adult obesity was the most important risk factor (PAR, 29.3%), particularly among women (PAR, 35%).
Recently, the INTERSTROKE study [O’Donnell et al. 2010] has demonstrated that in the Latin American countries abdominal obesity has a high PAR to ischemic and hemorrhagic stroke. Moreover, the odds ratio (99% CI) for abdominal obesity was 3.82 (1.26–11.55) for the Latin American subjects, 3.34 (1.96–5.68) for individuals of high-income countries, 1.36 (0.99–1.85) for people from Southeast Asia, 1.35 (0.96–1.89) for Indians, and 1.73 (0.99–3.02) for people from Africa.
These results highlight the importance of AO among the Latin American population as the principal risk factor for acute myocardial infarction and stroke, a very troublesome finding given the epidemic of excess weight and obesity in these countries [Rueda-Clausen et al. 2008]. Recently, in a representative sample of school children in Bucaramanga, Colombia, we demonstrated a positive correlation between BMI, systolic blood pressure, and CRP [López-Jaramillo et al. 2008a]. This finding confirms in children the correlation demonstrated in Colombian adults, and reinforces the idea that there is a link between adiposity content, particularly in visceral regions, and increased plasma concentrations of inflammatory markers such as CRP. Several studies have assessed CRP concentrations in school children in developed countries [Ford, 2003; Gillum, 2003; Visser et al. 2001; Cook et al. 2000]. Cook and colleagues measured CRP concentrations in a representative sample of the population of England and Wales that included 699 children aged 10 to 11 years [Cook et al. 2000]. That study showed that serum concentrations of CRP correlated positively with BMI, heart rate, systolic blood pressure, fibrinogen, and high-density lipoproteins, but not with other lipid fractions. Interestingly, it was found that a small number of children of South Asian origin had CRP levels 2.04 times higher than those of age-, sex-, and BMI-matched children. Ford analyzed the results of the National Health and Nutrition Examination Survey of the United States (NHANES, 1999–2000), in which 2486 boys and girls aged between 3 and 17 years participated [Ford, 2003]. A multiple linear regression analysis showed that BMI was the best predictor of CRP plasma concentration. This study also found differences related to ethnic origin in boys aged 8 to 17 years and girls aged 8 to 11 years. Specifically, they observed a higher CRP concentration in children of Mexican-American origin in comparison with Caucasian-American children. In Colombia, we found a significant positive correlation between BMI and CRP and, as a result, higher levels of CRP among boys and girls in the upper tertile of BMI (Figure 1).
Plasma C-reactive protein (CRP) and systolic blood pressure (SBP) in Colombian school children by body mass index (BMI) tertiles (T).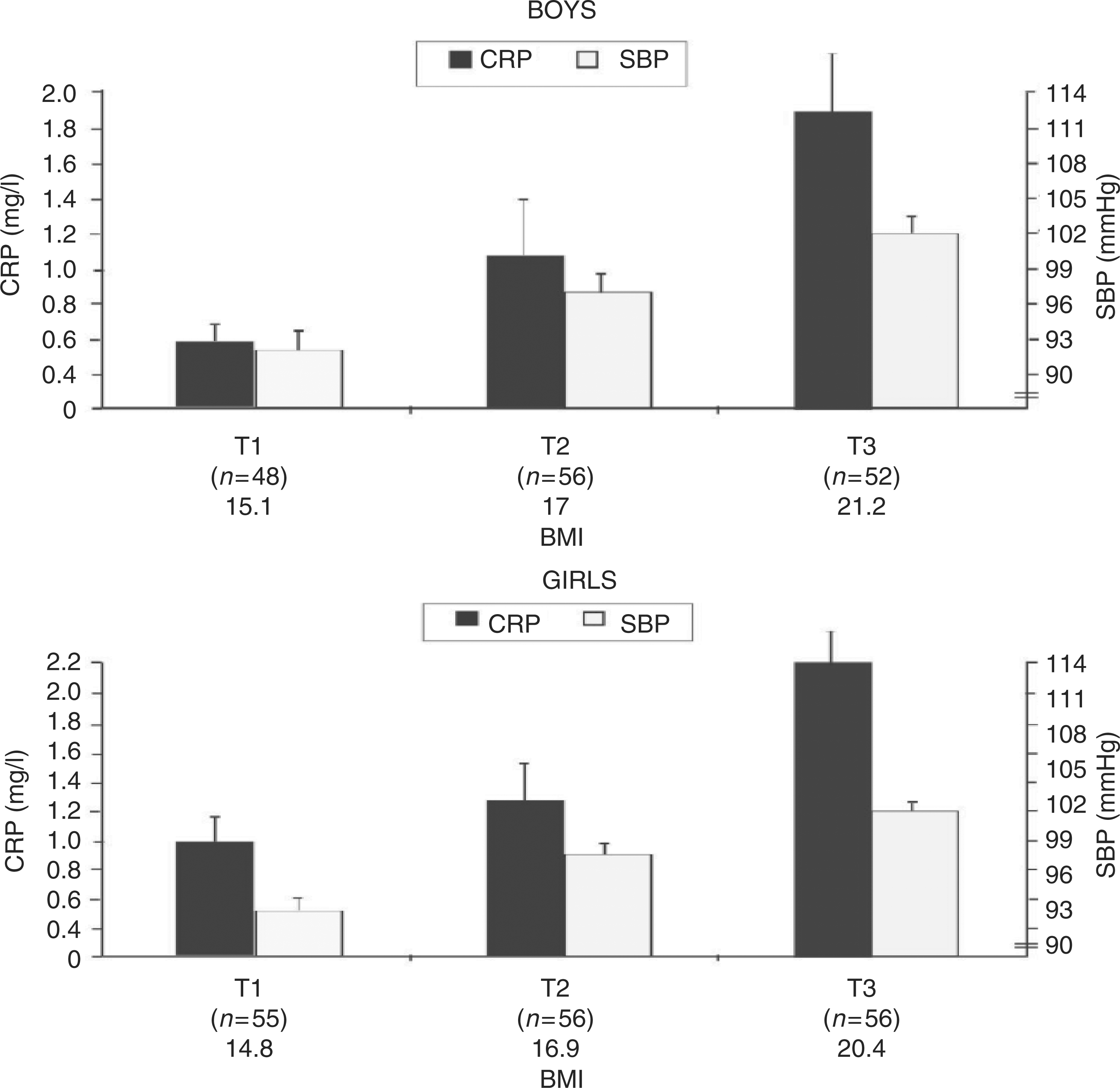
It is important to note that the concentrations of CRP that we encountered in the second tertile of BMI of both sexes in our population were as high as those registered in Caucasian-American children and European children of a similar age who were overweight or obese [Aeberli et al. 2006; Weiss et al. 2004]. Despite the possible differences in methodology for quantifying CRP in the different studies, and on the basis of data from our study in children and previous studies in our adult population [López-Jaramillo et al. 2008c; García et al. 2007b; Bautista et al. 2001] is it interesting to suggest the hypothesis that the Latin American population has a greater predisposition to generate an inflammatory response at lower body fat levels than those reported for Caucasian populations.
The question then is why are Latin American populations more sensitive to this process? We suggest that this is a result of less exposure time among the populations of developing countries to the new lifestyles associated with modernization. The shorter the exposure time, the less adapted the population is and there is a greater the risk of low-degree inflammation and insulin resistance at lower levels of abdominal obesity. It is well known that the Hispanic population in the United States and that the Hindu population in the United Kingdom are at greater risk for low-grade chronic inflammation, DM2 and cardiovascular mortality than the Caucasian populations of those countries [Chandalia et al. 2003; Chambers et al. 2001; Raji et al. 2001; Okosun et al. 2000]. However, it is currently not clear whether these differences are due to genetic or socioeconomic factors, as these groups migrated relatively recently to developed countries and have therefore only had less exposure to risk factors and are usually in lower socio-economic categories. Although there are no data from studies that have specifically investigated this problem, we believe that the length of exposure to the new living conditions generated by urbanization and modernity is an important risk factor for minority populations in developed countries [De Ferranti et al. 2004; Jaber et al. 2004; Ozsahin et al. 2004; Tan et al. 2004].
Nowadays, in Latin American countries, the bad habits and defects of the two worlds have collided: lack of potable water, defective waste and sewage removal, high rates of intestinal parasitism, nonpreventable infections and tropical diseases are all still present, but are now coupled with diets which are high in saturated fats and refined flours, more smoking, higher rates of physical inactivity, and abdominal obesity [O’Donnell et al. 2010; Rueda-Clausen et al. 2008; Kabagambe et al. 2007; Lanas et al. 2007; López-Jaramillo et al. 2007a, 2002; Yusuf et al. 2004].
The role of angiotensin II and adiponectin: epigenetic adaptations
Our proposal is that visceral adipocytes of people experiencing the rapid changes described above are overexpressing, by an epigenetic mechanism, the gene that regulates the synthesis of angiotensin II (Ang II). Ang II is produced in adipocytes [Van Harmelen et al. 2000; Karlsson et al. 1998; Jones et al. 1997], and it has been demonstrated that plasma levels of angiotensinogen and Ang II are increased with an increase in BMI [Harte et al. 2005]. Ang II has three important effects in humans, which were crucial to survival when human beings were nomads, fruit collectors, hunters and fishermen and had to endure long periods of starvation: (1) it blocks insulin intracellular signaling routes, producing insulin resistance, as a mechanism to retain energy [Muscogiuri et al. 2008]; (2) it stimulates the production of aldosterone, for maintaining sodium and water [Bader, 2010]; (3) it stimulates the production of pro-inflammatory cytokines, such as TNF-α, to maintain an alert state to fight infections [Arenas et al. 2004].
However, nowadays the production of Ang II in visceral adipocytes appears to be harmful since we have an excess energy intake and consume soft drinks. In this case, the insulin resistance and the water retention produced by Ang II are associated with hypertension and CMD, especially in Latin American countries where the excess of fast food and sedentary lifestyles are relatively recent [López-Jaramillo, 2009, 2008; López-Jaramillo et al. 2007a]. Moreover, it appears that the adaptation to this situation in obese people of developed countries, where the Western lifestyle is long lasting, is an overexpression of adiponectin, a substance that, in contrast to Ang II, improves the insulin sensitivity and has anti-inflammatory effects [Kadowaki et al. 2006]. A recent meta-analysis has shown that the risk of developing DM2 is lower in people with high levels of adiponectin in plasma [Shanshan et al. 2009]. So, we propose that the increased production of Ang II and the decreased production of adiponectin in visceral fat was a natural human biological response to the conditions of limited access to food and water. However, nowadays the imposition of Western lifestyles, which the humans in Latin America are not particularly well adapted to, is the main cause of the alterations that are leading to the epidemic of CMD.
In order to support this, we have recently demonstrated in an ex vivo model [Rueda-Clausen et al. 2010], using segments of internal mammary arteries obtained from individuals with severe coronary artery disease (CAD) who underwent coronary artery bypass grafts and were divided by the presence of adult obesity and matched by age, sex, glucose and insulin plasma levels, homeostatic model assessment (HOMA) index, lipid profile, tobacco and alcohol consumption, physical activity and arterial blood pressure, that the presence of adult obesity was related with a higher contractile response to Ang II. Moreover, in the plasma of these patients, progressive decreased levels of adiponectin and increased levels of leptin were observed, associated with an increase in the waist circumference (Figure 2). Moreover, in dyslipidemic patients with a clinically documented history of CAD we have observed higher concentrations of CRP and IL-6, when compared with dyslipidemic patients without a history of CAD [Rueda-Clausen et al. 2009]. The elevation of these inflammatory markers was not associated with any further impairment of endothelial function but was associated with a higher carotid intima-media thickness (IMT). Moreover, a positive correlation between the carotid IMT and plasma levels of the inflammatory markers was present only in subjects with a previous history of CAD. These results suggest that in our population there is a clear association between inflammation and the presence of a more severe stage of CAD.
Plasma levels of leptin and adiponectin in subjects with coronary artery disease (CAD) related to waist circumference. There is an increase in leptin (A) and a decrease in adiponectin (B) associated with higher values of waist circumference. In (C) we show the response ex vivo of segments of internal mammary artery with (__) and without endothelium (…) to the stimulus of angiotensin II (Ang II). The vasoconstrictor response is increased in the individuals with abdominal obesity (>90 cm in men and >80 cm in women) in relation with individuals without abdominal obesity (-AO) matched by age, sex and by other cardiovascular risk factors. (Adapted from Rueda-Clausen et al. [2010]).
Relevance of Ang II and leptin/adiponectin imbalance in metabolic alterations associated with obesity
Several experimental studies have pointed out the importance of Ang II in the metabolic and hormonal alterations associated with the model of diet-induced obesity. We have reported [De las Heras et al. 2009] that treatment with the AT1 receptor antagonist irbesartan reduced body weight gain, insulin resistance, dyslipidemia and ameliorated adipokine imbalance in obese rats fed a high-fat diet (HFD). The effect on body weight gain in rats was unrelated to a reduction of food intake and seemed to be due to a decrease in adipose tissue weight, as demonstrated by the reductions of epididymal and lumbar adipose tissue mass. This supports the concept on the involvement of Ang II in the regulation of fat mass by decreasing lipogenesis [Massiera et al. 2001]. Both circulating and locally formed Ang II contribute to the regulation of adipose tissue metabolism through Ang II AT1 receptors located in adipocytes [Crandall et al. 1994].
Ang II has been proposed as a trophic factor in white adipose tissue growth and development, since renin–angiotensin system components are regulated according to the nutritional state and adipose tissue mass [Boustany et al. 2004; Strazzullo and Galletti, 2004; Hainault et al. 2002; Janke et al. 2002; Kim et al. 2002; Saint-Marc et al. 2001]. Increase in thermogenesis could also participate in the reduction of body weight, and Ang II seems to be also related to this effect. In fact, the treatment of obese rats with irbesartan increased brown adipose tissue mass in these rats. The local renin–angiotensin system plays a role in adipocyte differentiation and in body-fat accumulation. In humans, Ang II produced by mature adipocytes appears to inhibit the differentiation of adipocyte precursors, thus decreasing the percentage of small insulin-sensitive adipocytes [Janke et al. 2002] and promoting the presence of large adipocytes, which decrease insulin sensitivity and produce ectopic deposition of lipids promoting the development of insulin resistance and type 2 diabetes [Weyer et al. 2000; Zorad et al. 1997].
Blockade of the renin–angiotensin system with either angiotensin-converting enzyme inhibitors or angiotensin receptor antagonists has been proven to have beneficial effects on adipocyte differentiation, substantially increasing the proportion of small adipocytes while the number of cells did not change [Jandeleit-Dahm et al. 2005]. Several studies have shown that treatment with Ang II AT1 receptor antagonists improved insulin resistance in obese, insulin-resistant or hypertensive animals and humans [Ran et al. 2004]. In animal studies, Ang II AT1 receptor blockers, enhanced insulin sensitivity and improved the serum lipid profile in rats that are obese or fed a high fructose diet [Okada et al. 2004; Ran et al. 2004; Navarro-Cid et al. 1995]. These effects are a consequence of the blockade of intracellular signals elicited by Ang II that are opposed to those of insulin in its target organs [Strazzullo and Galletti, 2004]. In addition, it should be proposed that the beneficial effects of AT1 receptor blockers on adipose tissue mass and insulin resistance in obesity conditions could be related to the enhancement of adiponectin expression, the reduction of leptin expression and the concomitant correction of leptin/adiponectin imbalance [Fasshauer et al. 2004].
Adiponectin effects on glucose metabolism and insulin sensitivity could be mediated through the phosphorylation and activation of AMP-activated kinase (AMPK) in skeletal muscle [Tomas et al. 2002], liver [Yamauchi et al. 2002] and adipocytes [Wu et al. 2003]. AMPK is a highly conserved heterotrimeric kinase that functions as a metabolic regulator of cellular enzymes involved in carbohydrate and fat metabolism, which regulate ATP conservation and synthesis. This signaling pathway affects many aspects of cellular metabolism including glucose uptake, glucose utilization and fatty acid oxidation [Russell et al. 2004; Wu et al. 2003; Marsin et al. 2000; Kudo et al. 1996]. Thus, it could be postulated that AT1 receptor blockers enhance glucose disposal and decrease free fatty acids, resulting in increased insulin sensitivity through the activation of AMPK by stimulated adiponectin and amelioration of the leptin/adiponectin imbalance. It has been proposed that both leptin and adiponectin gene expressions are partially under the control of PPAR-γ [Gustafson et al. 2003; Iwaki et al. 2003; Hollenberg et al. 1997]. Thus, the beneficial effects of angiotensin blockers on insulin resistance and the improvement of leptin/adiponectin imbalance could be a consequence of PPAR-γ activation or stimulation [Schupp et al. 2004].
TNF-α is a pro-inflammatory adipokine that impairs the action of insulin [Peraldi and Spiegelman, 1998; Hotamisligil et al. 1993] and suppresses PPAR-γ expression [Xing et al. 1997]. Thus, elevation of TNF-α in obesity states could be responsible for the reduced PPAR-γ expression and its mentioned metabolic consequences. In a recent study, we have observed that olmesartan improved insulin resistance and reduced inflammatory markers in patients with chronic kidney disease, without affecting plasma adipokine levels [De Vinuesa et al. 2006].
In summary, interactions between Ang II and leptin/adiponectin imbalance seem to play a key role in the metabolic alterations present in abdominal obesity and in the increased risk of developing cardio-metabolic diseases observed in Latin American countries.
Future perspectives
The Latin American immigrant population in southern European countries increased in an exponential manner in the past decade. According to data from the Spanish Ministry of Social Affairs, the European Commission and The United Nations Organization [Instituto Nacional de Estadística (España), 2008; Eurostat, 2006; United Nations, Department of Economic and Social Affairs, Population Division, 2006], there has been a sevenfold increase in the number of immigrants from Ecuador, Colombia, Bolivia, the Dominican Republic and Peru between 1995 and 2005. Women were predominant at the beginning of this migratory movement, but the number of men has increased in recent years, with the average age range being from 25 to 45 years old. Initially, incomes were low in general, but they became higher as the years went by.
This situation allowed these immigrant communities to improve their quality of life, but also in parallel, they experienced a marked change in lifestyle and nutritional habits [Aerny Perreten et al. 2010]. Rapid urbanization-derived habits, sedentary lifestyles and the consumption of high-energy foods, seems to be one of the main reasons for the elevated overweight and obesity rates among this immigrant population [García et al. 2009]. This could result in a significant increase in insulin resistance, MS and diabetes, and in the near future, it could be the main cause for the increase in cardiometabolic diseases. Supporting this notion is the recent demonstration in Sweden that parental country of birth is an important determinant of childhood diabetes [Hjern et al. 2008], and that diabetes prevalence is higher among the Asian immigrant populations in the United States, United Kingdom, and Canada compared with respective nationals [Rajpathak et al. 2009]. Although at the moment it is unknown whether a similar situation is occurring with the Latin American migrants in Europe, it is important to be aware of this possible future situation which could have a great economical impact on the public health system.
Footnotes
Funding
This work was partially supported by a grant from Ministerio de Educacion y Ciencia of Spain (SAF 2007-81595).
Conflict of interest statement
None declared.
Acknowledgements
The authors of this manuscript certify that they have complied with the Principles of Ethical Publishing [Coats, 2009].