
Abstract
Introduction
Hypertension is a major risk factor for cardiovascular disease [Kannel, 1995] and is an important leading cause of global mortality in five of the six World Health Organization regions [WHO, 2002]. It is also the third most important contributor to the global disease burden among six risk factors of underweight, unsafe sex, hypertension, unsafe water, tobacco and alcohol abuse [WHO, 2002]. Hypertension, a causal factor for cardiovascular disease is itself a result of certain risk factors such as heredity, increased salt intake, obesity, physical inactivity, excess alcohol use, low potassium diet, low vegetable and fruit intake and high saturated fat diet [Adeyemo et al. 2002; Sacks et al. 2001]. Hypertensive patients often die prematurely usually as a result of the systemic effects of hypertension on the cardiovascular, neurological and renal systems; with heart failure, stroke and renal failure as the most common causes of mortality [Williams, 2001].
There is clear evidence that the treatment of hypertension is beneficial irrespective of the drug type used [Turnbull, 2003]. Recent emerging chronotherapeutic studies [Hermida et al. 2007a; Minutolo et al. 2007] have demonstrated effective blood pressure control and a significant reduction in cardiovascular events following selected patterns of drug use. Chronotherapy takes into consideration time of day when medications are given. Night-time chronotherapy is being canvassed [Hermida and Smolensky, 2004] as this timing attenuates the morning blood pressure surge and returns day-time and night-time blood pressures to the normal circadian pattern. The result is adequate cover of the night-time period when most cardiovascular and cerebral events have been reported to occur [Elliot, 1998]. Most studies on chronotherapy have been performed in the West and there is a paucity of data on this beneficial approach in Nigeria. It was cautioned that this finding should not be generalized until replicated in any population. There is therefore the need to carry out such studies to appreciate any benefits of chronotherapy on our hypertensive population; as it constitutes a new option in optimizing blood pressure control and reduce risk [Hermida et al. 2005].
Methods
We performed an interventional randomized controlled clinical trial involving 181 patients with grades 1 and 2 hypertension consecutively recruited from the Cardiology Unit Medical Outpatients Clinic of Jos University Teaching Hospital, Jos, Nigeria between last quarter of 2007 and first quarter of 2008. By means of a table of random numbers, they were divided into two treatment groups on once-daily antihypertensive medication(s). Those who had been on treatment before enrolment were given a compulsory 2-week washout period. Excluded were current smokers, chronic alcoholic abuse patients, grade 3 hypertensives, those with clinical or laboratory evidence of secondary hypertension, those with significant renal impairment (serum creatinine >200 µmol/l) and pregnant/lactating females. One group (group A) had their drug(s) in the morning (10:00) and the other group (group B) had their drugs at night (22:00).
They all started on a thiazide diuretic or where contraindicated on a single other drug (calcium channel blocker, beta blocker or blocker of the renin–angiotensin system) appropriate for their clinical condition. A second drug was added at the 2-week review in patients who were not controlled, that is, those whose blood pressures were >20/10 mmHg above target blood pressure [Chobanian et al. 2003]. At the point of enrolment all patients underwent full physical examination and investigations. Office blood pressure was taken by standard sphygmomanometry after about 5 minutes rest. An average of two readings taken about 10 minutes apart was used for analysis. MAP was derived in the standard fashion from SBP and DBP. Height (h) was measured using a stadiometer without footwear or headgear in meters and weight (w) was measured using a weighing scale in kilograms. From these BMI was calculated from the formula weight divided by the height squared. Electrocardiography was performed using a ‘Cardiovit AT plus’ machine and Araoye code used for defining left ventricular hypertrophy (LVH) [Araoye, 1996]. Echocardiography was performed using a ‘LOGIC 5 EXPERT’ machine for LVSD and LVPWD. LVM was determined from above data using the standard formula [Sahn et al. 1978].
The first and second visits after enrolment were at 2 and 6 weeks, respectively. These were devoted to drug review if control had not been achieved, ensure compliance and assess whether any complication had developed. On the third and last visit 12 weeks into treatment all investigations performed at enrolment were repeated. Only 165 patients completed the study and form the cohort on which we report. Ninety patients had been randomized to morning dosing but 9 were lost to follow up leaving 81 for final analysis. Ninety one were randomized to the night dosing and 7 were lost to follow up leaving 84 available for analysis at the end. All patients signed the written informed consent forms and the protocol was approved by the research ethics committee of Jos University Teaching Hospital.
Statistics
Results are expressed as means ± SD. The two-tailed Student’s t-test was used for comparison of group means. Chi-squared tests were used to determine the significance of associations in comparing categories or proportions. Statistical significance was set at p < 0.05. Data were analyzed with Microsoft Excel statistics software.
Results
Demographic and physical characteristics of subjects at baseline.

Data represent mean (SD).
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure.
Echocardiographic data of subjects at baseline.

Data represent mean (SD).
IVSD, interventricular septum diameter; LVPWD, left ventricular posterior diameter; LVEDD, left ventricular end diastolic diameter; LVM, left ventricular mass.
Mean change in subjects’ physical and echocardiographic characteristics from enrolment to study completion at 12 weeks.
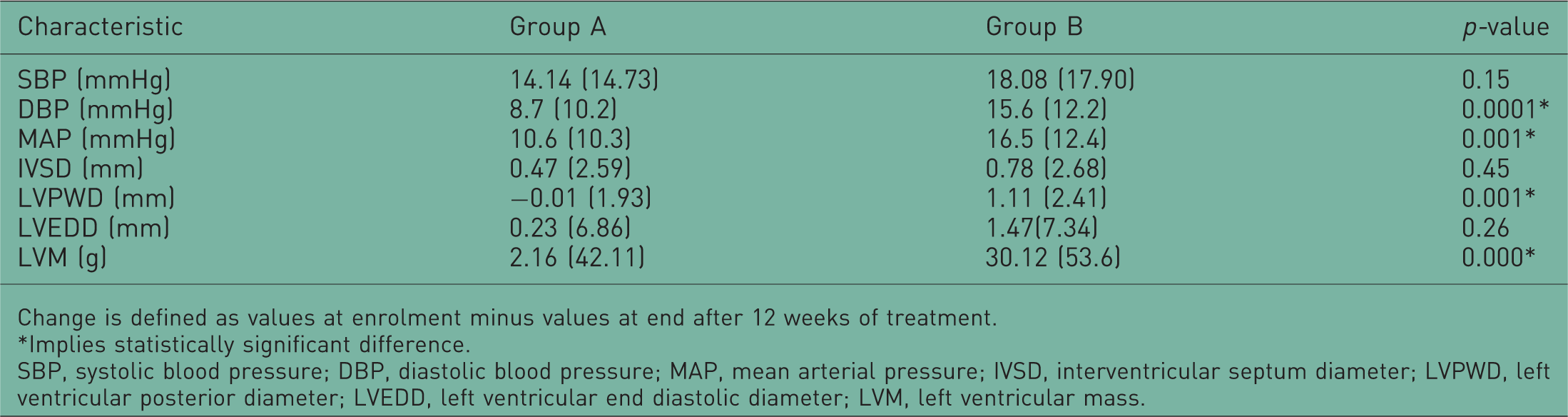
Change is defined as values at enrolment minus values at end after 12 weeks of treatment.
Implies statistically significant difference.
SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; IVSD, interventricular septum diameter; LVPWD, left ventricular posterior diameter; LVEDD, left ventricular end diastolic diameter; LVM, left ventricular mass.
Only three subjects developed heart failure, one in group A and two in group B. There was no difference in proportion between groups and they were treated appropriately. No stroke or myocardial infarction occurred in either group during the study. Drug use analysis at the end of the study showed that all subjects required at least one and at most three antihypertensive agents. Group A required a mean of 1.6 drugs in contrast to 1.4 in group B. The most common drug used was thiazide diuretic followed by calcium blockers, beta blockers and renin–angiotensin system blockers (angiogenesis receptor and angiotensin-converting enzyme inhibitor blockers).
Discussion
Chronotherapeutic studies done in other parts of the world and using different drug classes have met with significant success [Hermida et al. 2008; Hermida and Ayala, 2009]. Switching drugs from morning to night [Minutolo et al. 2007] as well as night-time dosing for add-on medication [Ikeda et al. 2007; Kario et al. 2000] have been shown to control blood pressure and lead to regression of LVH. These have largely been among Whites prompting a caution that results should not yet be generalized [Hermida and Ayala, 2009]. The present study has been conducted among Nigerians who are Black Africans resident in sub-Saharan Africa. At the onset, both groups randomized into morning and night-time intake of their antihypertensives were similar in demographic and physical characteristics (Table 1), as well as echocardiographic LVH parameters. That makes them good groups for comparison with any intervention. We were able to reproduce the findings among Whites, namely better control of blood pressure and reduction of the LVH response in hypertension (Table 3). The reasons for better blood pressure control with night-time dosing have been thought to include normalization of the abnormal dipping pattern [Kario et al. 2000]. Since nondipping is related to an increase in end organ injury [Brotman et al. 2008], its correction spares end organs from damage including kidney disease and left ventricular disease. Kidney disease sustains elevated blood pressure and slowing or aborting its progression will result in better blood pressure control [Minutolo et al. 2007]. LVH is the normal response of the left ventricle to increased afterload, the hallmark of systemic arterial hypertension. Night-time administration of drugs caused more significant regression of LVPWD and LVM. There was a greater tendency for reduction in IVSD which did not attain statistically significant difference. This regression of LVH is because of the greater reduction at night of blood pressure indices including MAP. In rats, cardiac enlargement has been found to be determined principally by blood pressure during sleep [Morgan et al. 2000]. Other than normalization of dipping pattern, antihypertensives such as renin–angiotensin system blockers should work better at night since renin–angiotensin aldosterone system is activated more during the nocturnal sleep span [Hermida et al. 2007b]. Circadian rhythms in gastric pH and emptying, gastrointestinal motility, biliary function and circulation to abdominal organs also alter pharmacokinetics of antihypertensives in such ways that they are more effective given at night [Labrecque and Beauchamp, 2003]. Finally glomerular filtration rate has a circadian pattern of hitting a maximum during the day and a minimum at night [Koopman et al. 1989]. Drugs are therefore cleared slowly and could potentially act for longer. The fact that four major classes of antihypertensives were used in this study also implies that each drug class could potentially produce this desirable effect when given at night albeit at different rates [Morgan and Anderson, 2003]. However, for thiazides which cause diuresis capable of disturbing sleep, hence countering the beneficial effects, it would be preferred if at least one of the other drugs (since most hypertensives would require two or more drugs) is given at night. Since sleep blood pressure predicts cardiovascular and cerebrovascular ischemic events while awake blood pressure predicts haemorrhagic strokes [Kikuya et al. 2005], night-time administration, which reduces sleeping blood pressure better than morning administration and improves prevalence of controlled ambulatory blood pressure [Hermida and Ayala, 2009], stands to reduce morbidity and mortality statistics of hypertension more impressively.
In conclusion, night-time chronotherapy benefits Black Africans as much as Whites and should become a useful tool in the treatment of hypertension in sub-Saharan Africa.
Footnotes
Acknowledgement
We are grateful to Dr Aigbe Ohihoin for assistance with statistical analysis of the data.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.