
Abstract
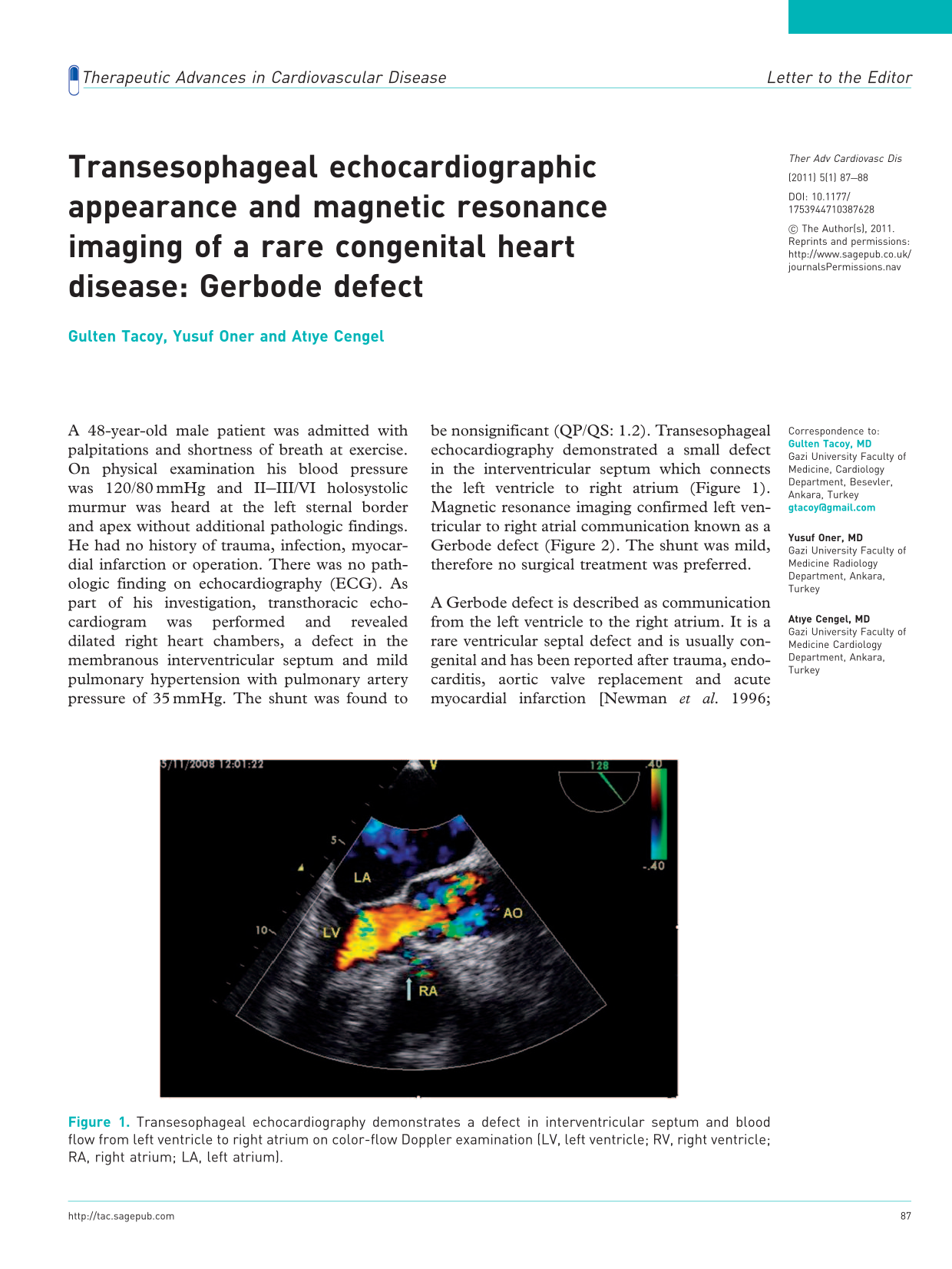
A 48-year-old male patient was admitted with palpitations and shortness of breath at exercise. On physical examination his blood pressure was 120/80 mmHg and II–III/VI holosystolic murmur was heard at the left sternal border and apex without additional pathologic findings. He had no history of trauma, infection, myocardial infarction or operation. There was no pathologic finding on echocardiography (ECG). As part of his investigation, transthoracic echocardiogram was performed and revealed dilated right heart chambers, a defect in the membranous interventricular septum and mild pulmonary hypertension with pulmonary artery pressure of 35 mmHg. The shunt was found to be nonsignificant (QP/QS: 1.2). Transesophageal echocardiography demonstrated a small defect in the interventricular septum which connects the left ventricle to right atrium (Figure 1). Magnetic resonance imaging confirmed left ventricular to right atrial communication known as a Gerbode defect (Figure 2). The shunt was mild, therefore no surgical treatment was preferred.
Transesophageal echocardiography demonstrates a defect in interventricular septum and blood flow from left ventricle to right atrium on color-flow Doppler examination (LV, left ventricle; RV, right ventricle; RA, right atrium; LA, left atrium). MRI demonstrates communication between left ventricle and right atrium (LV, left ventricle; RV, right ventricle; RA, right atrium; LA, left atrium).

A Gerbode defect is described as communication from the left ventricle to the right atrium. It is a rare ventricular septal defect and is usually congenital and has been reported after trauma, endocarditis, aortic valve replacement and acute myocardial infarction [Newman et al. 1996; Gerbode et al. 1958]. Echocardiography and MRI are useful tools for the diagnosis of Gerbode defects.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.