
Abstract
Background
Concerns about COVID-19-associated coagulopathy (CAC) in pregnant individuals were raised in early pandemic.
Methods
An ISTH-sponsored COVID-19 coagulopathy in pregnancy (COV-PREG-COAG) international registry was developed to describe incidence of coagulopathy, VTE, and anticoagulation in this group.
Results
All pregnant patients with COVID-19 from participating centers were entered, providing 430 pregnancies for the first pandemic wave. Isolated abnormal coagulation parameters were seen in 20%; more often with moderate/severe disease than asymptomatic/mild disease (49% vs 15%; p < 0.0001). No one met the ISTH criteria for disseminated intravascular coagulopathy (DIC), though 5/21 (24%) met the pregnancy DIC score. There was no difference in antepartum hemorrhage (APH) with asymptomatic/mild disease versus moderate/severe disease (3.4% vs 7.7%; p = 0.135). More individuals with moderate/severe disease experienced postpartum hemorrhage (PPH) (22.4% vs 9.3%; p = 0.006). There were no arterial thrombotic events. Only one COVID-associated venous thromboembolism (VTE) was reported.
Conclusions
Low rates of coagulopathy, bleeding, and thrombosis were observed among pregnant people in the first pandemic wave.
Background
COVID-19 infection remains a major public health challenge, with considerable morbidity and mortality, and continuing threat from new variants. 1 It became apparent early in the pandemic that patients hospitalized with COVID-19 had an increased risk of thromboembolic events.2–5 Subsequent observations linked these events to a newly defined entity termed COVID-19-associated coagulopathy (CAC). 6 CAC comprises microvascular and macrovascular thrombosis, initially within the pulmonary vasculature but with a risk of progression to life-threatening acute lung injury, and multiorgan dysfunction. 7 Initially, it was anticipated that due to its inherent hypercoagulable state, with higher levels of fibrinogen, von Willebrand factor, factor VII, and factor VIII and with increased levels of D-dimers, 8 pregnancy with concurrent COVID-19 infection would be more susceptible to CAC.7,9
With a sharp increase in reports of CAC, including suggestion of disseminated intravascular coagulopathy and venous thromboembolism, in the non-pregnant population, and concerning early case reports of CAC in pregnant individuals,10–13 a communication from the International Society on Thrombosis and Hemostasis (ISTH)'s Scientific Standardization Committee (SSC) for Women's Health outlined preliminary recommendations for management of CAC in pregnancy. 14 Owing to the paucity of data regarding CAC in this population, establishment of an international registry was recommended. The objective of this report was to leverage data from the ISTH-sponsored, COVID-19 coagulopathy in pregnancy (COV-PREG-COAG) registry, to describe (a) the incidence of coagulopathy, (b) the incidence of VTE, and (c) use of anticoagulation in COVID-19-affected pregnancies.
Methods
Registry questionnaire
The COV-PREG-COAG international registry is administered in the form of an online case report form (CRF), consisting of 569 elements (https://redcap.isth.org/surveys/?s=4JPX9W98RH).
Based on known differences in management for these populations, COVID-19 severity was defined as asymptomatic (SARS-CoV-2 positive, without clinical symptoms), mild (outpatient management), moderate (hospitalization, without critical care), or severe (intensive care unit admission).15,16
Postpartum hemorrhage was defined as estimated blood loss of greater than 1000 mL, regardless of the mode of delivery. 17 Preterm birth was defined as birth before 37 weeks’ gestation, and early preterm birth as birth before 34 weeks’ gestation. 17 Small for gestational age (SGA) was defined as birthweight below 10th centile for gestational age. 18 Determination of the presence of other obstetric complications, such as gestational hypertension, pre-eclampsia, HELLP, gestational diabetes, cholestasis, and antepartum bleeding (APH), was left up to the individual centers, based on documentation of these conditions in their patient records. Pregnancy- and trimester-specific laboratory parameter ranges were used to determine laboratory abnormalities, 19 with values below the lower normal range considered as “cytopenias” (e.g., thrombocytopenia, leukopenia, etc.) and those above the upper normal range considered as “cytosis” (e.g., thrombocytosis, leukocytosis, etc.).
Documentation of various biochemical parameters was sought, based on their previously reported prognostic value in COVID-19.20,21 Because CAC was an emerging concept and lacked an accepted definition at the time of the registry's inception, the survey definition encompassed “any coagulation parameter abnormality, bleeding or thrombotic event.” Questions regarding anticoagulation focused on low-molecular-weight heparin (LMWH), given its role as the preferred agent in pregnancy.22,23 Registry entries were based on data provided by the respondent and did not involve a formal chart review. The study received ethics approval at each participating institution. In the UK, this included Health Research Authority and Health and Care Research Wales Approval. Data were handled in line with information governance regulations. Ethics approval without requirement for consent was likewise granted in the USA and Canada. Data entry proceeded under a study number with removal of any identifying information such as medical record number, date of birth, or hospital site.
An invitation to participate in the registry, with a web-link for access, was distributed through email via specialist societies, including the ISTH, Canadian Society of Maternal–Fetal Medicine, and British Maternal–Fetal Medicine Society. Social media platforms were also utilized to raise awareness of the registry and encourage participation.
Clinical data for each case were abstracted from relevant clinical charts and hospital records by local registry contributors, for entry directly into a Research Electronic Data Capture (REDCap) database, hosted on the ISTH website. A downloadable form of the questionnaire was also included on the website as an alternative where REDCap entry was not feasible.
Data analysis
Data were downloaded into an SPSS database that included all records and fields contained within the questionnaire, and descriptive statistics were carried out. Frequencies and percentages were used to summarize categorical variables. Depending on normality of distribution, means (standard deviations) or medians (interquartile ranges) were used for continuous variables, as appropriate. Group comparisons for categorical variables were made using chi-squared tests or Fisher's exact tests, as appropriate.
Results
Representatives of several institutions contacted the project leads (AKM, SK, MO) and entered data into the registry, which included 430 pregnancies for the first wave of the pandemic, with variable degree of detail recorded. Consecutive cases of COVID-19 in pregnancy from the participating institutions were captured.
Maternal demographic details are shown in Table 1, as are maternal co-morbidities and risk factors for venous thromboembolism (VTE).
Maternal demographics.
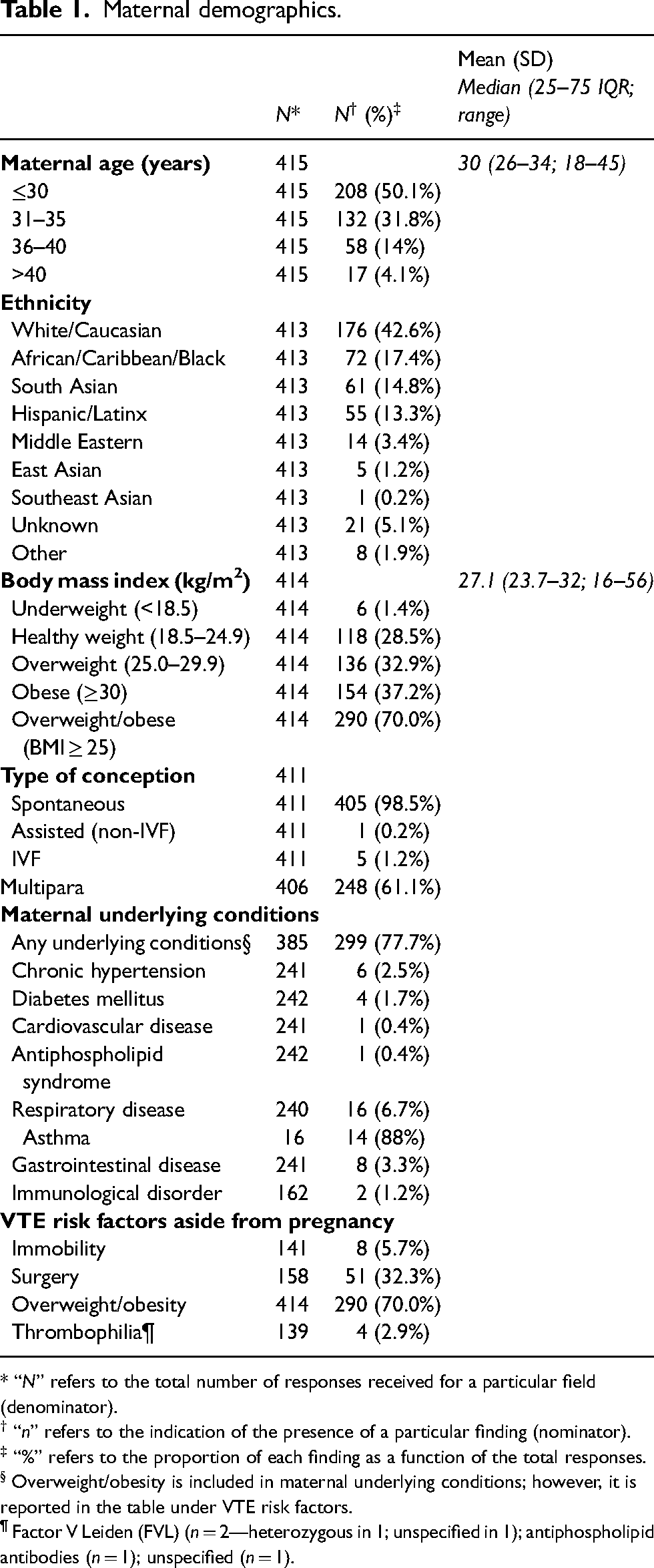
* “N” refers to the total number of responses received for a particular field (denominator).
† “n” refers to the indication of the presence of a particular finding (nominator).
‡ “%” refers to the proportion of each finding as a function of the total responses.
§ Overweight/obesity is included in maternal underlying conditions; however, it is reported in the table under VTE risk factors.
¶ Factor V Leiden (FVL) (n = 2—heterozygous in 1; unspecified in 1); antiphospholipid antibodies (n = 1); unspecified (n = 1).
Table 2 presents characteristics of COVID-19 infection, including details of testing, symptomatology, and disease course. Diagnosis was most frequent in the third trimester (321, 75%), and the majority of cases (255, 60%) were asymptomatic. Hospitalization was required in 53 (31%) of those who were symptomatic, with intensive care unit (ICU) admission in 10 (19%) of hospitalized individuals. Oxygenation via high-flow nasal cannula was necessary in seven (2.1%) individuals, non-invasive mechanical ventilation in six (1.8%), and invasive mechanical ventilation (IMV) in six (1.8%). No one received extracorporeal membrane oxygenation (ECMO), and there were no maternal deaths.
Clinical characteristics of COVID-19 infection course.
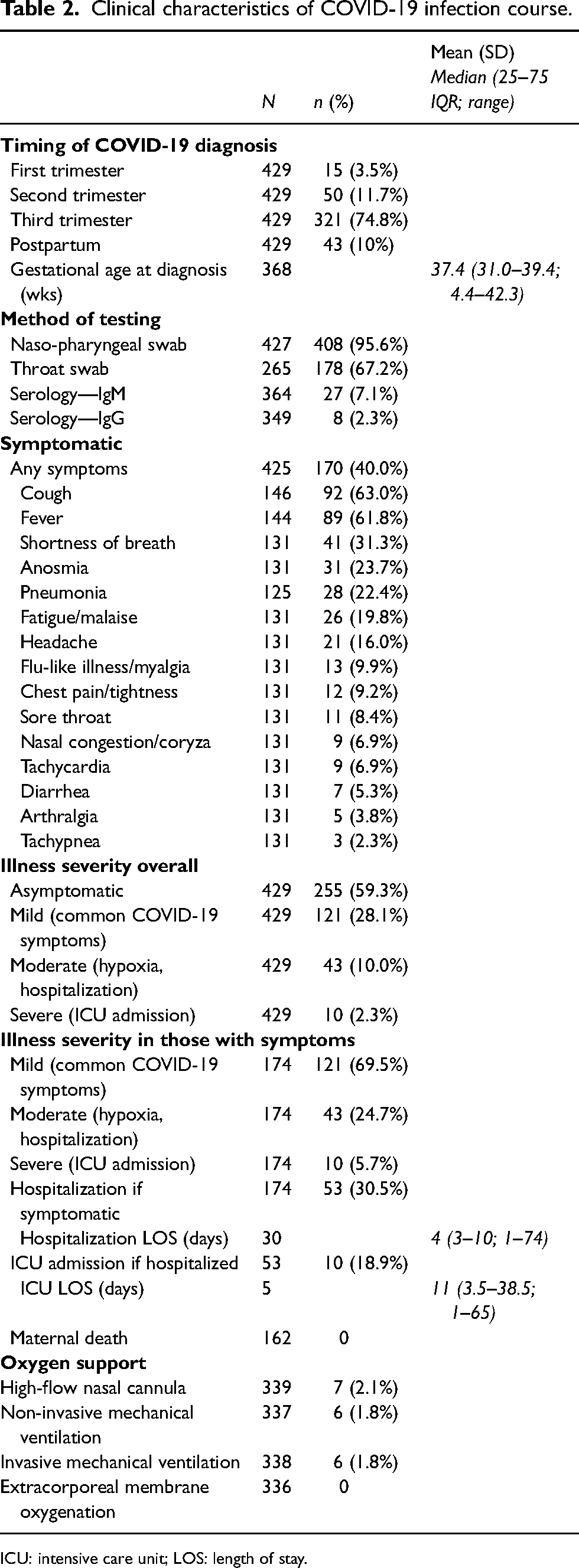
ICU: intensive care unit; LOS: length of stay.
Details of general hematological and coagulation-specific parameters are summarized in Table 3. There were no illness severity-based differences for most of the general laboratory parameters. Conversely, significant differences for asymptomatic/mild illness and moderate/severe illness were observed for leukopenia and hyperferritinemia, both of which were higher in the moderate/severe group. Hypoferritinemia was observed more frequently in the asymptomatic/mild illness group. Isolated abnormal coagulation parameters were seen in 70 (20%), according to pregnancy- and trimester-specific values. 19 These included thrombocytopenia (13%), thrombocytosis (3%), prolonged APTT (16%), hypofibrinogenemia (30%), hyperfibrinogenemia (13%), and elevated D-dimer (67%). More individuals with moderate/severe disease experienced isolated coagulation abnormalities in comparison to those with asymptomatic/mild disease (49% vs 15%; p < 0.0001). Prolonged APTT was noted only in individuals with moderate/severe disease. None of the participants met the criteria for disseminated intravascular coagulopathy (DIC) per the ISTH definition, 24 though 5/21 (24%) of those for whom all hematological parameters were available met the pregnancy DIC score. 25
Pregnancy- and trimester-specific laboratory parameters 19 according to severity of COVID-19 infection.
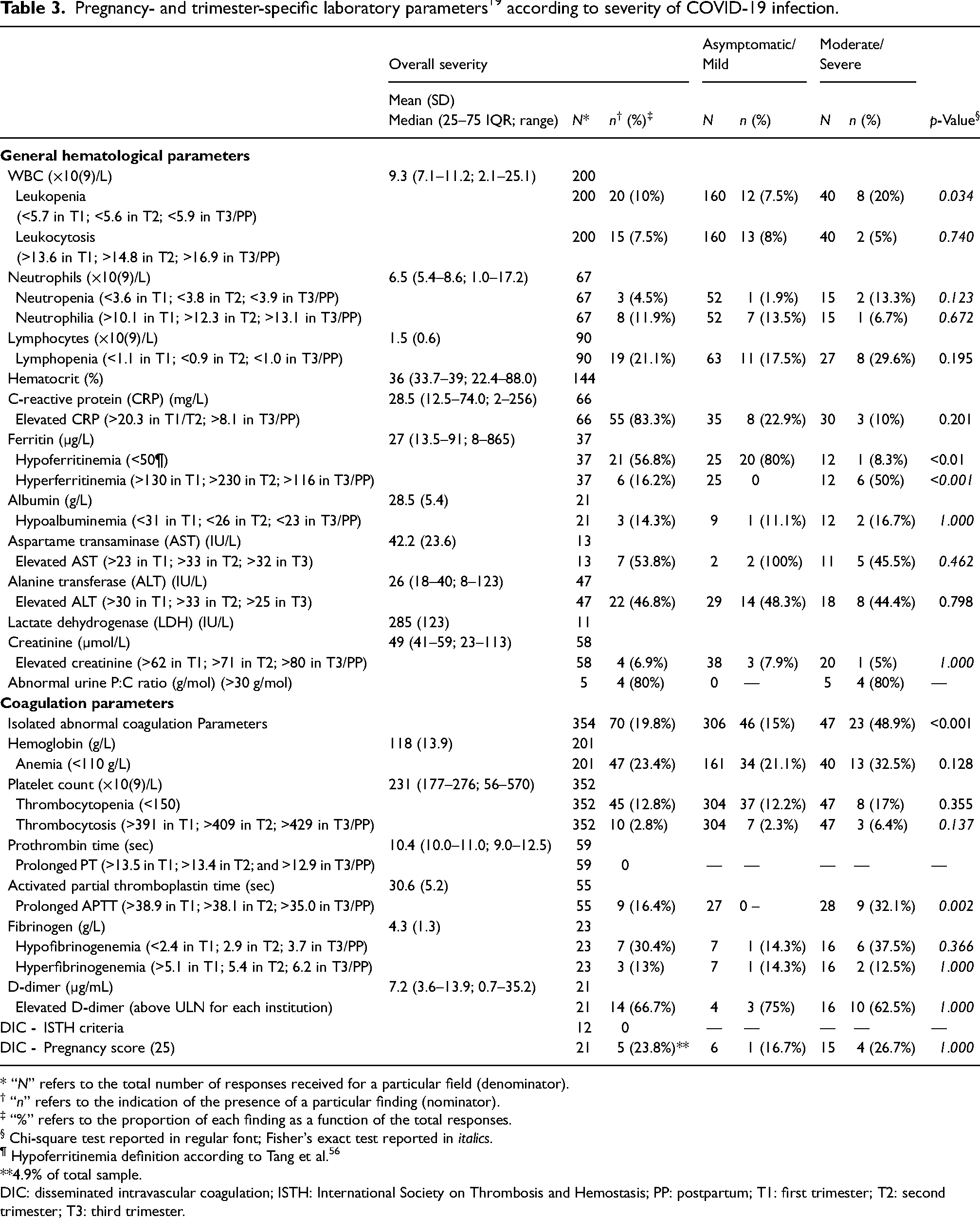
* “N” refers to the total number of responses received for a particular field (denominator).
† “n” refers to the indication of the presence of a particular finding (nominator).
‡ “%” refers to the proportion of each finding as a function of the total responses.
§ Chi-square test reported in regular font; Fisher's exact test reported in italics.
¶ Hypoferritinemia definition according to Tang et al. 56
**4.9% of total sample.
DIC: disseminated intravascular coagulation; ISTH: International Society on Thrombosis and Hemostasis; PP: postpartum; T1: first trimester; T2: second trimester; T3: third trimester.
Data on bleeding and thrombosis is presented in Table 4. There was no difference in APH between those with asymptomatic/mild disease and those with moderate/severe disease (3.4% vs 7.7%; p = 0.135). Conversely, more individuals with moderate/severe disease experienced PPH compared to those with asymptomatic/mild disease (22.4% vs 9.3%; p = 0.006), with more urgent or emergent Caesarean deliveries in the moderate/severe group (44% vs 18.8%; p < 0.001). There were no reported arterial thrombotic events. Only one VTE was observed. This was in the form of a pulmonary embolism on post-operative day 5 after an urgent Caesarean delivery, despite thromboprophylaxis with LMWH.
Pregnancy outcomes.
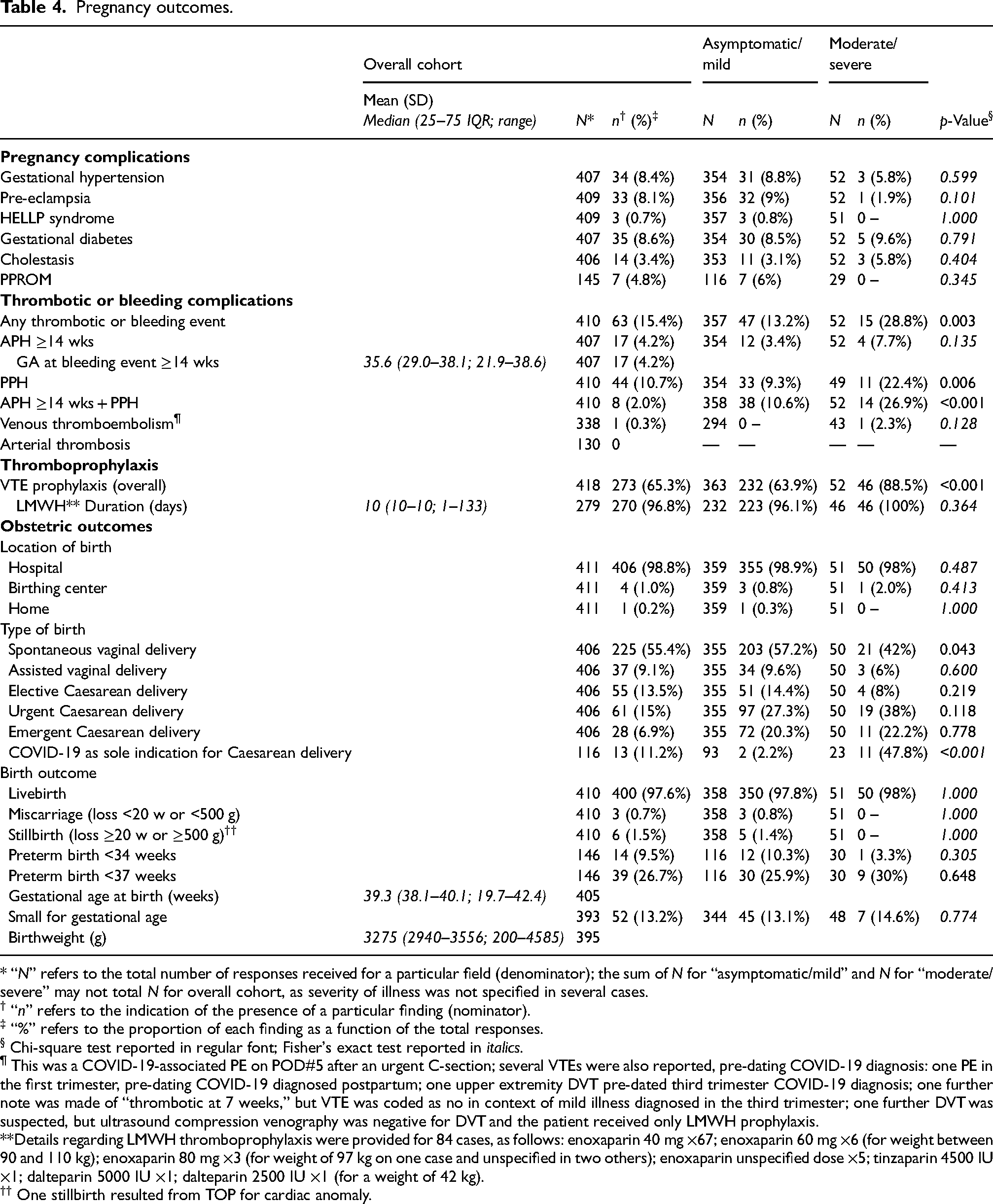
* “N” refers to the total number of responses received for a particular field (denominator); the sum of N for “asymptomatic/mild” and N for “moderate/severe” may not total N for overall cohort, as severity of illness was not specified in several cases.
† “n” refers to the indication of the presence of a particular finding (nominator).
‡ “%” refers to the proportion of each finding as a function of the total responses.
§ Chi-square test reported in regular font; Fisher's exact test reported in italics.
¶ This was a COVID-19-associated PE on POD#5 after an urgent C-section; several VTEs were also reported, pre-dating COVID-19 diagnosis: one PE in the first trimester, pre-dating COVID-19 diagnosed postpartum; one upper extremity DVT pre-dated third trimester COVID-19 diagnosis; one further note was made of “thrombotic at 7 weeks,” but VTE was coded as no in context of mild illness diagnosed in the third trimester; one further DVT was suspected, but ultrasound compression venography was negative for DVT and the patient received only LMWH prophylaxis.
**Details regarding LMWH thromboprophylaxis were provided for 84 cases, as follows: enoxaparin 40 mg ×67; enoxaparin 60 mg ×6 (for weight between 90 and 110 kg); enoxaparin 80 mg ×3 (for weight of 97 kg on one case and unspecified in two others); enoxaparin unspecified dose ×5; tinzaparin 4500 IU ×1; dalteparin 5000 IU ×1; dalteparin 2500 IU ×1 (for a weight of 42 kg).
†† One stillbirth resulted from TOP for cardiac anomaly.
The incidence of PPH did not differ between those who did and those who did not meet the criteria (1/4 with PPH vs 3/4 without PPH, p = 1.000), although the numbers are likely too small to appreciate a difference. The sole person who experienced a VTE did not meet the criteria for the pregnancy DIC score.
Thromboprophylaxis was provided more frequently in those with moderate/severe illness than with asymptomatic/mild illness (64% vs 89%; p < 0.001). Postpartum thromboprophylaxis was recorded in 90% of cases, with data available for 27% of the sample. Details of agent and dose were available in 84 cases, with standard prophylactic doses in the majority, and select cases of weight-based thromboprophylaxis (enoxaparin 40 mg in 67 cases, enoxaparin 60 mg in six cases (weight 90–110 kg), enoxaparin 80 mg in three cases (weight 97 kg in one and unspecified in two others), enoxaparin at unspecified dose in five cases, and in one case each tinzaparin 4500 IU, dalteparin 5000 IU, and dalteparin 2500 IU (weight 42 kg)).
Data on pregnancy complications and obstetric outcomes are shown in Table 4. There were no differences between illness severity groups for the majority of pregnancy complications and obstetric outcomes. Vaginal delivery was achieved more often in those with asymptomatic/mild illness compared with moderate/severe illness. COVID-19 as a sole indication for Caesarean delivery was more frequent in those with moderate/severe illness than in those with asymptomatic/mild illness (47.8% vs 2.2%; p < 0.001).
Conclusions
Principal findings
This report of the ISTH-sponsored COV-PREG-COAG international registry includes data from 430 individuals in the first wave of COVID-19 infection. Moderate or severe COVID-19 disease was recorded in 30% of individuals. Isolated abnormal coagulation parameters were seen in 20%, with a higher number of individuals with moderate or severe disease experiencing isolated abnormal coagulation parameters in comparison to those who were asymptomatic or had mild disease. None of the participants met the criteria for DIC per the ISTH, though 24% of those for whom all hematological parameters were available met the pregnancy DIC score. There was no difference in APH between those who were asymptomatic or had mild disease and those with moderate or severe disease; however, a higher number of individuals with moderate or severe disease experienced PPH in comparison to those who were asymptomatic or had mild disease. There were no reported arterial thrombotic events. Only one COVID-associated VTE was reported. Thromboprophylaxis was provided more frequently in those with moderate or severe illness than in those who were asymptomatic or had mild illness.
Results in context of literature
Clinical outcomes
Consistent with reported literature, our findings suggest a higher risk of COVID-19 in those of non-Caucasian ethnicity, multiparous patients, and those with underlying medical conditions, most notably obesity. 26 Likewise, in keeping with published reports is the mild nature of the illness in the majority27,28 and predominance of cough, fever, and shortness of breath in those who were symptomatic, as in the non-pregnant population. 29
Of those who were symptomatic, 31% were hospitalized, and of those hospitalized, 19% required ICU admission. Comparison to the initial reports from China concerning the general population demonstrates slightly higher rates of hospitalization in our symptomatic pregnant patients (20% vs 31%) and slightly higher ICU admission in those who were hospitalized (5–15% vs 19%). 29
COVID-19 diagnosis was most often made in the third trimester (75%) at a median gestational age of 37.4 weeks; potentially explained by universal screening adopted by countries like the USA and the UK for any individual attending hospital for any reason, including labor and birth,30,31 although the practice of universal screening was more variable in Canadian centers, despite similar timing of diagnosis. 32
General hematological and coagulation parameters
Anemia (hemoglobin below 100 g/L) was observed in 23% of our sample, compared to 5% observed with COVID-19 outside of pregnancy. 32 The higher rate of anemia in pregnancy may be partially related to the physiologic hemodilution of pregnancy, alongside a high prevalence of iron deficiency.19,33
In our sample, elevated CRP was seen in 83%, elevated AST in 54%, elevated ALT in 47%, and high creatinine in 7%. Abnormalities in these parameters have been shown to be predictive of severe illness, hospitalization, or worse outcomes in the non-pregnant population.34,35,36,37
Conversely, hyperferritinemia was seen in only 16% of pregnant patients, while hypoferritinemia was noted in 57%. Whereas hyperferritinemia in the non-pregnant population with COVID-19 has been associated with illness severity, its relative infrequency in this pregnant population may be explained by the prevalence of iron deficiency in this cohort. 33 Furthermore, the relatively higher rate of hypoferritinemia in those with asymptomatic/mild illness and relatively higher rate of hyperferritinemia with moderate/severe disease are likely attributable to ferritin's role as an acute-phase reactant.
As with the non-pregnant population, 38 we noted approximately half of those with moderate/severe disease exhibited an abnormality in at least one coagulation parameter (vs 15% with mild disease). Gestational thrombocytopenia can accompany 7–12% of otherwise uncomplicated pregnancies; 39 thus we are unable to comment whether thrombocytopenia observed herein was directly related to COVID-19. Reassuringly, thrombocytopenia was mild, with only two cases of severe thrombocytopenia, one in moderate/severe disease, and one owing to chronic liver disease.
DIC involves a dysfunctional activation of the coagulation cascade, which can be incited by a number of catalysts including injury, sepsis, or pregnancy-related events such as placental abruption, stillbirth, HELLP syndrome, or obstetric hemorrhage. 40 In 2001, the ISTH proposed a definition of DIC, which incorporated assessment of the platelet count, fibrin-related markers (D-dimer or fibrin degradation products), PT, and fibrinogen; the committee further acknowledged that DIC can be overt or non-overt, with the diagnosis of the latter hampered by the insensitivity of these global coagulation parameters. 41 Using the ISTH definition, there were no cases of DIC in our study. However, the physiologic changes of pregnancy leading to an increase in pro-coagulant activity, designed to anticipate the potential peripartum blood loss, render the application of the ISTH DIC definition problematic, as it reflects the non-pregnant state. 40 To account for these physiologic adaptations, the pregnancy DIC score was developed and validated. 25 It includes modified criteria for the platelet count, fibrinogen, as well as the assessment of the difference in PT (calculated from the patient's result as compared to the average control for a given laboratory), while it excludes D-dimer, the values of which are typically increased in pregnancy. 40 Given these stipulations, we calculated the pregnancy DIC score, which met the criteria in 24% of patients in our study for whom all hematological parameters were available. 25 However, the incidence of PPH did not differ between those who did and those who did not meet the criteria for the pregnancy DIC score. The sole person who experienced a VTE likewise did not meet criteria for the pregnancy DIC score. Given the small number of patients for whom all necessary parameters were available to calculate the pregnancy DIC score, its association with clinical bleeding or thrombotic outcomes remains unclear and requires further study.
It is worth noting that the pattern of anemia, low-platelet counts, and elevated liver enzymes encountered in non-pregnant patients with COVID-19, in pregnancy may be mistaken for HELLP syndrome, a condition warranting delivery to achieve resolution. 42 However, while delivery is the cure for HELLP syndrome, it will not alter the course of COVID-19 and may add unnecessary risks: (a) to the mother through exposure to the physiologic and potentially surgical stresses of birth when medically unwell and (b) to the infant if iatrogenically premature.13,43,44 To add complexity, it is worth noting the increased risk ratio for pre-eclampsia in nulliparous individuals with COVID-19 in pregnancy (RR 1.89; 95% CI 1.17–3.05). 45 Careful differentiation of whether the clinical and laboratory alterations represent a hypertensive disorder of pregnancy or whether they are purely reflective of the underlying COVID-19 is vital and will help guide the most appropriate management. The following parameters can be helpful in considering pre-eclampsia/HELLP as the inciting event: elevated blood pressure (if present), inappropriate adaptation of uterine artery blood flow, and elevated soluble fms-like tyrosine kinase-1 or decreased placental growth factor where their measurements are feasible. 44
Bleeding and thrombosis
Bleeding complications were noted in 15% of our sample, with APH after the first trimester in 4% and PPH in 11%. While disease severity did not influence APH rates, individuals with moderate/severe disease had higher rates of PPH, observed in nearly 25%. The higher incidence of PPH in those with more severe illness may have been influenced by the higher rate of urgent or emergent Caesarean delivery within this group.
Non-pregnant patients hospitalized with COVID-19 have been shown to have a higher risk of thromboembolic events,2,3,4,5 later linked with the presence of CAC. 6 With these observations, there was a concern that the additional hypercoagulable state of pregnancy will potentiate thrombotic risk. Interestingly, only one COVID-associated VTE was reported in our first-wave sample, which occurred despite LMWH thromboprophylaxis. This lower-than-expected incidence of thrombosis in the pregnant population may have been mitigated by thromboprophylaxis in two-thirds of the sample for whom data was available and in 90% postpartum. This perhaps underscores the importance of continuing this practice, which has now been supported by a number of studies outside of pregnancy,46,47,48 although it does require further scrutiny in the pregnant population.
Pregnancy complications and obstetric outcomes
Pregnancy has now been reported as an independent risk factor for adverse outcomes in individuals with COVID-19 infection, especially with co-existence of co-morbidities, such as elevated BMI, diabetes, or hypertension. 26 However, even in the absence of co-morbidities, COVID-19 infection itself has been established as a risk factor for higher rates of adverse pregnancy outcomes, including increased risk of thromboembolic disease, hypertensive disorders, preterm birth, SGA size, and Caesarean delivery.49,50,51,52 Our data is similar to that of the Canadian national registry showing livebirths in 1774 (97.4%), stillbirths in 19 (1.0%), prematurity in 228 (12.9%), and SGA size in 127 (10.8%). 52 Thus, ongoing fetal and maternal surveillance is warranted in COVID-recovered pregnant people.
In contrast to earlier reports, vaginal delivery was achieved in most pregnancies, with COVID-19 as a sole indication for Caesarean delivery noted in 11%. It is likely that the higher Caesarean delivery rates in earlier reports represented a cautious approach reflecting a novel pathogen for which outcomes were unknown. With evolving familiarity, it became apparent that vaginal delivery did not confer higher rates of adverse maternal or fetal outcomes than Caesarean delivery, removing COVID-19 infection as a sole indication for Caesarean delivery.53,54
Clinical implications
Despite isolated coagulation abnormalities, the thrombotic nature of COVID-19, and thrombophilic physiologic state of pregnancy, the rates of thrombosis and bleeding among pregnant people from the first wave of the pandemic are low, even in the context of inconsistent thromboprophylaxis.
Research implications
Our report includes pregnancies from the first wave of the pandemic. It is possible that findings from pregnancies complicated by subsequent variants of SARS-CoV2 will differ and comparisons based on data from later waves of the pandemic will be informative.
Strengths and limitations
Our study adds to the sparse reports describing the state of coagulopathy in pregnancies affected by COVID-19. Our definitions of severity reflect the state of knowledge at the time of the first wave of the pandemic, as such severity of illness may be under-represented, as space and resource constraints led to care of sicker patients on lower-acuity wards as the pandemic advanced. Our findings are derived from a retrospective international registry and as such are vulnerable to the limitations inherent in this type of research design, 55 which include lack of random allocation, potentially less robust patient follow-up, and selection bias introduced by missing or incomplete data and by the fact that blood draws are more likely to be completed in sicker individuals. While efforts have been made to include consecutive patients from each participating institution, untested individuals with asymptomatic or mild illness may have been missed. Within those limitations, consideration must be given to the fact that in some conditions, contexts, or populations, studies employing higher-order research designs may not be feasible and that in such circumstances registries serves a valuable function 55 by gathering much-needed data to fill critical knowledge gaps that would otherwise remain unexplored.
Interpretation
Our findings suggest relatively low rates of severe COVID-19 infection and hematological complications such as thrombosis and bleeding among pregnant people. However, we have only included pregnancies from the first wave of the COVID-19 pandemic, and therefore it is possible that pregnancies complicated by subsequent variants of SARS-CoV2 will differ in this regard. The use and duration of thromboprophylaxis on admission and after discharge was inconsistent, though with studies in non-pregnant individuals demonstrating improved outcomes with the use of anticoagulation, there may have been a change in practice in the later waves of the pandemic, which would be worth exploring.
Footnotes
Author contributions
SK, MO, and AKM conceived and designed the study and developed the registry. SK, MO, RK, PSB, JT, EC, LF, MN, RAK, and AKM contributed to the data of the registry. SK and AKM analyzed the results. SK, MO, and AKM drafted the manuscript. RK, PSB, JT, EC, LF, MN, and RAK reviewed and approved the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study has been approved by the ethics board of each participating institution, and patient consent was waived given the retrospective nature of the study and anonymized data.
Guarantor
AKM.