
Abstract

Most healthcare professionals recognize that accurate and inclusive language is fundamental to providing care that is comprehensive and accessible to all. Given that many people who have uteri—such as women, transgender men and non-binary people—can and do carry pregnancies, there is an interest in learning how to incorporate gender-inclusive terminology in obstetrical practice.
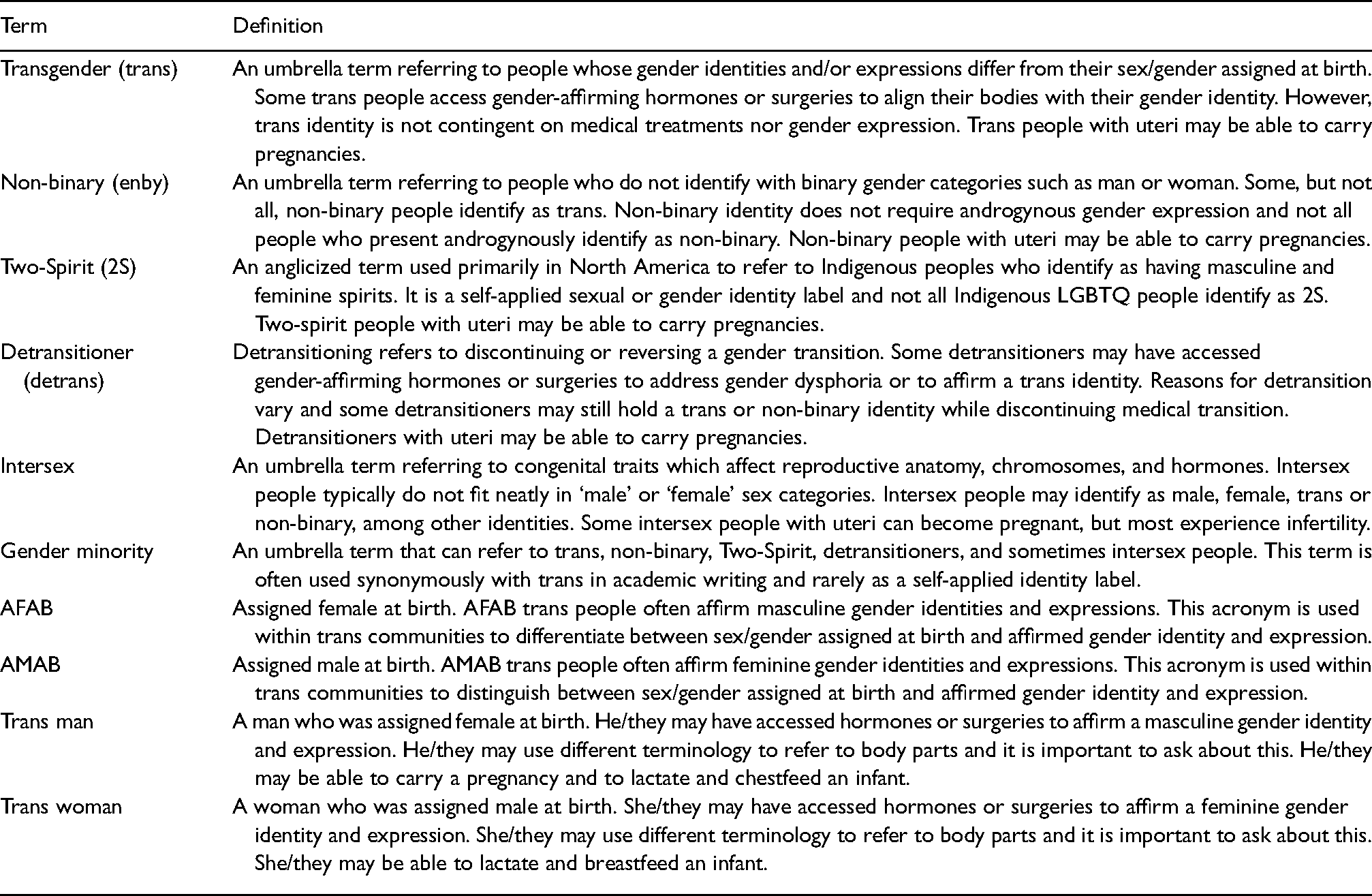
In this invited Editorial, we offer a way forward for the use of language that is inclusive of women, transgender (trans) and other gender minority people in reproductive health (Table 1). Trans is an umbrella term encompassing a diverse range of persons whose internal sense of gender, or the way they express their gender, does not match their sexed bodies. We offer some initial reflections on why it is important to decouple the notions of pregnancy and gender by challenging the assumption that everyone is cisgender (e.g. non-trans).
Terminology.
Gender-inclusive language: An old practice made new again?
Gender-inclusive terms for pregnancy and birthing are not new. Lesbian parents have long distinguished between birth and non-birth mothers, a practice that appears in over a decade of academic literature.1,2 In uncoupling gender from a body's ability to gestate and birth a child, we note that adoptive mothers, cisgender lesbian non-birth mothers and trans mothers who were assigned male at birth (AMAB) all engage in mothering activities and typically identify as mothers. Recognition of these myriad modalities of becoming a mother provides an impetus to develop more precise language for people who require obstetrical services. Further, individuals who might never become mothers – like surrogates or trans people who were assigned female at birth (AFAB) – may nonetheless need obstetrical care.
Obstetric Medicine previously addressed this fraught linguistic terrain with an editorial decision to broadly use the term ‘pregnant woman’ instead of ‘mother’ or the more gender-neutral, if medicalized, ‘pregnant patient’. This decision was justified on the grounds that (1) not all pregnant women give birth, and not all pregnant women are mothers and (2) pregnancy is not an illness. However, the term ‘pregnant woman’ relies on outdated binary gender categories (man/woman) and it excludes from its name some people with uteri who carry pregnancies. More recently, Obstetric Medicine began applying ‘pregnant person’ or ‘pregnant individual’ to most articles – an act of renaming which respectfully responds to evolving knowledge about gender diversity.
Decoupling the notions of pregnancy and gender: Why is it important?
Cisnormativity is the assumption that a person's gender identity matches their sex assigned at birth. In western society, gender is usually categorized into either man or woman and sex characteristics into male or female. This type of binary thinking privileges and normalizes cisgender people. In contrast, trans people's experiences and bodies are made invisible and discounted, which is part of a more subtle and insidious form of transphobia. The assumption of everyone's gender identity matching their sex assigned at birth (cisnormativity) creates an environment of discomfort and systemic prejudice towards trans people. In comparison to cisgender people, trans people are more likely to report unmet healthcare needs 3 and to have their specific care needs erased within cisnormative medical environments. 4 As Sara Ahmed explains, ‘normativity is comfortable for those who can inhabit it’ 5 and uncomfortable for everyone else.
Obstetrical environments are not an easy fit for individuals whose gender identities do not match their sexed bodies. When cisnormativity pervades medicine (e.g. the assumption that only cisgender women give birth), it perpetuates beliefs and practices that centre obstetrical care for cisgender women. Although the majority of pregnancies are carried by cisgender women, the term ‘pregnant woman’ gives pregnancy a gendered characteristic which renders invisible AFAB trans persons with uteri who become or desire to become pregnant. The term ‘pregnant woman’ rests upon cisnormativity, establishing the logic that pregnancy is a bodily function exclusive to cisgender women.
Why adopt language and practices that recognize trans people?
Language affects patient health outcomes. For example, a study which examined 22 AFAB trans people's experiences of pregnancy and chestfeeding indicates that providers’ use of incorrect terminology (e.g. ‘she’, ‘mom’, ‘breasts’) intensifies gender-related psychological distress. 6 Postpartum depression was reported by 35% of this participant sample, suggesting the importance of adopting inclusive language to avoid doing harm. Some trans people delay or discontinue medical transition for the purpose of becoming pregnant, and for some, pregnancy is a pinnacle period of gender dysphoria. 7 Clinicians can avoid compounding the distress experienced by some trans people during pregnancy and birthing by routinely asking about gender identity and appropriate language of those in their care. Having conversations about gender identity and inquiring about the terminology people use to describe their own bodies as a baseline standard of care can help to attenuate pregnant and birthing trans people's healthcare inequities. 8
Pregnant people, birthing people, or patients?
One proposed solution to the problem of the term ‘pregnant women’ is to introduce ‘pregnant men’ and ‘pregnant nonbinary person’ into the obstetrical lexicon. However, an unintended consequence of this decision may result in the amplification of cisnormativity. For example, in 2008, Oprah Winfrey interviewed Thomas Beatie, an AFAB trans man who the mass media then dubbed ‘the first pregnant man’ – despite many who came before him. 9 Winfrey called into question Beatie's status as a man and as a father on the basis of his pregnancy and birthing, and she also interrogated the health of his pregnancy altogether by interviewing his obstetrician. 9 In another example, Freddy McConnell was denied legal recognition as father on his child's birth certificate. According to the UK High Court, by law, he was a ‘mother’ because he had given birth. 10 In both cases, the ‘biological fact’ of pregnancy and birthing were leveraged to discredit Beatie's and McConnell's gender identities. Classifying pregnant people as pregnant women, pregnant men and pregnant non-binary people unintentionally promotes cisnormative social and legal preconceptions.
At present, ‘pregnant people’ and ‘birthing people’ provide a neutral ground to pause and recognize gender-inclusive descriptors in obstetrics. Open-ended names provide clarity without excessive verbosity and inclusivity without binary gender. In some clinical obstetrics cases, additional medical signifiers such as ‘patient’ may be appropriate. For instance, when caring for people with chronic kidney disease who are pregnant, ‘pregnant patient’ denotes a medicalized component of a pregnancy while avoiding the erasure of trans people. 11 However, in the absence of relevant intercurrent disease, referring to pregnant people rather than pregnant women or mothers ensures that no one's core gender identity or pregnancy/birthing experience is devalued by scholarly discussions of obstetric medicine.
Some might object that this nomenclature favours inclusivity over the experiences of the majority of pregnant people who are cisgender women, and that we should instead be centring the experiences of these women. However, the term ‘pregnant person’ does not discredit cisgender women; rather it opens the umbrella to cover everyone seeking obstetrical care. Language evolves, and words matter. Providing comprehensive and accessible healthcare to all includes broadening gender-neutral and affirming language in obstetrics.
While trans people still experience stigma and poor health outcomes owing largely to cisnormativity, the medical community has moved past some of its more egregious historical practices. For example, physician gatekeepers used to judge whether trans patients were ‘truly’ trans by their willingness to abandon their children in order to medically transition. 12 Thankfully, trans people no longer have to leave their families to receive gender-affirming hormones or surgery. Responding to such past harms done to trans people by using gender-inclusive language extends an olive branch from the medical community to this often-stigmatized population, signalling an act of reconciliation. It also demonstrates respect for an evolving gender classificatory system and awareness of changing clinical practices. Caring about, and for, people's health, including their reproductive health, must include thoughtful renaming practices that promote inclusion and the search for words of recognition and respect.
Footnotes
Acknowledgements
The authors would like to thank the editors, Drs. Stephen Lapinsky and Charlotte Frise, as well as the peer reviewers, for providing feedback and guidance.
Informed consent
Informed consent was not required as this writing did not involve original research or human subjects.
Ethical approval
N/A. Research ethics board approval was not required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Guaranteed author
Kinnon R. MacKinnon is guarantor of the present work.