
Abstract
Carotid webs are intraluminal shelf-like projections caused by thickening of the arterial tunica intima. Due to their projections forming a nidus for thrombus formation and subsequent embolus, they are considered to be a rare cause of ischaemic strokes. We report a case of a woman with a background of recurrent ischaemic strokes due to bilateral carotid webs who presented with a twin pregnancy. We use this case to discuss how her pregnancy-related stroke risk was subsequently medically managed.
Keywords
Background
The incidence of stroke in pregnancy worldwide has been reported to be 30 per 100,000 pregnancies, roughly three times higher than the incidence of stroke in young adults. 1 Risk is seemingly greatest in the peripartum period. 2 Mortality associated with pregnancy-related stroke has been reported at 10% and for those that do survive, subsequent disabilities can have a devastating impact on young women and their families. 3 It is therefore vital that clinicians can effectively investigate and manage stroke risk factors. When common causes of ischaemic stroke have been excluded, rarer causes should be considered. Carotid webs are intraluminal shelf-like projections that arise at the carotid bulb caused by thickening of the arterial tunica intima. They are considered to be a variant of fibromuscular dysplasia and due to their projections forming a nidus for thrombus formation and subsequent embolus, they are considered to be a rare cause of ischaemic strokes. 4 Prevalence has been reported at 1–2% 5 but has been reported to be as high as 21.2% in those investigated for a cryptogenic stroke. 6 They occur more commonly in females6,7 and although genetic predisposition and hormonal influences have been suggested, their exact cause is unknown. The presence of carotid webs and the impact these may have on stroke risk during pregnancy is unknown. 8
In this case report we discuss the case of a woman who presented with recurrent ischaemic events and was ultimately diagnosed with bilateral carotid artery webs. We discuss the therapeutic management of this condition in the context of the patient's subsequent twin pregnancy.
Case presentation
A 39-year-old mother of two with a past medical history of migraines (with aura), Raynaud's phenomenon, eczema and recently diagnosed recurrent ischaemic strokes was re-referred to stroke services as she was newly pregnant with twins. There was no history of concerning neurological symptoms during her first two pregnancies.
She had first presented approximately 5 years earlier after a 30-min episode of onset left upper limb weakness, slurred speech and left-sided blurred vision. Subsequent examination, blood tests, electrocardiogram (ECG), carotid Doppler and plain computerised tomography (CT) were normal and the episode was attributed to a hemiplegic migraine. She continued to suffer with similar intermittent neurological episodes (presenting with limb weakness, dysarthria and facial droop), which were diagnosed as recurrence of hemiplegic migraines, during the next 5 years. Due to the prolonged history of recurrent headaches, outpatient magnetic resonance scan (MRI) was then undertaken which demonstrated the presence of an old right-frontal insular infarct. Bubble contrast echocardiogram, transthoracic echocardiogram, 24-h heart tape and carotid Doppler were requested. All were unremarkable and she was commenced on 75 mg of aspirin daily.
A few months later, she presented again having woken from sleep with left-sided arm and leg weakness (lasting approximately 2.5 hrs). Immediate CT head scan demonstrated a new infarction in the right basal ganglia. A CT angiogram identified bilateral vascular webs. She continued to smoke 10 cigarettes per day and was converted to dual antiplatelet therapy with 75 mg of aspirin and 75 mg of clopidogrel. Her resultant anti-nuclear cytoplasmic antibody, anticardiolipin and erythrocyte sedimentation rate (ESR) tests were negative and repeat MRI confirmed the sub-acute right cortical and right basal ganglia infarcts.
She became pregnant with twins within 6 months of her most recent infarct.
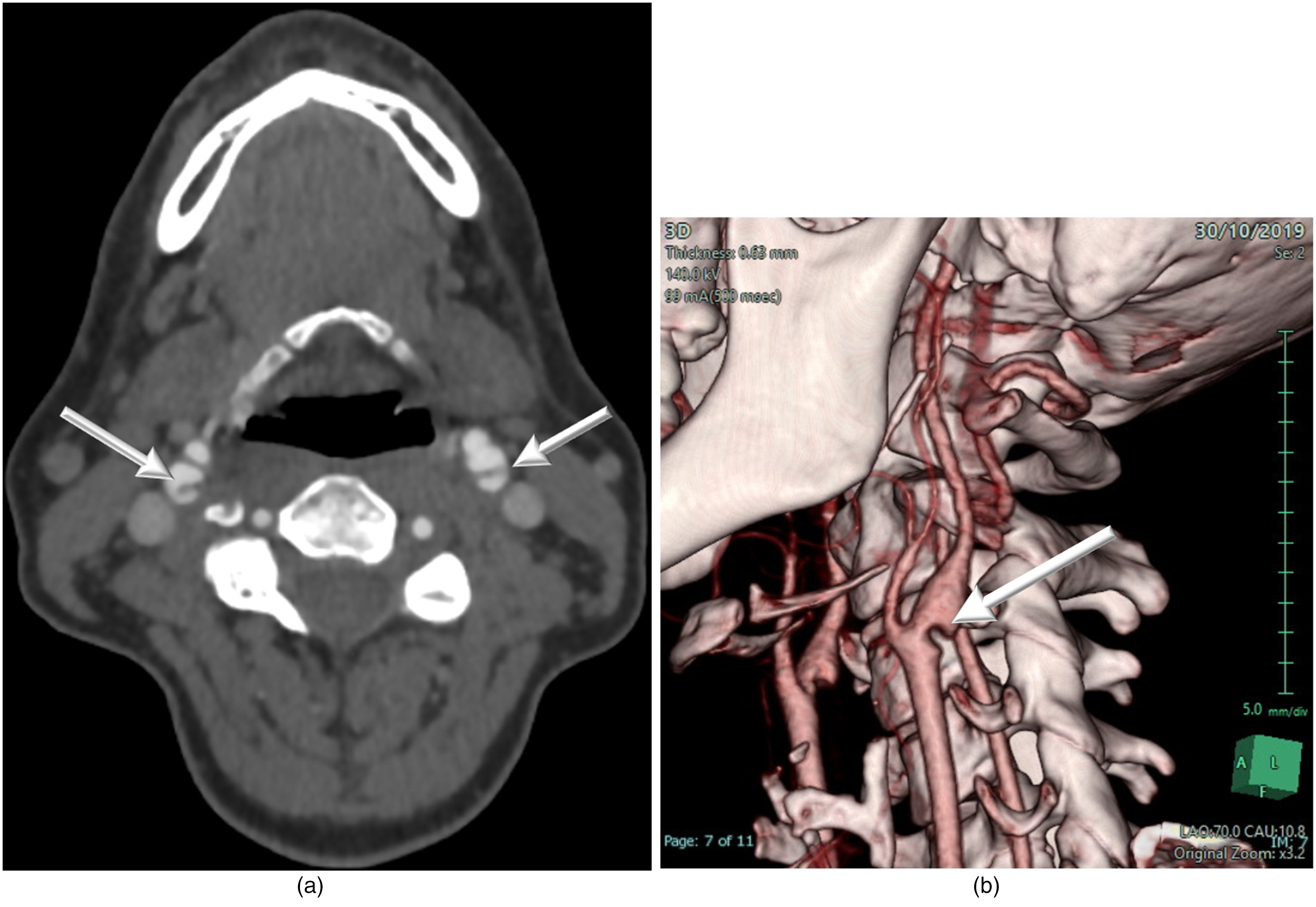
(a) CT angiogram demonstrating both internal carotid webs (arrows). (b) 3D reconstruction showing left carotid web (arrow).
Treatment
There was concern that as she had already suffered a recurrent ischaemic stroke while taking a single antiplatelet therapy, the risk of further ischaemic events in the hypercoaguable setting of a twin pregnancy was increased even further. Following consultation with the patient and the wider multidisciplinary team, it was decided that she remain on dual antiplatelet therapy (DAPT) throughout early pregnancy. Due to concerns regarding post-partum haemorrhage caused by clopidogrel, her treatment was temporarily converted to prophylactic dose low molecular weight heparin in the late third trimester and for 6 weeks following delivery. She did not suffer from any neurological deficits during her pregnancy.
At 37 weeks of gestation she underwent a caesarean section, under spinal anaesthesia, for failure to progress in labour. Her twins were born in good condition, with birthweights of 2.4kg and 2.5kg.
This woman has not suffered any further ischaemic events in the 4 years since starting DAPT. She remains on long-term DAPT.
Discussion
There is generally a lack of robust evidence around the management of stroke in pregnancy with the majority of evidence being based on case reports and retrospective studies. This is partially due to a paucity of evidence regarding the cause of ischaemic strokes in the young. Even for conditions that are known triggers (such as arterial dissection, Factor V Leiden, Protein C or S deficiencies or autoimmune diseases) very little clinical data is currently available. 9 Current advice supports this use of thrombolysis and thrombectomy if indicated in moderate-to-severe ischaemic stroke. 10
For secondary prevention, there is a lack of clear guidance on the safety of antiplatelets. Aspirin has been shown to be safe in pregnancy at lower doses but the safety of high-dose aspirin has not been clearly demonstrated. Clopidogrel can also be used but the use of DAPT is not standard management due to the risk of bleeding. 11
There is no specific guidance for the management of carotid artery webs, especially in the context of pregnancy. Pharmacological or surgical management options with antiplatelets and carotid endartectomy/stenting, 6 respectively, are traditionally utilised but no definitive trial has been undertaken to demonstrate the superiority of either option. Similarly, the superiority of single agent therapy versus DAPT has not been definitively demonstrated but there is an apparent increased risk of stroke when antiplatelets are discontinued. 6
In this case, investigation of the cause was vital to minimize the further risk of stroke. Generally in pregnancy-related stroke, the risk in future pregnancies is low but can be much higher in some causes such as antiphospholipid syndrome. 11 In comparison, other common causes of ischaemic strokes in the young (such as traumatic arterial dissection/illicit drug use) may not confer increased risk if the primary trigger is not repeated. Accurate diagnosis makes it possible to commence suitable secondary prevention, although clearer guidance for optimal management is required.
Footnotes
Acknowledgements
We would like to thank the patient for allowing us to write about her case.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Written consent has been obtained from the patient.
Author contributions
All authors have contributed to the writing of this case report. All authors have also read the manuscript and have agreed to its submission.