
Abstract
Objective
To assess the uptake of postnatal oral glucose tolerance test and to determine the sensitivity of fasting postnatal blood sugar in predicting 2-h impaired glucose tolerance.
Methods
Retrospective study of 1961 women diagnosed with gestational diabetes mellitus. All women were offered oral glucose tolerance test six weeks post-delivery.
Results
Of 1961 women, 1090 (56%) returned for postpartum oral glucose tolerance test. A fasting plasma glucose of ≥6.1 mmol/l identified only 76 of 167 women with impaired glucose tolerance detected by a 2-h oral glucose tolerance test (sensitivity of 45.5%; 95%CI: 38.1–53.1). We observed a normal fasting glucose but an impaired 2-h glucose tolerance in 91 out of 968 (9.4%) women. Asian ethnicity, admission on special care baby unit and antenatal insulin therapy strongly predicted 2-h impaired postnatal blood glucose levels (P < 0.05).
Conclusion
Although fasting plasma glucose is a convenient method, it lacks sensitivity in identifying women with impaired glucose tolerance postnatally.
Keywords
Introduction
Gestational diabetes (GDM) is defined as glucose intolerance that is diagnosed for the first time in pregnancy 1 and affects 4% of pregnant women. 2 With the growing concerns regarding rising body mass index (BMI) and increased maternal age among women becoming pregnant, the prevalence of GDM is expected to rise.3,4
Diabetes in pregnancy is associated with risks to the woman and to the developing fetus;4–6 therefore, early recognition and treatment of this is likely to have benefits for the maintenance of both short- and long-term health for mother and the fetus.6,7 Women with a history of GDM have at least a seven-fold increased risk of developing type 2 diabetes in future compared with women who have normoglycaemic pregnancies.1,3,8 This is a growing public health concern associated with a number of serious health complications that reduce both the life-expectancy and quality of life of those who suffer.1,9 There is good evidence to suggest that intensive lifestyle interventions can reduce type 2 diabetes in high-risk individuals.1,3,4 Thus, a diagnosis of GDM represents a window of opportunity for implementing these interventions. 1
Postpartum glucose testing six weeks after delivery is recommended for women diagnosed with GDM to identify those at risk of developing type 2 diabetes, so that timely intervention and preconception care in subsequent pregnancies can be provided.10–12 Despite this evidence, uptake of postnatal testing for diabetes is poor.10,13 Furthermore, there is inconsistent and limited information on what constitutes the optimal screening method for identifying women at risk of diabetes.11,14
This study aimed to (a) assess the uptake of postnatal glucose testing (b) determine the sensitivity of fasting postnatal blood sugar in predicting 2-h impaired glucose tolerance (IGT) and (c) identify the strength of association of maternal demographics and pregnancy-related factors with future risk of diabetes in women with GDM.
Material and methods
We performed a retrospective analysis on all women diagnosed with GDM at the Jessop Wing Hospital, Sheffield between January 1990 and December 2015. The study was undertaken to determine the sensitivity of fasting postnatal blood sugar in predicting 2-h IGT and to assess whether maternal, demographics, antenatal, intrapartum, postpartum or neonatal variables can identify women with postnatal IGT. All women with type 2 diabetes were excluded from the study.
Women at risk of developing GDM were selectively screened with an oral glucose tolerance test (OGTT) at 24–28 weeks of gestation and were defined as having GDM if they fulfilled the World Health Organization (WHO) criteria for impaired fasting glucose (fasting plasma glucose ≥6.1 mmol/l) and/or IGT (2-h post challenge plasma glucose ≥7.8 mmol/l). 15 Using these criteria, women diagnosed with GDM attended a combined Obstetric endocrine clinic for intensive medical and obstetric management.
All women with GDM were recommended to have a 75 g OGTT six weeks postpartum to confirm their glucose tolerance status. 12 Women were advised about the postpartum OGTT and an appointment was made before hospital discharge. All women and their general practitioners were notified of the result by letter.
Data for this retrospective review were retrieved from the clinical database maintained within Jessop Wing Maternity Unit, Sheffield.
Statistical analysis
The diagnostic accuracy of postpartum fasting blood glucose for predicting postnatal 2-h IGT was evaluated using sensitivity and specificity. The relationship between demographic, antenatal, intrapartum and postnatal factors for predicting normal fasting blood glucose and impaired 2-h blood glucose, compared to normal fasting blood glucose and normal 2-h blood glucose, was assessed using logistic regression model and results presented as odds ratios (OR) and 95% confidence intervals (CI). Univariable models were first applied to examine the relationship between individual variables and the development of the outcome of interest (2-h IGT result). Stepwise multivariable logistic regression was used to identify variables that were statistically significant predictors of the outcome of interest. Differences between women who did and did not return for postpartum glucose testing were compared using independent samples t-test for continuous variables and chi-square tests for categorical variables. All analyses were conducted using SPSS (IBM SPSS Statistics for Windows, Version 21.0, Armonk, NY).
Results
Demographic characteristics of women, labour and birth.

OGTT: oral glucose tolerance test; SCBU: special care baby unit; BMI: body mass index; SD: standard deviation.
The mean age of the women was 31.6 years (SD ± 6.1). Sixty-one per cent were Caucasians and 28% Asian. Antenatal insulin was commenced in 23% of our population. Mean birth weight was 3.3 kg (SD ± 0.6) and 81% of the babies required admission on special care baby unit (SCBU). The main reason for SCBU admission was for the stabilisation of blood sugar levels.
Characteristics of the women stratified by whether they returned for postpartum glucose testing.
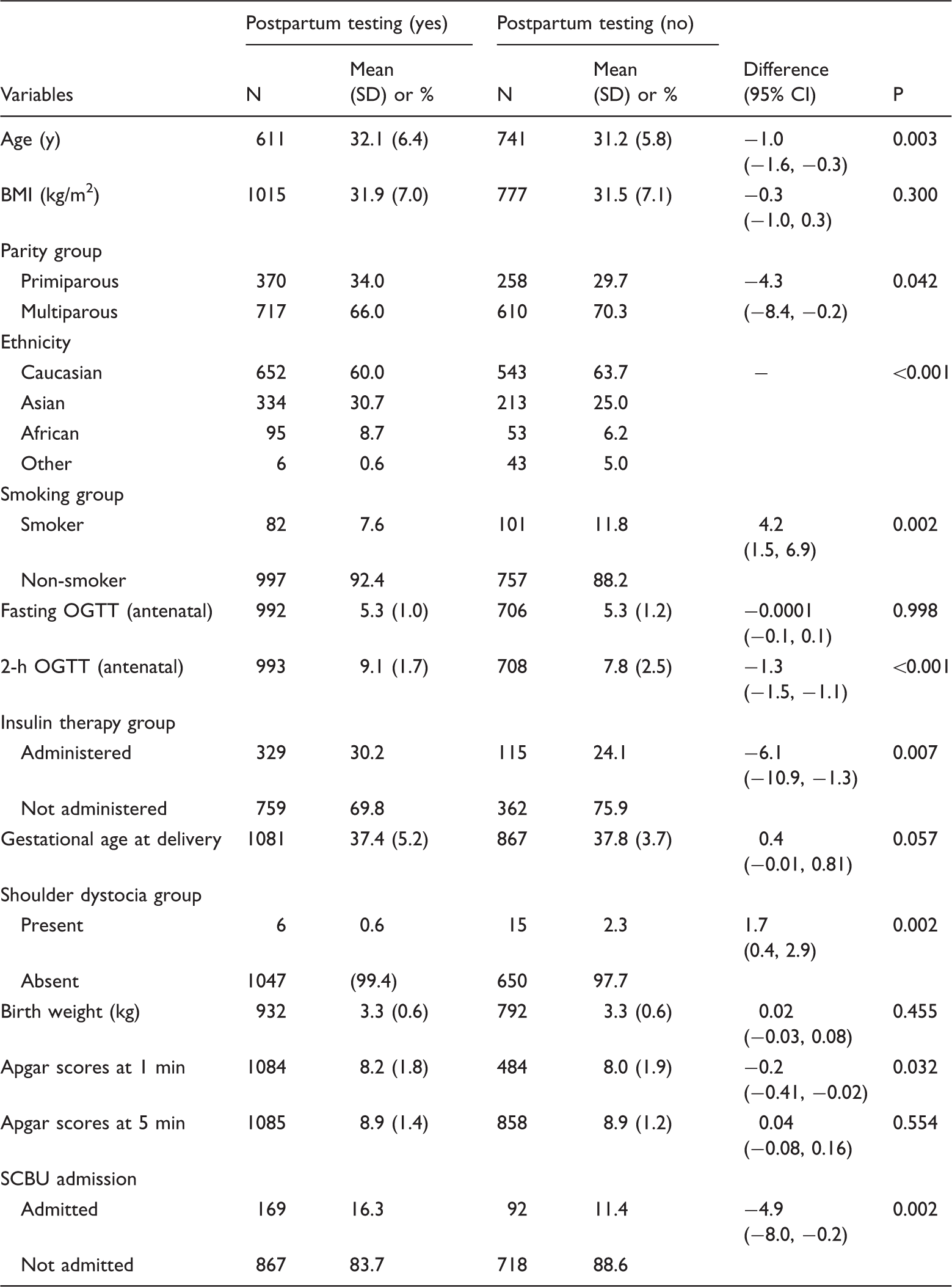
OGTT: oral glucose tolerance test; SCBU: special care baby unit; BMI: body mass index; SD: standard deviation.
Women who returned for postpartum OGTT were predominantly nulliparous, slightly older, of Asian ethnicity, had higher 2-h blood sugars at the diagnosis of GDM, required insulin to treat their GDM, encountered shoulder dystocia at the time of delivery and their babies required admission on SCBU (P < 0.05).
Comparison of fasting blood glucose results and 2-h blood glucose results for identifying impaired glucose tolerance.
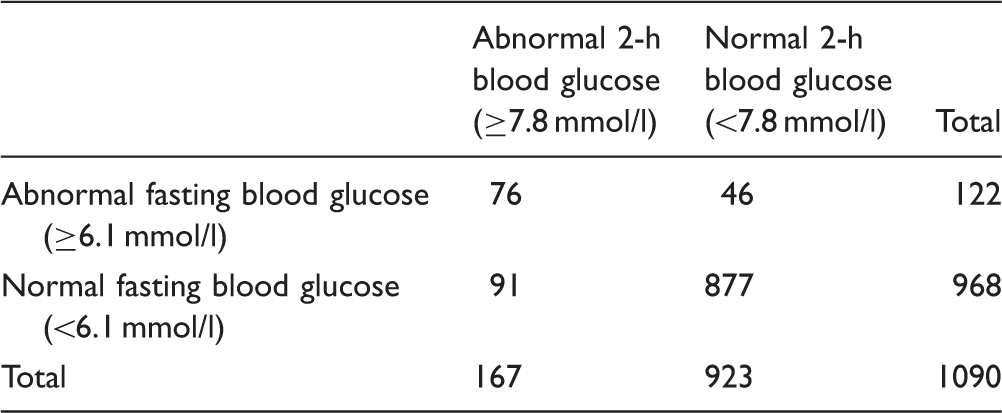
Although a normal postpartum fasting plasma glucose (<6.1 mmol/l) correctly identified normal 2-h glucose tolerance in 877 of 923 (specificity of 95.0%; 95%CI: 93.4–96.2), a fasting plasma glucose of ≥6.1 mmol/l identified only 76 of 167 cases with impaired 2-h glucose tolerance (sensitivity of 45.5%; 95%CI: 38.1–53.1). Of the 1090 postnatal OGTTs that were performed, 167 women were diagnosed with IGT based on raised 2-h plasma glucose level (≥7.8 mmol/l) giving an incidence of 15.3%, and 122 were diagnosed with IGT based on raised fasting plasma glucose (≥6.1 mmol/l), giving an incidence of 11.2%. We observed normal fasting but impaired 2-h blood glucose in 91 out of 968 women (9.4%).
Odds ratios of normal fasting blood glucose but impaired or abnormal 2-h blood glucose compared to normal fasting blood glucose and normal 2-h blood glucose from univariable logistic regression models.

OGTT: oral glucose tolerance test; SCBU: special care baby unit; BMI: body mass index.
Odds ratio for a one unit increase.
Women from Asian ethnicity were at a 1.5 times higher risk of impaired 2-h glucose tolerance compared to Caucasians (OR: 1.58; 95% CI: 1.01–2.49). Those who required insulin therapy to manage GDM demonstrated strong association with IGT compared to those who did not require insulin treatment (OR: 3.08; 95% CI: 1.98–4.78). Women whose babies required admission to SCBU more often exhibited impaired blood glucose compared to those who did not require SCBU admission (OR: 2.01; 95% CI: 1.17–3.44). However, when multivariable analysis was conducted, only the use of insulin remained a significant predictor for IGT for women with GDM.
Discussion
Our study revealed two principal findings. Firstly, postnatal fasting plasma glucose was not sensitive enough to identify women with IGT. Secondly, women diagnosed with GDM from an Asian background, requiring insulin therapy during pregnancy and whose babies required admission on SCBU were at higher risk of developing IGT postnatally.
In addition to the above findings, we observed higher attendance rates for postpartum screening among older women, those within the Asian population and those who had high blood sugar levels and required insulin treatment during pregnancy.
The optimal method of testing to determine whether a woman’s glucose tolerance has returned to normal remains a subject of some debate. 7 The American diabetes association, 16 the Fifth International Workshop Conference on Gestational Diabetes 17 and the Canadian Diabetes association 18 recommend postnatal OGTT. However, recent UK guidance published by the National Institute for Clinical Excellence 5 recommends fasting plasma glucose alone. Our data show that in our population, a significant proportion of cases with IGT would be missed by a postpartum screening policy based on fasting plasma glucose alone. Although fasting plasma glucose has greater reproducibility compared with an OGTT, it lacks sensitivity in identifying women with IGT and type 2 diabetes.11,19 Kitzmiller et al. 9 reported that among 527 women with GDM, fasting plasma glucose lacked the sensitivity (34%) to identify IGT and type 2 diabetes in the postpartum OGTTs performed. Similar observations were made by Kim and coworkers, 11 Hunt and Conway 20 and McClean et al. 7 Our own findings are in agreement with these conclusions and highlight the potential of missing women at risk of diabetes. Therefore, the greater convenience of utilising fasting blood glucose needs to be weighed carefully against its decreased sensitivity, particularly among women requiring insulin therapy in pregnancy.
The strength of the current study is that it includes a relatively large number of postpartum women with a history of GDM. The study cohort was of sufficient size to evaluate the relative importance of multiple clinical risk factors related to the mother, pregnancy and the neonate for predicting postpartum diabetes. This study also identified admission on the neonatal unit as a strong predictor of IGT, not previously seen in other studies.
The future risk of diabetes appears to be mainly associated with gestational glycaemic status and not with the mother’s weight or the baby’s birth weight. Based on multivariable analysis, we found that women who require insulin treatment during pregnancy are more likely to develop IGT. This is in agreement with the results of previous studies.8,13 In contrast to other studies, we did not find an association between: maternal-age, BMI, multiparity, increased levels of either fasting or 2-h blood glucose during pregnancy, birth weight or fetal macrosomia and the development of IGT.8,9,13
The significant association between Asian ethnicity and IGT is striking. In the Asian population, fasting blood glucose has much lower sensitivity than postprandial glucose concentration for the detection of diabetes, 21 implying that it is possible that detection of IGT in substantial number of these patients would be missed if routine OGTT was not undertaken for this study cohort. Curtailing the rapidly increasing prevalence of young-onset diabetes in Asian countries is a pressing task for healthcare practitioners. 21 More effort is needed to identify these young women as early as possible, because they are one of the best groups for effective implementation of primary prevention not only for themselves but also for their offspring and family.
Postpartum glucose testing is an important first step in an attempt to prevent both recurrence of GDM and the development of type 2 diabetes. 22 It is clear from many studies that there is a high rate of non-attendance for postpartum follow-up, 23 and the lack of clear communication between secondary and primary care providers to arrange follow-up has been reported.13,24 Compliance with postpartum glucose screening and long-term follow-up is low because of the poor perception by women with GDM of the risk that they have of developing type 2 diabetes. 25 The uptake of postnatal testing in our population was 56% which is comparable to that observed in a randomised controlled trial by Clark et al. 26 in which the response rate was 60.5%, when both patient and doctors received reminders. We observed higher attendance rates for postpartum screening among older women, those within the Asian population and those who had high blood sugar levels and required insulin treatment during pregnancy. Although the reasons are speculative, it is possible that healthcare providers may have stressed the importance of postpartum screening among these women, given their high prevalence of diabetes. 27
The database from which the material for this report was collated was designed to ensure that all women were offered a follow-up appointment and to identify and make contact with those who did not attend an initial appointment. Poor attendance at postpartum screening was observed in women of higher parity. In order to further improve postpartum screening performance, reminders should be introduced into regular practice. 28 If there is lack of response to automated, live or recorded telephone or e-mail messages to patients and their doctors, an effort should be made to directly contact the patient, i.e. via a home visit by a healthcare worker. 21 Communication between hospitals and general practitioners on the mother’s risk of future diabetes could be improved by providing discharge summaries with pregnancy-specific risk factors associated with an increased risk of IGT, such as insulin administration, admission of baby on the neonatal unit and OGTT results. An additional benefit of this summary is to raise the awareness of the individual risk factors as women have been shown to be more likely to comply with diet and lifestyle changes if they know their individual risk of future diabetes. 13 The implications of preventing impending diabetes are profound in terms of cost savings for the individuals and the healthcare system, if significant numbers of these high-risk women can avoid development of diabetes until much later in life.
We acknowledge the inherent limitations in a retrospective analysis, including the inability to control data quality. Participants for the study were identified from medical records; therefore, documentation and record keeping were inconsistent across time and clinicians. An additional limitation was the inability to assess the occurrence of postpartum glucose testing among 36% of women diagnosed with GDM. Although we examined clinical factors and their relationship to assess whether a woman returned for postpartum glucose screening, we were not able to obtain information directly addressing why women did not turn up for postpartum screening. In order to improve our ability to screen women postpartum, it would be pertinent to examine and acquire information on sociocultural status.
We found that women with GDM who require insulin therapy during pregnancy have substantial risk of IGT, best identified by a 75-g 2-h OGTT six weeks postpartum. Performance of fasting blood glucose as opposed to the OGTT will miss a subpopulation of women at risk. The identification of women with IGT is of special importance, since IGT has a higher sensitivity than impaired fasting blood glucose for predicting the progression to type 2 diabetes. 29 Moreover, since IGT reflects postprandial hyperglycaemia, it may predict a greater cardiovascular risk, implying that OGTT may be more predictive than fasting plasma glucose for future cardiovascular disease. 30
Diagnosing IGT in women after GDM is important to reduce the risk of poor glycaemic control at the conception of any subsequent pregnancy, thereby reducing the risk of fetal abnormalities and other birth complications. 2 Pregnancy is an important point in the life of woman when she has regular contact with the healthcare system, thus providing opportunities to influence the future health of both mother and child. 13 Therefore, every effort should be made to recall women who had GDM, in order to improve testing rates in this high-risk population and reduce the number of missed opportunities to diagnose diabetes.
We recommend that in population where the risk of persistent diabetes after pregnancy is high, in particular women who require insulin treatment during pregnancy, routine postpartum OGTT should be employed to ensure early detection and appropriate treatment of abnormal glucose levels to reduce long-term impact of diabetes on woman’s health. Healthcare providers could use this information to warn these women and increase their perceived susceptibility and threat of type 2 diabetes. This information can help in counselling patients regarding their individual risk while they are still pregnant, highly motivated and under frequent medical care. Introducing this concept during pregnancy, especially to those at greatest risk of type 2 diabetes, will improve medical follow-up after delivery and reduce the burden of diabetes especially in women at risk of young-onset diabetes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted as a service evaluation project so formal ethical approval was not required.
Guarantor
HK.
Contributorship
All authors contributed significantly to the manuscript and approved the final version. Dr Habiba Kapaya contributed to the concept and design and drafted the report. Dr Lucy May participated in acquiring the data and drafted the article. Dr Richard Jacques analysed and interpreted the data and drafted the report. Dr Priya Madhuvrata contributed to the concept and design and revised the manuscript critically for important intellectual content.