
Abstract
Background:
Subglottic cysts (SGCs) are a rare disease with a high misdiagnosis rate.
Objectives:
We aim to improve the diagnostic and management ability of pediatricians for SGCs by analyzing the clinical characteristics of confirmed cases.
Design:
Observational, retrospective cohort study
Methods:
We enrolled children diagnosed with SGCs admitted to the Children’s Hospital of Chongqing Medical University between January 2010 and December 2022. Clinical characteristics data were collected and analyzed retrospectively. Patients were regularly followed up for 1 year post-treatment or discharge.
Results:
Eleven children were included in this retrospective study. There were nine (9/11, 81.8%) males and two (2/11, 18.2%) females, and the median age was 15 months. Eight (72.7%) were premature. Seven (63.6%) patients had a history of intubation. The common manifestations were stridor (72.7%), wet cough (72.7%), shortness of breath (72.7%), and dyspnea (54.5%). The average diagnosis time was 7 months. The most common comorbidity was laryngopharyngeal reflux disease (LPRD, 45.5%), followed by laryngomalacia (27.3%), bronchopulmonary dysplasia (27.3%), bronchial stenosis (18.2%), and adenoid hypertrophy ( 18.2%). The obstruction degree of SGCs was “3” (51%–75% occlusion) or higher in eight (72.7%) patients. Two (18.2%) patients experienced recurrence after initial cyst aspiration and subsequently underwent successful laryngoscopy marsupialization. Ultimately, eight (72.7%) patients achieved complete recovery after endoscopic marsupialization.
Conclusion:
SGCs should be considered in the differential diagnosis of children, especially those with a history of prematurity and/or perinatal intubation, who present with stridor, wet cough, and respiratory distress. Endoscopic evaluation is crucial for both definitive diagnosis and guiding effective treatment.
Introduction
Subglottic cysts (SGCs) are a rare but significant benign cause of upper airway obstruction in children. The clinical presentation of SGCs is highly variable, ranging from asymptomatic to stridor, respiratory distress, apneic episodes, recurrent croup, and failure to thrive due to chronic subglottic airway obstruction.1–9 Owing to this lack of specific clinical manifestations, SGCs are frequently misdiagnosed as more common conditions such as laryngomalacia, subglottic stenosis in clinical practice,5,10 potentially leading to inappropriate treatment. Delayed diagnosis and treatment of SGCs may increase clinical and financial burden. Physicians, especially pediatricians, should be aware of this condition as patients usually visit them first.
Flexible or rigid endoscopy plays a pivotal role in the contemporary management of SGCs, as it allows for both definitive diagnosis by direct visualization and accurate assessment of the lesion’s characteristics.2,4,5,10,11 Furthermore, endoscopy provides a therapeutic avenue. Endoscopic marsupialization is regarded as the gold standard treatment for symptomatic SGCs.2,4,5,11 However, achieving long-term control can be challenging. Previous studies have indicated that the recurrence rate following endoscopic intervention ranges ranging from 25% to 70%,1,12 highlighting the need for technical precision and perhaps adjunctive strategies. Therefore, we retrospectively enrolled children with SGCs admitted to our hospital from January 2010 to December 2022 to analyze the clinical features to enhance the understanding of SGCs, improve early diagnosis and intervention, ultimately reducing the rate of clinical misdiagnosis and improving patient care.
Methods
Study design
This observational cohort study was conducted at the Children’s Hospital of Chongqing Medical University. Children diagnosed with subglottic cysts hospitalized between January 1, 2010, and December 31, 2022, were enrolled retrospectively. This study was approved by the Children’s Hospital of Chongqing Medical University research committee(s) (File No. (2022)128). Patient consent was waived due to the retrospective nature of the study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 13
Inclusion and exclusion criteria
The inclusion criteria were all of the following: (1) inpatients; (2) younger than 18 years old; (3) presence of at least one of the following symptoms: stridor, cough, shortness of breath or inspiratory retractions; (4) SGCs confirmed by enhanced computed tomography, bronchoscopy, laryngoscopy, or surgery2,3,7; and (5) with complete medical records.
Exclusion criteria included any of the following: (1) non-subglottic cysts (e.g., saccular cysts, laryngeal cysts, and subglottic haemangioma) and (2) incomplete medical records.
Data collection
The following parameters were recorded: demographic data, gestational age at birth, intubation history and duration, clinical symptoms, the morphological classification of SGCs, treatment, complication rates, recurrence(s) of cysts following initial management, and duration of follow-up.
The morphological classification criteria for pediatric central airway stenosis are as follows 14 :
Stenosis position: “1” represents the subglottic stenosis, “2” represents tracheal stenosis, “3” represents carinal stenosis, “4” represents bilateral main bronchial stenosis, and “5’”represents unilateral main bronchial stenosis;
Stenosis type: “1” denotes intraluminal growth, “2” represents extrinsic compression, “3” represents scar/stricture, “4” represents distortion, “5” represents floppy membrane, and “6” represents airway malacia;
Stenosis degree: “1” signifies⩽25%, “2” signifies 26~50%, “3” signifies 51~75%, “4” signifies 76%~90%, “5” signifies>90%,nearly completely occluded, “6” signifies complete obstruction;
Stenosis lengths: “1” indicates <1 cm, “2” indicates 1~3 cm, “3” indicates 3~5 cm, “4”’ indicates >5 cm.
Surgical or intervention techniques
All patients underwent laryngoscopy and/or bronchoscopy to evaluate the SGCs accurately. Endoscopic cyst excision was undertaken in those cases where significant improvement in the subglottic airway could be achieved. 4 Marsupialization was performed using a laser or cold steel microinstruments.2,4 Cryotherapy was administered when a notable volume of inflammatory tissue remained after marsupialization.
Outcome measures
Patients were regularly followed up at 1 week, 1–3 months, 3–6 months, and 6–12 months post-treatment/discharge, in accordance with standard medical practice. Follow-up included assessment of respiratory symptoms. Repeat laryngoscopy or bronchoscopy was performed for patients with recurrent symptoms. Recurrence was defined as the detection of a cyst at the previous excision site upon repeat laryngoscopy or bronchoscopy re-evaluation. 2 Complete recovery was defined as the absence of cysts on endoscopy and the resolution of all symptoms during the follow-up period. 2
Statistical analysis
Statistical analyses were performed using R software (version 4.3.0, R Core Team, 2023). Categorical data between groups (e.g., with vs without LPRD, with vs without intubation history) were compared using Fisher’s exact test. Continuous data were compared using the Student’s t-test or the Wilcoxon rank-sum test, as appropriate. A p-value of < 0.05 was considered statistically significant.
Results
A total of 48,321 bronchoscopies and 9197 laryngoscopies were performed on inpatients during the study period. Among these, 11 cases of SGCs were confirmed, yielding a detection rate of 0.2‰. The cohort consisted of nine (81.8%) males and two (18.2%) females. The median age was 15.0 (IQR, 30.3) months, with seven patients (63.6%) aged 0–3 years and three (27.3%) aged 3–6 years. The median time from symptom onset to diagnosis was 7 months.
An analysis comparing patients with (n = 7) and without (n = 4) a history of intubation revealed that the non-intubated group was significantly older at diagnosis (median age: 56.2 vs 10.4 months, p = 0.0726), although this difference did not reach formal statistical significance, likely due to the small sample size.
Subglottic cysts were most commonly located on the left lateral wall. Solitary cysts were observed in nine (81.8%) patients, while two (18.2%) had multiple cysts. Eight (72.7%) patients were premature. Seven (63.6%) had a history of intubation, with durations ranging from 6 to 45 days. The diagnosis of SGCs was confirmed from 5 to 44 months post-extubation. The most prevalent comorbidity was laryngopharyngeal reflux disease (LPRD, 45.5%), followed by laryngomalacia (27.3%), bronchopulmonary dysplasia (BPD) (27.3%), bronchial stenosis (18.2%), and adenoid hypertrophy (18.2%; Table 1). Before treatment, patients exhibited various respiratory symptoms. The most common presenting symptoms were stridor (72.7%), wet cough (72.7%), shortness of breath (72.7%), and dyspnea (54.5%). Other symptoms included hoarseness (45.5%), growth retardation (36.4%), feeding difficulties (27.3%), and pharyngeal pruritus (18.2%) (Table 1). No significant differences in clinical manifestations were found between patients with and without LPRD or between those with and without an intubation history (Tables 1 and 2).
Clinical features of SGCs in 11 children with or without laryngeal reflux disease.

Wilcoxon rank-sum test.
BPD, bronchopulmonary dysplasia; m, months; SGCS, Subglottic cystic stenosis.
Clinical features of SGCs in 11 children with or without intubation history.
Wilcoxon rank-sum test.
BPD, bronchopulmonary dysplasia; LRD, laryngopharyngeal reflux disease; m, months; SGCS, Subglottic cystic stenosis.
Different types of SGCs are detailed in Figure 1. According to the morphological classification, the stenosis degree was “3” or higher in eight patients (72.7%). Five patients (45.5%) underwent laryngoscopic marsupialization. Two patients (18.2%) who initially underwent cyst aspiration experienced recurrence within 2–3 months and were successfully treated with subsequent laryngoscopy marsupialization. One patient (9.1%) was treated via flexible bronchoscopy using a holmium laser combined with cryotherapy. At the one-year follow-up, eight patients (72.7%) achieved complete recovery, and the remaining three (27.3%) had only mild (degree “1”) residual stenosis and were asymptomatic (Table 3).
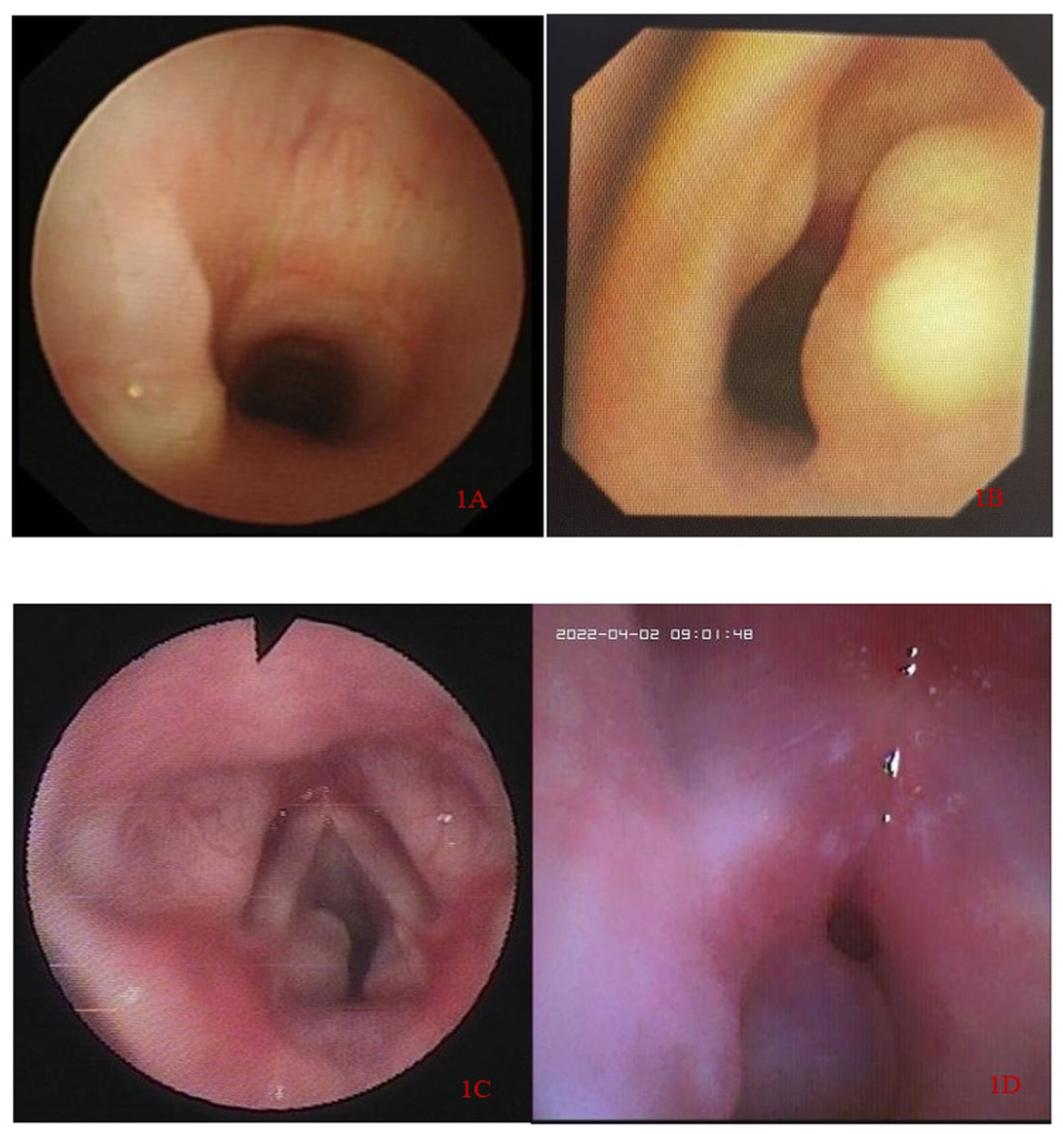
The different morphological classifications of SGCs. (a) 1111, the subglottic region, intraluminal growth, stenosis degree ⩽ 25%, stenosis length < 1cm. (b) 1131, the subglottic region, intraluminal growth, stenosis degree 51~75%, stenosis length < 1 cm. (c) 1142, the subglottic region, intraluminal growth, stenosis degree 76%~90%, stenosis length 1~3 cm. (d) 1152, the subglottic region, intraluminal growth, stenosis degree>90% and nearly completely occluded, stenosis length 1~3 cm.
Morphological classification, treatment, and outcomes of the 11 children with SGCs.

1111: the subglottic region, intraluminal growth, stenosis degree⩽25%, stenosis length<1 cm, 1131: the subglottic region, intraluminal growth, stenosis degree 51~75%, stenosis length<1 cm, 1132: the subglottic region, intraluminal growth, stenosis degree 51%~75%, stenosis length 1~3 cm, 1142: the subglottic region, intraluminal growth, stenosis degree 76%~90%, stenosis length 1~3 cm, 1152: the subglottic region, intraluminal growth, stenosis degree>90% and nearly completely occluded, stenosis length 1~3 cm.
Cryo, Cryotherapy; Ho, Holmium laser; m, Months.
Discussion
SGCs are a rare cause of upper airway obstruction, with a detection rate of 0.2‰ in our institution, consistent with their known rarity. The etiology has been classified as congenital or acquired (secondary to mucosal injury from endotracheal intubation).1,2 In this study, seven (63.6%) cases were secondary SGCs. The majority were male, aligning with previous reports.2,8,15 We identified eight (72.7%) cases with a history of prematurity and seven (63.6%) with a history of intubation, figures lower than those reported in other studies.2,5,15 Further analysis revealed that these non-intubated patients were older at diagnosis (median 56.2 vs 10.4 months), suggesting that SGCs may develop through other mechanisms or, more likely, that the diagnosis is often delayed or overlooked in children without an intubation history.
Our results showed that stridor (72.7%), wet cough (72.7%), shortness of breath (72.7%), and dyspnea (54.5%) were the common symptoms. SGCs should be considered in patients with histories of prematurity and perinatal intubation, presenting with stridor and upper airway obstruction. The median diagnosis time in this group of children was 7 months, indicating that clinicians’ ability to recognize SGCs needs improvement. SGCs should be confirmed and accurately evaluated by laryngoscopy or bronchoscopy as early as possible. SGCs are submucosal or superficial, 16 and retention cysts are thought to occur as a result of fibrosis and scarring following trauma from endotracheal intubation.17,18 SGCs can be solitary or multiple, developing in both the lateral walls and the posterior wall of the subglottic space.2,5,19 In line with previous reports,4,12 we found that eight (72.7%) cases occurred in the left lateral wall. These findings appear to support the iatrogenic hypothesis. As intubators are usually right-handed, this may increase the risk of left subglottic mucosa injury. 20 However, D.R. Toriumi et al. primarily detected posterior SGCs, 21 as the mucosa over the posterior lamina of the cricoid cartilage was pushed anteriorly against the endotracheal tube by the lordosis of the cervical spine. 22
Studies showed the possible correlation between SGCs and gastroesophageal reflux.18,23 Regrettably, patients in this study did not undergo gastroesophageal reflux tests. However, we found a high prevalence of LPRD (45.5%) in this study. To our knowledge, no studies have indicated the possible correlation between SGCs and laryngopharyngeal reflux.24,25 Although no significant difference in clinical manifestations was found between patients with and without laryngopharyngeal reflux, our results showed that two patients with laryngopharyngeal reflux relapsed after endoscopic therapy. Whether laryngopharyngeal reflux is a contributing factor or a coincidence of SGCs requires further study to confirm.
Observation is suitable for asymptomatic cysts, while surgical or interventional treatment is appropriate for symptomatic cysts.1,2,26 The gold standard therapy is endoscopic marsupialization.2,4,5,10 In our cases, eight patients had cyst excision, and two patients relapsed after the first cyst aspiration treatment, a rate lower than that in a previous study.2,5,10 Therefore, suction is strictly a short-term measure and not a definitive treatment. Meanwhile, skilled surgical technique and adequate endoscopic marsupialization are necessary for SGC patients and have been confirmed to reduce recurrence. 4
Soloperto et al. demonstrated that subglottic cysts could not be reliably assessed or managed by flexible fiberoptic nasopharyngolaryngoscopy, whereas suspension laryngoscopy using a rigid endoscope enables precise evaluation of the glottic and subglottic regions, making it suitable for the comprehensive management of subglottic cysts. 2 Seven pediatric patients underwent marsupialization of subglottic cysts via suspension laryngoscopy. Recently, a few studies reported successful management of SGCs by flexible bronchoscopy. 15 In this study, case 11 was successfully treated with holmium laser and cryotherapy via bronchoscopy. Of these, cases 1 and 11 exhibited coexisting bronchial stenosis, and bronchoscopy allowed for better assessment of the airway condition. Therefore, it suggests that SGCs could be treated by bronchoscopic marsupialization, and the airway condition can be better evaluated via flexible bronchoscopy.
Strengths and limitations
This study retrospectively enrolled patients over a 12-year period, representing the largest reported sample size in China. It also suggests that pulmonologists can treat SGCs via bronchoscopy. However, the single-center, retrospective nature of the data, recorded over 12 years, implies a risk of recall bias, with potential data parameters limited by the quality of data recorded at the time.
Conclusion
SGCs should be suspected in children with persistent stridor and respiratory distress, particularly those with a history of prematurity or intubation. Endoscopic marsupialization is a highly effective treatment, and the procedural choice (rigid vs flexible) should be tailored to the patient’s specific anatomy and comorbidities.
Supplemental Material
sj-doc-1-tar-10.1177_17534666251410167 – Supplemental material for Subglottic cysts as an uncommon cause of upper airway obstruction: a 12-year retrospective study
Supplemental material, sj-doc-1-tar-10.1177_17534666251410167 for Subglottic cysts as an uncommon cause of upper airway obstruction: a 12-year retrospective study by Guangli Zhang, Chongjie Wang, Xiaoyin Tian, Jian Luo, Yuanyuan Li, Fengtao Suo, Li Zhang, Ruixue Gu, Xiaohong Xie and Zhengxiu Luo in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.