
Abstract
Background:
Self-expandable metallic stents (SEMS) are increasingly used in the management of both malignant and nonmalignant airway stenosis. There are multiple stents available in the market; however, the current literature on the efficacy and safety of newly available 3rd generation SEMS (Bonastent) is extremely limited and only has data from single center studies.
Objectives:
To report the efficacy and early (<7 days) and late (⩾7 days) complications in patients with central airway obstruction (CAO) treated with Bonastent placement at two institutions.
Design:
We performed a retrospective analysis of data of consecutive patients who underwent therapeutic bronchoscopy and Bonastent placement at two tertiary care university hospitals between January 2019 and November 2023.
Methods:
Bonastent deployment was performed in the operating room. Stents were deployed using rigid or flexible bronchoscopy under direct visualization with a flexible bronchoscope and in conjunction with fluoroscopic guidance. We then analyzed the effectiveness, short-term, and long-term complications of Bonastent placement.
Results:
A total of 107 Bonastents® were placed in 96 patients. The most common etiology of CAO was malignancy, 92.7% (n = 89), followed by excessive dynamic airway collapse (EDAC) and post-intubation tracheal stenosis. Seventy-three patients (76%) had improvement in symptoms or imaging within 7 days of stent placement, including successful liberation from mechanical ventilation in a patient with CAO. Early complications occurred in seven patients (two-airway bleeding, two-mucus plugging that improved with airway clearance, two-stent migrations, and one-cough).
Late complications occurred in 23 patients (1-stent migration requiring revision bronchoscopy and replacement of airway stent, 11-mucus plugging, 6-granulation tissue, 2-pneumonia, 1-cough, 1-tumor ingrowth/stent fracture, 1-airway emergency due to excessive granulation tissue obstructing the distal end of the stent and had a failed cricothyroidotomy leading to death). Overall, the early complication rate was 7.3% (7/96) and late complication rate was 23.9% (23/96).
Conclusion:
Our study is the first multicenter study that found a good safety profile with a low complication rate after tracheobronchial Bonastent placement with improvement in symptoms soon after stent placement.
Introduction
Central airway obstruction (CAO) is defined as narrowing of ⩾50% of the trachea, mainstem bronchi or the bronchus intermedius. CAO can be from malignant and non-malignant diseases with malignant etiology being more common and in up to 20–30% of lung cancers. 1 Malignant CAO can present purely as endoluminal tumors, extrinsic compression, or a combination of both. 2 Etiologies of nonmalignant CAO include mechanical factors which are predominantly iatrogenic, inflammatory diseases, infectious etiologies like tuberculosis, benign endobronchial tumors, excessive dynamic airway collapse (EDAC), tracheobronchomalacia, and airway complications after lung transplantation.
Management of patients with CAO should include a multimodality team approach of radiologists, thoracic surgeons, oncologists, and interventional pulmonologists. A wide variety of therapeutic modalities are available in patients with inoperable disease in symptomatic airway obstruction. Endoscopic mechanical debridement, cryo-thermal ablative therapies, or airway stent placement is recommended to improve symptom relief and quality of life in these patients. 3 In the era of personalized medicine, treatment should be individualized to optimize outcomes.
While airway stents are effective in alleviating symptoms in patients with CAO, complications are not uncommon. In malignant disease, the long-term outcome of patients is often poor; however, patients with benign CAO often have a superior long-term prognosis. Appropriate patient selection on who will benefit from airway stent insertion is paramount. The choice of stent depends on the characteristics of stenosis. The superiority of one stent over another remains unclear as there is no comparative data available.
The fully or partially covered self-expandable metallic stents (SEMS) are most commonly used in malignant CAO. 4 Stent placement is associated with increased 30-day mortality and morbidity due to stent related complications like migration, tumor ingrowth, mucous plugging, and stent fracture. 5
Metallic stents are designed to maintain patency of the airway and have gained attractiveness due to ease of deployment, optimal radial force, and lower incidence of migration. The clinical scenario essentially predicts the type of metallic stent that can be used. There are several SEMS available in the market with varying advantages and disadvantages with each stent. 6
Here we report our experience with the newly available third generation SEMS, Bonastent (Thoracent Inc., Alpharetta, GA, USA) (Figure 1). It is a fully covered nitinol stent with variable sizes extending from 10 × 20 mm to 20 × 80 mm (diameter × length) that can be delivered with an ultra-thin coaxial deployment system and can be re-captured up to 70% deployment. 7
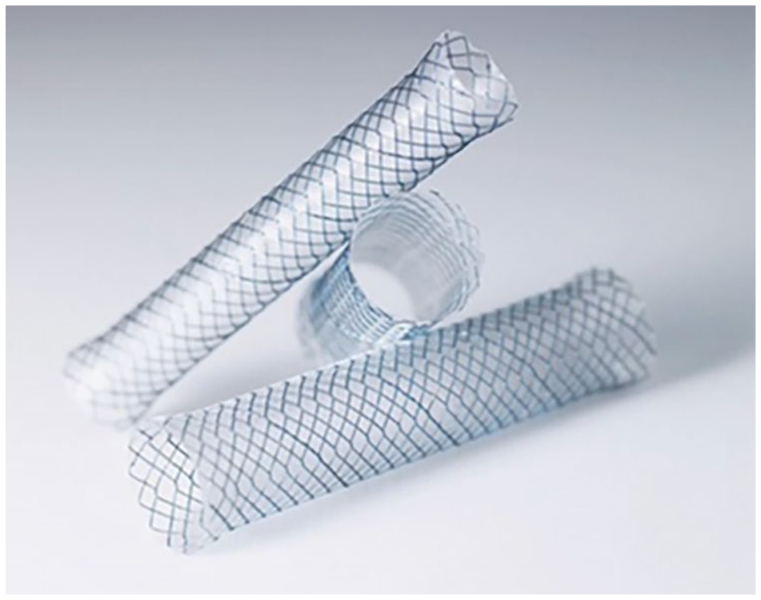
Bonastent, fully covered self-expandable metallic stent.
Little is known about the newly available Bonastent with regard to outcomes in CAO. Given how commonly this is found in lung malignancy, data regarding this stent’s efficacy is imperative to know. The available data currently consist of case reports and smaller single center series. This retrospective study is the first multicenter study, showing outcomes of both benign and malignant etiologies. It is also the largest study in non-transplant patients and second largest in all patients.8–11
Patients and methods
This is a retrospective analysis of data collected between January 2019 and November 2023 at two university hospitals in the United States (Albany Medical Center Hospital, Albany, NY, USA and Cooper University Hospital, Camden, NJ, USA). Inclusion criteria included patients 18 years of age or older who underwent therapeutic bronchoscopy and Bonastent (Thoracent Inc, Alpharetta, GA) for either malignant or benign CAO. Exclusion criteria included patients under the age of 18 and/or unable to undergo bronchoscopy (i.e. medical instability, anesthesia concerns). Institutional databases were queried for airway stent placements performed by interventional pulmonology.
All the therapeutic procedures needing stent deployment were performed in the operating room, and 46.8% of stents were deployed using rigid bronchoscopy under direct visualization with a flexible bronchoscope in conjunction with fluoroscopic guidance. Rigid bronchoscopy was used in patients where adverse events were anticipated, tumor debulking was planned, and as a part of fellowship training programs to increase exposure. Stent deployment location was estimated by guidewire under fluoroscopy, with eventual Bonastent placement confirmed both fluoroscopically and bronchoscopically. All the patients who underwent stent placement were placed on aggressive mucociliary clearance regimen with hypertonic saline and acetyl cysteine nebulization.
This study was approved by the Cooper University Hospital Institutional Review Board (IRB# 20-028) and Albany Medical Center Hospital (IRB# 6500) with a waiver to informed consent provided. Patient data were collected from the electronic medical record using a standardized form. Information collected included demographic data (age, sex), indication for stenting, type of lesion, and stent data (date of placement, type and size of stent, location of stent placement, post-stent airway patency, date of removal, and stent-related complications that include obstruction from granulation tissue, mucous, tumor in-growth, stent fracture, stent migration, and airway infection). Improvement in respiratory symptoms, radiological improvement and bronchoscopic data (type of bronchoscopy, therapeutic interventions used), and need for repeat bronchoscopy were collected. Complications occurring within 7 days of procedure were defined as early complications, and complications occurring after seven were defined as late complications.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 12
Statistical analysis
Continuous data are summarized by the mean and standard deviation and the median with the interquartile range with inference by Welch’s t-test. Categorical data are summarized by frequencies and proportions with inference by Pearson’s chi-square test or, if the expected value in any cell is less than five, by Fisher’s exact test. Minitab statistical software was used for the analysis. As this is an exploratory study, no multiplicity correction was applied.
Results
In the period between January 2019 and November 2023, 96 patients with CAO had 107 SEMS (Bonastents) placed. Malignancy was predominantly the cause of CAO (92.7%) in 89 patients, 4 patients (4.16%) had EDAC, and 3 patients had post-intubation tracheal stenosis. The mean patient age was 63.18 ± 14.46 years (18–89 years.), with 48 patients (50%) being female (Table 1).
Baseline patient characteristics.

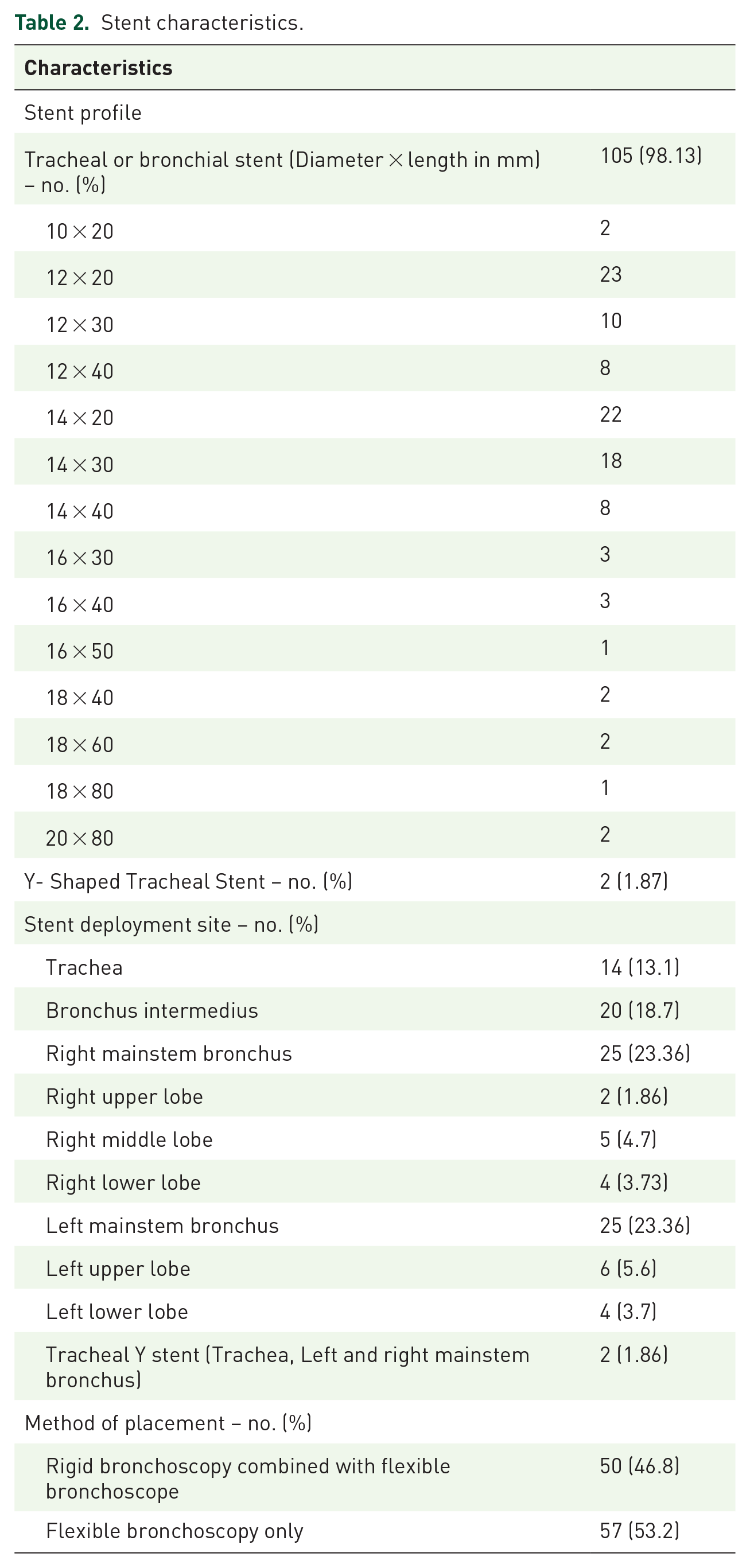
Dyspnea with hypoxic respiratory failure was the most predominant presentation in these patients followed by cough. Multimodal therapy was utilized in 81/96 (84.4%) with argon plasma coagulation (APC), balloon dilation, and bipolar gold probe. The latter was the most predominant modality followed by cryo-debridement and mechanical debridement. Most common locations for stent deployment were left mainstem bronchus (23.36%), right mainstem bronchus (23.36%) and bronchus intermidius (18.7%). Details of stent profile and deployment site are summarized in Table 2.
Stent characteristics.
The rate of early complications (⩽7 days) after tracheobronchial stent placement was 7.3% (7/96), and 23.9% (23/96) of patients had late complications (>7 days), with an overall complication rate of 31.2% (30/96), (Table 3). Statistical analysis revealed no significant difference between patients with complications (early and later) as compared to patients without complications (Table 4).
Stent related complications.

APC, argon plasma coagulation.
Statistical analysis of complications and no complications
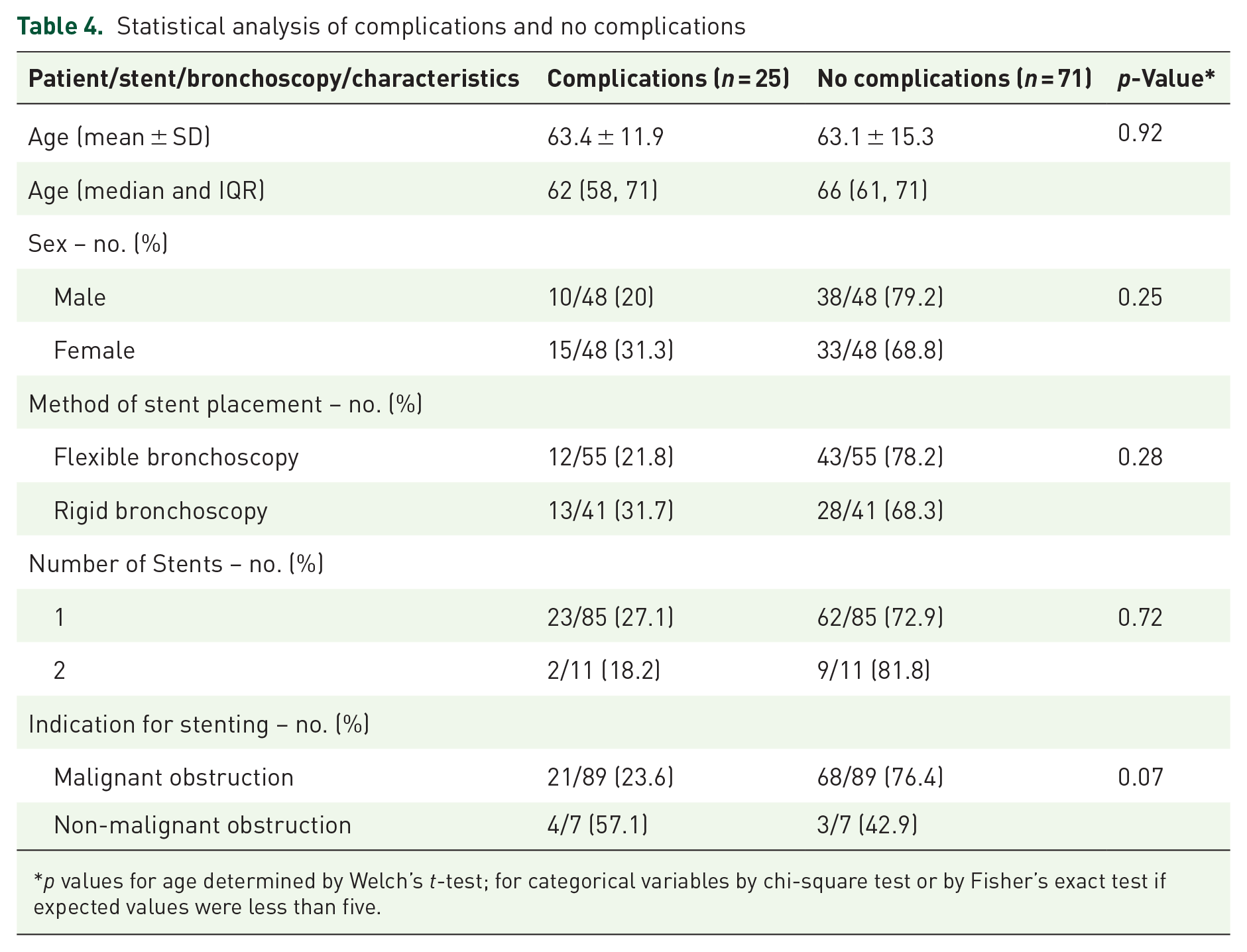
p values for age determined by Welch’s t-test; for categorical variables by chi-square test or by Fisher’s exact test if expected values were less than five.
Outcomes
Overall, 76% (73/96) of the patients had improvement in respiratory symptoms or radiologically within 7 days of stent placement. Two patients with CAO and severe hypoxic respiratory failure required mechanical ventilation. These two patients had CAO from lymphomatoid granulomatosis and non-small cell lung cancer. They were successfully extubated 2 days after endobronchial stent placement (Figure 2). An example is shown in Figure 3(a)–(d) of one patient with an endobronchial lesion. Due to only achieving partial removal of the endobronchial lesion, residual airway obstruction was present, so a Bonastent was placed which greatly improved the patency of their airway. That patient eventually needed stent removal due to mucous impaction (Figure 3(e)).

Portable chest radiograph showing opacification of the right hemithorax pre-stent ((a) and (b)) and status-post Bonastent in the bronchus intermedius ((c) and (d)) showing improved aeration of the right lower lobe.

Images (a)–(d) are bronchoscopic views. Images (a) and (b) show a large endobronchial lesion in the left main bronchus. Images (c) and (d) are after partial removal of the endobronchial lesion and after stent placement. Image (e) endobronchial stent with mucous impaction that was removed.
Discussion
Our study is currently the largest non-transplant study, and the first multi-center study examining outcomes of Bonastents in CAO both benign and malignant in etiology, and showed most patients had symptomatic improvement with low failure/complication rates.
An airway stent is an endobronchial prosthesis frequently used to restore and preserve airway patency in CAO from various causes. Traditionally, malignant CAO either from extrinsic or intrinsic compression of the airway is the most common indication for a stent placement. 4 Regarding intrinsic compression from endobronchial obstructions, options include debulking or APC. However, this may be only partially completed, or there may be co-existent extrinsic compression causing residual obstruction, requiring airway stenting. This is mainly for palliative purposes to provide symptomatic relief and improve the quality of life in such patients. In recent years, airway stents are being increasingly used for CAO from non-malignant causes such as airway obstruction from benign tumors, tracheoesophageal fistula (TEF), EDAC, subglottic stenosis, among others.1–4
There are a variety of SEMS in the market; however, the current literature on efficacy and safety is limited. First-generation stents are from uncovered balloon-expandable stainless-steel stents. Second generation stents are made of SEMS composed of nitinol. Bonastent is a newly available third generation fully covered SEMS that was developed after the United States Food and Drug Administration issued a warning in 2005 regarding the risk of stent-related complications and difficulties associated with earlier generation stent retrieval.13,14 Advantages of these third-generation stents include conforming to airways without losing diameter, ability to be deployed through a flexible bronchoscope, multiple size options, and fully covered nature to reduce ingrowth of tissue and aid in removal. 13 As noted earlier, rigid bronchoscopy was mostly performed in our patients if tumor debulking or complications were anticipated and to further trainees exposure.
The high radial force and traumatic borders of the metallic stents account for devastating complications. The new generation stents are made from alloys, most used is nitinol (titanium and nickel alloys). These stents have ‘shape memory’ and decrease the risk of airway perforation, because they retain length and shape even with cough. 15 Complications of airway stents include stent migration, infection, stent fracture, mucoid impaction, granulation tissue, and tumor ingrowth.
Currently, there is limited data regarding the efficacy and safety of Bonastent. To date, there are four case series published, three of these were mainly about malignant airway disease.8–11 Recently, a large case series was reported by Sinha et al. in patients with lung transplants with Bonastent being the most frequently used covered metallic stent. The stent breakdown was 219 Bonastent (58.24%), followed by 130 (34.57%), then Atrium Icast, and 27 (7.18%) Aerostents. The main indication for stent placement was bronchial stenosis. The authors analyzed the complication rates of each individual stent placed, and they found them to have a similar complication rate except for a higher fracture rate noticed in Bonastent. The most common complications of Bonastents include secretions (51%) followed by granulation tissue (32.88%), migration (13.2%), and fracture (6.5%). The most common reason for stent removal was mucous plugging followed by granulation tissue in all the stents used. 11 Currently, there is limited safety data of SEMS in benign disease, and this study provides insight into the safety profile of SEMS, especially on the Bonastent in the treatment of benign airway disease. We found an acceptable safety profile on par with malignant airway diseases.
Holden and colleagues had sixty stents placed in mainly malignant airway disease and found an overall complication rate of 54%, similar to previously published studies. The most common complication [early versus late (30 days)] is mucous plugging noticed at 8.3% versus 23.5% followed by granulation tissue 6.7% versus 14.7% and cough 5.0% versus 14.7%. 8
Avasarala et al. 9 have reported three cases of granulation tissue, two cases of stent migration and one case of stent fracture while Makkar et al. 10 reported mucous plugging in three patients and stent migration in one patient with a total of 13 stents placed in 11 patients in each study.
In our study, we have noticed an overall complication rate of 31.5%. The most common late complications (⩾7 days) were mucous impaction noticed in 11.6% followed by granulation tissue of 5.3%. Stent migration was noticed in three patients; one in a patient who underwent tracheal stent placement for a TEF, and two left main bronchial stent from extrinsic tumor mediastinal compression. The first patient with a TEF likely had migration from the TEF itself. The latter two were likely from undersizing. The tracheal stent could not be replaced due to medical instability; therefore, it was removed, the left bronchial stents were replaced. The complication rates that were noticed in our study are lower than that of the larger study reported by Holden et al. and Sinha et al. with significant improvement in respiratory symptoms within a week.8–11 One likely explanation for low mucous impaction in our study could be from aggressive mucociliary clearance with hypertonic saline and acetyl cysteine nebulization and surveillance bronchoscopies.
In lesions with tight stenosis, the airways stents tend to migrate distally or proximally during deployment leading to misdeployment/malposition. A unique feature of Bonastent is that it could be recaptured/re-sheathed and adjusted to desirable position until the stent is deployed up to 70% averting this issue. Another interesting feature of Bonastent is that smaller stents with sizes less than 12 mm could be deployed through the working channel of a therapeutic bronchoscope. Lastly, Bonastent has three radiopaque markers that could be of great importance while working with long stenosis (Figure 4). 7

Bonastent showing deployment handle. After deployment, the stent could be adjusted up to the redline, with the black line denoting complete deployment.
Our study has several limitations, including its retrospective nature and that patients may have received other interventions. We did not account for additional interventions (including dilation, APC) that were offered to treat CAO in conjunction with stent placement, which could have impacted the safety profile of the SEMS. We did not perform a power analysis for sample size calculation, which is another limitation of this study. Further prospective studies are necessary to understand the safety and complication of Bonastent.
Conclusion
Our study is the first multicenter study on Bonastents, adds to the literature, and reiterates the safety and efficacy of new SEMS (Bonastent) placement in CAO. Bonastents have an acceptable complication rate with good efficacy.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241260235 – Supplemental material for A multicenter observational study assessing the safety, feasibility, and complications of Bonastent in central airway obstruction
Supplemental material, sj-docx-1-tar-10.1177_17534666241260235 for A multicenter observational study assessing the safety, feasibility, and complications of Bonastent in central airway obstruction by Nagendra Y. Madisi, Sana Ali, Daniel Greenberg, Gowthami Kobbari, Muhammad Salick, Anoosh Parimi, Ziad Boujaoude and Wissam Abouzgheib in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.