
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) is characterized by multiple systemic comorbidities, not only airflow limitation. Metabolic syndrome (MetS) is a common comorbidity. Patients with COPD have a higher risk of MetS than do healthy individuals.
Objectives:
We aimed to investigate the prevalence of and explore the factors associated with MetS in Thai COPD patients and to assess the clinical consequences of MetS after a 5-year follow-up period.
Methods:
A prospective observational study was conducted in patients with stable COPD at Songklanagarind Hospital between June 2015 and November 2019. MetS was defined according to the International Diabetes Federation 2005 criteria. The patients were followed-up for 5 years. The prevalence, associated factors, and consequences of MetS were analyzed.
Results:
A total of 115 patients with COPD were enrolled, of whom 95.3% were male. The overall prevalence of MetS was 37.4% (43 patients). Chronic bronchitis and high C-reactive protein (CRP) levels were independently and significantly associated with MetS in patients with COPD (p = 0.036 and 0.044, respectively). After following patients for 5 years, the incidence of cardiovascular disease and stroke, exacerbation rate, and mortality rate were significantly higher in the COPD with MetS group [relative risk (RR) = 15.36, 95% confidence interval (CI) = (2.13–110.67), RR = 45.43, 95% CI = (4.61–447.07), RR = 1.94, 95% CI = (1.40–2.70), and RR = 48.01, 95% CI = (1.12–2049.43), respectively].
Conclusion:
The prevalence of MetS is high in patients with COPD. Chronic bronchitis and high CRP levels are associated with MetS in COPD. The incidence of clinical consequences was significantly higher in patients with COPD and MetS after a 5-year follow-up. Screening for MetS is strongly recommended for all patients with COPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic respiratory disease that was the third leading cause of death worldwide in 2019. 1 Patients with COPD also have concomitant chronic systemic diseases, including cardiovascular disease, metabolic syndrome (MetS), lung cancer, osteoporosis, skeletal muscle wasting, and anxiety/depression. 2 MetS is a common comorbidity of COPD and is defined by the clustering of abdominal obesity, hypertriglyceridemia, low high-density lipoprotein cholesterol (HDL-c) levels, hypertension, and hyperglycemia. 3 The overall mean prevalence of MetS in patients with COPD was 34% (21–58%) in a recent systematic review and was significantly higher than that in control subjects. 4
The coexistence of COPD and MetS was originally considered based on the theory of systemic inflammation, lung function impairment, and aging.5,6 Moreover, some recent pathogenic hypotheses have been put forward, based on the clinical characteristics of MetS. Hyperlipidemia can cause fatty acid–induced inflammation and activate the innate immune system. Second, abdominal adiposity increases leptin levels and decreases adiponectin levels, leading to airway smooth muscle hyperplasia and subepithelial fibrosis. Third, hyperglycemia and insulin resistance may cause mechanical and functional changes in the airway smooth muscle. These processes lead to bronchial hyper-responsiveness and airway obstruction. 6
The exact association between COPD and MetS remains unclear, however. Most previous data were derived from the United States and European countries; therefore, the previously reported findings might depend on genetics, lifestyle, and culture. No prior study has investigated the prevalence, associated factors, and clinical consequences of MetS in patients with COPD. In this study, we aimed to investigate the prevalence of and explore the factors associated with MetS in Thai COPD patients and to assess the clinical consequences of MetS after a 5-year follow-up period.
Methods
Study populations and design
This prospective 5-year observational study was conducted at a tertiary hospital that is a major referral center for 14 provinces in southern Thailand from June 2015 to November 2020. Patients were eligible for this study if they met the following criteria: age ⩾40 years, stable COPD diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines 2015, 2 and followed up at the outpatient department. Patients were excluded if they had asthma and COPD overlap, had an acute exacerbation within 2 months before enrollment, had an abnormal abdominal contour, or had a recent infection (within the previous 1 month). Patients with recent infection within 4 weeks, inflammatory bowel disease, connective tissue disease, active arthritis, and active malignancy were also excluded due to C-reactive protein (CRP) level interference.
MetS was defined according to the International Diabetes Federation global definition of MetS 3 as follows: people with central obesity (defined as waist circumference values >90 cm for men and >80 cm for women) or body mass index >30 kg/m2, plus any two of the following four factors: triglycerides (TGs) >150 mg/dl or taking medication for this lipid abnormality, HDL-c <40 mg/dl for men or <50 mg/dl for women or taking medication for this lipid abnormality, systolic blood pressure >130 mmHg or diastolic blood pressure >85 mmHg or taking medication for previously diagnosed hypertension, and fasting blood sugar (FBS) levels >100 mg/dl or previously diagnosed type 2 diabetes.
Demographic data – including age, sex, body mass index, smoking history, COPD severity, forced expiratory volume in 1 s (FEV1)% predicted, FEV1/forced vital capacity ratio, Modified Medical Research Council Dyspnea Scale, COPD Assessment Test, exacerbation rates in the previous year, and medication – were collected. Chronic bronchitis type was defined by chronic productive cough at least 3 months per year for two consecutive years, whereas other COPD patients without these symptoms and evidence of emphysema from chest imaging were classified into emphysematous type. 2
Blood tests for FBS, hemoglobin A1c (HbA1c), lipid profile, and CRP levels were obtained at the study entry and measured at the central laboratory of Songklanagarind Hospital. FBS was measured using enzymatic hexokinase/G-6-PDH (Abbott GmbH & Co., Wiesbaden, Germany). Glycated hemoglobin levels were measured using capillary electrophoresis (Capillarys 2; Sebia, Lisses, France). TG levels were measured using glycerol phosphate oxidase (Abbott GmbH & Co.). HDL levels were measured using an accelerator selective detergent (Abbott GmbH & Co.). CRP level was measured using turbidimetric/immunoturbidimetric methods (SENTINEL CH. S.p.A., Milano, Italy). COPD patients with MetS received standard treatment during the follow-up period, including lifestyle modification and medication according to their primary doctors’ opinion.
Outcomes
The primary outcome was the prevalence of MetS in the participating Thai COPD patients. The secondary outcomes were the associated factors and clinical consequences of MetS, after a 5-year follow-up period, in patients with COPD.
Statistical analyses
The sample size was calculated by estimating an infinite population proportion from the application called n4Studies 7 according to a previously published study on MetS prevalence in patients with COPD. 4 The total required sample size, which included an additional 10% for missing data, was at least 98 patients.
Continuous demographic data are reported as mean value ± standard deviation or median with interquartile range. Discrete parameters are presented as counts and percentages. The Chi-square test or Fisher’s exact test was used to compare differences in categorical variables, whereas Student’s t test was used for continuous variables.
Variables yielding p < 0.2 in the univariate analysis were included in the multivariate logistic regression analysis to determine the factors associated with MetS in patients with COPD, with significant clinical consequences. Statistical significance was set at p < 0.05. All statistical analyses were performed using Stata/MP 16.0 Mac (StataCorp LLC, College Station, TX, USA).
Results
MetS prevalence in COPD patients
A total of 121 patients with stable COPD were screened, of whom 115 patients were included in this study. Three patients were excluded due to acute exacerbation before the baseline visit and three patients declined to participate. A total of 43 of these patients (37.4%) were diagnosed with MetS. All patients were followed-up for 5 years (Figure 1).

Patient flow diagram.
The prevalence of each MetS component is summarized in Figure 2. In both MetS and non-MetS groups, the MetS components most frequently found in both groups were high fasting blood glucose and high blood pressure. All MetS components were significantly more common in the COPD group with than in the group without MetS (p = 0.013).
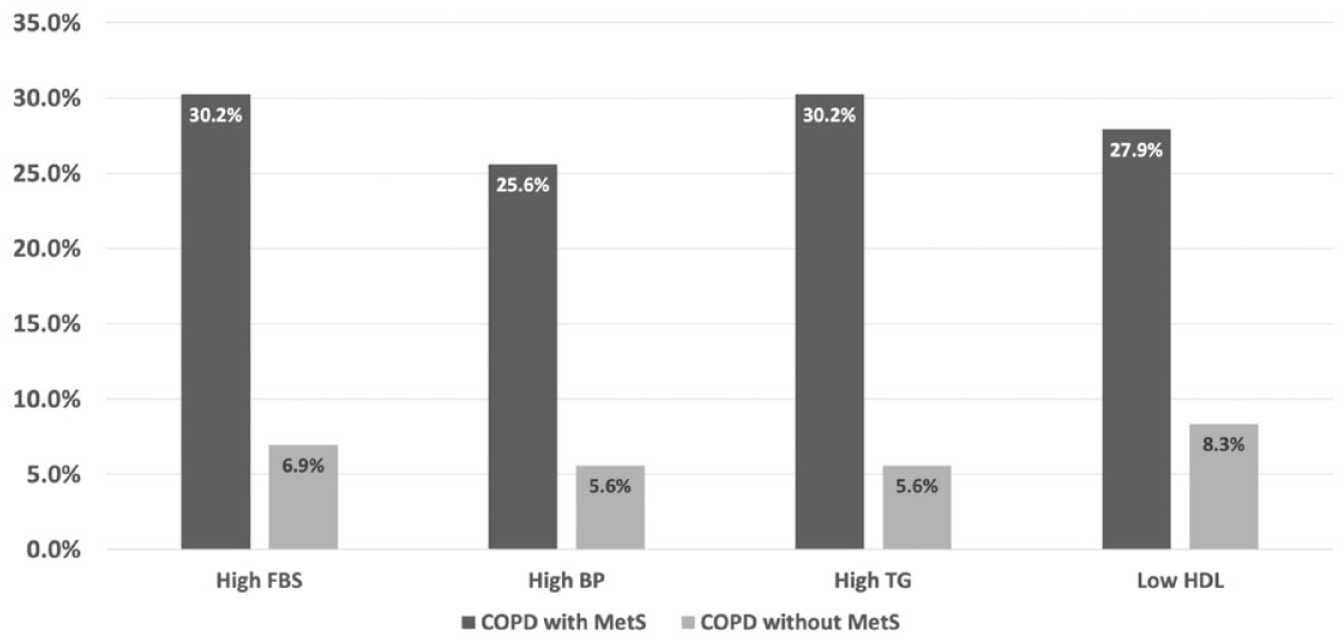
Prevalence of each component of metabolic syndrome (MetS) in patients with chronic obstructive pulmonary disease (COPD) with and without MetS.
Patient characteristics
Patients’ baseline characteristics are presented in Table 1. Most patients in this study were male (90.4%). COPD patients with MetS were mostly classified as having very severe airflow limitation based on FEV1 (30.2%) and as group C based on GOLD assessment (30.3%). Compared with patients with COPD without MetS, COPD patients with MetS were more obese (29.8 ± 3.0 kg/m2 versus 21.5 ± 3.1 kg/m2; p < 0.001), had chronic bronchitis-type COPD (87% versus 9.7%; p < 0.001), and had CRP levels >0.6 mg/l (58.1% versus 12.5%; p < 0.001). The percentage of long-acting muscarinic antagonist use was also significantly higher in patients with MetS (34.9% versus 20.8%, p = 0.041). Systolic and diastolic blood pressure, FBS, TG, and HDL-c levels were notably higher in the MetS group defined according to the MetS criteria. There were no differences in low-density lipoprotein cholesterol levels, sex, smoking status, COPD severity, lung function, dyspnea score, and history of exacerbation between the two groups, however.
Demographic and baseline patient characteristics.

BMI, body mass index; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; DBP, diastolic blood pressure; FBS, fasting blood sugar; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HbA1c; hemoglobin A1c; HDL, high-density lipoprotein; ICS, inhaled corticosteroid; IQR, interquartile range; mMRC, modified Medical Research Council; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; LDL, low-density lipoprotein; SBP, systolic blood pressure; SD, standard deviation; TG, triglyceride.
MetS-associated factors in COPD patients
From multivariate analysis, chronic bronchitis type, and high CRP level (>0.6 mg/l) were significant potential predictors of MetS development in COPD, as shown in Table 2.
Multivariate analysis of metabolic syndrome-associated factors in chronic obstructive pulmonary disease patients.

CI, confidence interval; CRP, C-reactive protein.
MetS consequences in COPD patients
After a 5-year follow-up period, the clinical consequences of MetS in COPD patients were explored. Interestingly, stroke, coronary artery disease, and mortality were significantly more common in the group with COPD and MetS (34.9%, 53.5%, and 20.9%, respectively). Furthermore, the group with COPD with MetS had a significantly higher exacerbation rate per year, as shown in Table 3.
Clinical consequences of metabolic syndrome in COPD patients.

COPD, chronic obstructive pulmonary disease; IQR, interquartile range; MetS, metabolic syndrome.
Data are presented as n (%) or median (IQR) as appropriate.
Multivariate analysis revealed that stroke, coronary artery disease, exacerbation, and mortality were the significant clinical consequences of MetS in COPD patients. Mortality and coronary artery disease showed the highest relative risks (48.01 and 45.43, respectively), as shown in Table 4.
Multivariate analysis of clinical consequences of metabolic syndrome in chronic obstructive pulmonary disease patients.

CI, confidence interval; RR, relative risk.
All clinical consequences in the COPD with MetS group increased with age, according to adjusted predictions of probability, as shown in Figure 3.

Probability of clinical sequences in patients with chronic obstructive pulmonary disease (COPD) with and without MetS, adjusted by age. (a) Stroke, (b) coronary artery disease, (c) acute exacerbation, and (d) death.
Discussion
MetS is a silent comorbidity of COPD that impacts health status. This study yielded four important findings. The prevalence of MetS in patients with COPD was 37.4%. Factors significantly associated with MetS in COPD patients were chronic bronchitis type and high CRP level >0.6 mg/l. COPD patients with MetS had higher incidences of stroke and coronary artery disease, exacerbation, and higher mortality rates. Moreover, these clinical consequences in COPD patients with MetS were exacerbated by age.
In a previous systematic review, the overall prevalence of MetS in patients was 34%. 4 The prevalence of MetS in recent studies differed from 23% to 59%,8–13 according to geographic area, which might be due to ethnicity, body composition, lifestyle, study design, and diagnostic criteria for MetS. This study found that one-third of Thai COPD patients had MetS, which was higher than in the general population (approximately 15%), as previously reported by Lohsoonthorn et al. 14 and Pongchaiyakul et al. 15
The factors associated with the development of MetS in COPD patients in this study were chronic bronchitis type and high CRP level (>0.6 mg/l). The pathogenesis of MetS in COPD patients remains unclear. It is thought to involve multiple pathogenic mechanisms, such as systemic inflammation, adipose tissue inflammation, physical inactivity, lung function impairment, and aging.5,6,16 CRP, fibrinogen, and interleukin-6 are widely used as markers of systemic inflammation in COPD.17–19 In this study, we used CRP as a systemic inflammatory marker, because of its cost-effectiveness and wide availability in clinical practice. We found that a high CRP level >0.6 mg/l in stable COPD patients was a predictor of MetS, similar to previous studies.20,21 This finding supports the hypothesis that patients with COPD with MetS have higher systemic inflammation levels, even in a stable disease setting. Chronic bronchitis is defined as regular sputum production for ⩾3 months in 2 consecutive years, without explained conditions, according to the GOLD guidelines 2015. 2 Some previous studies have reported that chronic bronchitis in COPD patients is significantly associated with the total number and severity of exacerbations.22,23 Individuals with chronic bronchitis are typically overweight or obese. We hypothesized that these typical physical features relate to systemic inflammation more than the emphysematous type, which contributes to comorbid MetS. On the contrary, there were no differences in previously reported MetS-associated factors, such as female sex, smoking status, and inhaled or oral steroid use, between COPD patients with and without MetS in this study. These disparate findings may be due to differences in patient characteristics and study designs.
After a 5-year follow-up, we found more severe clinical consequences, including stroke, coronary artery disease, COPD exacerbation, and mortality, in patients with COPD and MetS. The relationship between COPD and cardiovascular disease commonly focuses on complex mechanisms and is not well understood. These two diseases share risk factors, such as smoking, physical activity, and exposure to air pollution. 24 We assumed that increased systemic inflammation levels in patients with COPD and MetS underlies these clinical consequences. MetS has been shown to promote cardiovascular disease, type 2 diabetes mellitus, stroke, and mortality directly.25–27 The association between MetS, COPD, and acute exacerbation has also been previously reported.13,28 It has been hypothesized that the systemic inflammatory process of MetS could precipitate acute exacerbation, as it was confirmed by this study. A high CRP level (>0.6 mg/l) can lead to MetS, reflecting that patients with COPD with MetS have systemic inflammation that could trigger an acute exacerbation. After adjusted-probability analysis, the probability of clinical consequences occurring in patients with COPD and MetS was age-dependent. Aging is a nonmodifiable risk factor for stroke and cardiovascular diseases, and increasing age is associated with an elevation in the number of acute exacerbation events.
This study revealed many aspects of COPD associated with MetS, including associated factors, clinical consequences, and mortality. Clinical consequences were evaluated using a long (5-year) follow-up period. These findings could alert pulmonologists to the importance of MetS in COPD patients. Screening for MetS in patients with COPD may facilitate earlier, proper management and prevention of clinical consequences. This study, however, had some limitations. First, it was a single-center study. Second, there were some confounding factors such as family history of cardiovascular disease and physical inactivity which also affected the consequences of MetS. Third, female patients comprised only 8% of the patients included in this study, due to the low proportion of the female Thai population exposed to smoking. Thus, we could not evaluate differences in MetS in COPD patients according to sex. Therefore, further studies should be conducted in population-based, sex-matched control patients.
Conclusion
The prevalence of MetS is high in Thai patients with COPD. Chronic bronchitis type and high CRP levels are associated with MetS in COPD patients. The incidence of cardiovascular disease and stroke, the exacerbation rate, and the mortality rate were significantly higher in patients with COPD and MetS after a 5-year follow-up period. Screening for MetS is strongly recommended in patients with COPD.