
Abstract
Background:
Fibrotic hypersensitivity pneumonitis (fHP) is associated with significant morbidity and mortality. Interstitial lung disease–gender-age-physiology (ILD-GAP) performance in fHP outside the initial cohort was never performed.
Aim:
To assess the ILD-GAP index’s ability to predict mortality in a Portuguese cohort of patients with fHP and analyse whether other clinical variables add value.
Methods:
Retrospective analysis of fHP cohort in two Portuguese ILD centres. The baseline ILD-GAP index was calculated. Survival was analysed in months; mortality was the primary outcome. Univariate and multivariate analyses to identify mortality risk factors were performed.
Results:
A total of 141 patients were included. Fifty-three patients (37.6%) died during the follow-up. The usual interstitial pneumonia (UIP) pattern was found in 49.6%, and their survival was inferior to non-UIP [32 months (interquartile range, IQR = 19, 60) versus 52 months (IQR = 28, 98), p = 0.048]. Patients with an ILD-GAP index higher than three double their risk of mortality [hazard ratio (HR) = 6.48, 95% confidence interval (CI) = (3.03–13.96)] when compared with the patients with an index between 2 and 3 [HR = 3.04, 95% CI = (1.62–5.71)] adjusting for acute exacerbation history. Even though UIP patients had worse survival, it did not reach statistical significance when UIP pattern was added to this model. Acute exacerbation history was an independent risk factor for mortality; however, ILD-GAP still predicted mortality after adjusting for this factor. PaO2 and 6-minute walk test desaturation were not significant risk factors.
Conclusion:
ILD-GAP index is a good predictor for mortality in fHP, even after adjusting for other mortality risk factors.
Introduction
The prevalence of hypersensitivity pneumonitis (HP) varies widely, ranging from 2% to 47% among interstitial lung diseases (ILD) in different registries.1–5 The HP classic division into acute, subacute, and chronic forms is outdated, and recently, a new classification into acute/cellular versus chronic/fibrotic subtypes has been proposed. 6 In this line, the recently published HP diagnosis guideline highlights the importance of subdividing into two phenotypes: acute/non-fibrotic and chronic/fibrotic. 7
It has been recognized that the chronic forms are predominant,8–11 and among the different behaviour patterns, 12 some of them have a progressive fibrosing phenotype, resembling idiopathic pulmonary fibrosis (IPF).9,10,13 In the era of antifibrotic therapy, it is of utmost importance to identify such patients, 14 ideally, before substantial clinical and functional decline got established.
The gender-age-physiology (GAP) 15 model was designed and validated in IPF and, posteriorly, the analysis of its performance was extended to other ILDs with the publication of ILD-GAP. 16 ILD-GAP was created by adding an ILD subtype variable (connective tissue disease-ILD, chronic HP, idiopathic non-specific interstitial pneumonia and unclassifiable ILD) to the original GAP model that accounted for better adjusted survival in these patients. ILD-GAP index is divided in 0–1, 2–3, 4–5, and >5 stages that predict mortality risks at 1, 2, and 3 years. For example, indexes below 3 have a 1-year mortality risk inferior to 8.8%; however, above 4, the mortality risk significantly increases and these patients can be referred to transplant, if appropriate. 16 Nevertheless, its performance was evaluated in other ILD;17,18 to our knowledge, it was never evaluated and published in the subset of chronic/fibrotic HP outside the initial cohort. This study aimed to assess ILD-GAP index’s ability to predict mortality in a Portuguese cohort of fibrotic HP (fHP) patients and analyse whether other clinical variables can have additional value.
Materials and methods
Study population
A retrospective analysis of patients with fHP, in two Portuguese ILD centres [Centro Hospitalar Universitário São João-Porto (CHUSJ) and Hospital Pedro Hispano-Matosinhos (HPH)] was accomplished. The diagnosis of HP was made according to clinical presentation, exposure, thoracic high-resolution computed tomography (HRCT), bronchoalveolar lavage (BAL) fluid, and flow cytometry and lung biopsies, as previously published. 11 All diagnoses were established in the multidisciplinary team (MDT) meeting. Patients in whom baseline ILD-GAP calculation was not feasible were excluded from the analysis. This study had the approval of the local Ethics Committee in both centres.
Measurements
Baseline demographic data (age, sex, symptoms, smoking status, antigen exposure) and pulmonary function testing, 6-minute walk test (6-min WT), and oxygen arterial pressure (PaO2) at diagnosis were recorded. Accordingly, the ILD-GAP index was calculated, and medical chart review was assessed to obtain data from BAL, lung biopsy, immunosuppressive therapy, and acute exacerbation events.
HRCTs at diagnosis were reviewed by two experienced thoracic radiologists. The combination of centrilobular nodules, ground-glass infiltration, mosaic attenuation, and middle or upper lobe distribution was considered typical for HP. Fibrotic changes included reticular pattern, traction bronchiectasis, and honeycombing. 11 Usual interstitial pneumonia (UIP) pattern was described according to the Fleischner Society terminology. 19 Biopsy samples (transbronchial cryobiopsy or surgical lung biopsy) were independently observed and evaluated by two pathologists. HP diagnosis was based on the presence of centrilobular and perilobular fibrosis, bridging fibrosis, centrilobular fibroblastic foci, granulomas, mononuclear chronic interstitial inflammation, and organizing pneumonia. If two or more findings were present, the biopsy was considered high confidence; if only one feature was present, it was considered low confidence. 11 The UIP pattern in fHP includes patchy collagen subpleural fibrosis, fibroblast foci, and associated subpleural-dominant honeycombing.
Time to mortality was the primary endpoint. All the patients were followed up from the first to the last visit, lung transplantation, or death.
Statistical analysis
Data are presented as mean (and standard deviation), when continuous, or as counts (and frequencies), when categorical. UIP versus non-UIP mean values of continuous variables were compared with independent sample t-tests, and their categorical variables’ frequencies were compared with chi-square or Fisher’s exact tests (when appropriate).
Survival was analysed with time (in months) from diagnosis to dead (primary outcome) censored by the end of follow-up or transplantation. Kaplan–Meier curves were used for survival estimates and compared with the log-rank test. Univariate and multivariate Cox proportional hazards regressions were used to identify variables that predict survival status and hazard ratios and their 95% confidence intervals computed. A final Cox regression model with forward conditional stepwise selection was obtained. A final Cox regression model was obtained through forward conditional stepwise selection. The proportional hazards assumption for the final Cox regression model was also tested. ILD-GAP was separated into three groups: ILD-GAP index 0-1, 2-3, and >3. Statistical significance was established at p < 0.05. All statistical analysis and graphical representations were performed in Rstudio, an environment for R programming language.
Results
Patient characteristics
A total of 141 patients with fHP were included in the analysis after assessing all the including criteria. The cohort baseline characteristics are presented in Table 1. The patients’ mean age was 64.7 years, 61% (n = 86) were female, and 21.3% (n = 30) had a smoking history. Avian exposure was the most frequently reported (66.7%), and 21.3% (n = 30) of the patients had an undetermined exposure. Regarding BAL fluid, the mean lymphocyte count was 30.9% ± 21.3%. Of all patients included, 36.2% (n = 51) had been submitted to lung biopsy, 49% (n = 25) with transbronchial lung cryobiopsy, 41.2% (n = 21) with surgical lung biopsy, and 9.8% (n = 5) with CT transthoracic biopsy. Concerning treatment options, 13.2% (n = 18) were under vigilance and antigen eviction, 17.6% (n = 24) were under steroids, and 69.1% (n = 94) were under immunosuppressive therapy with azathioprine, mycophenolate, or rituximab. The median follow-up time was 40 [interquartile range (IQR) = 22, 85] months. Fifty-three patients (37.6%) died during the follow-up, and 11 (7.8%) were submitted to lung transplant.
Descriptive statistics of fHP cohort and comparison between UIP and non-UIP patients.
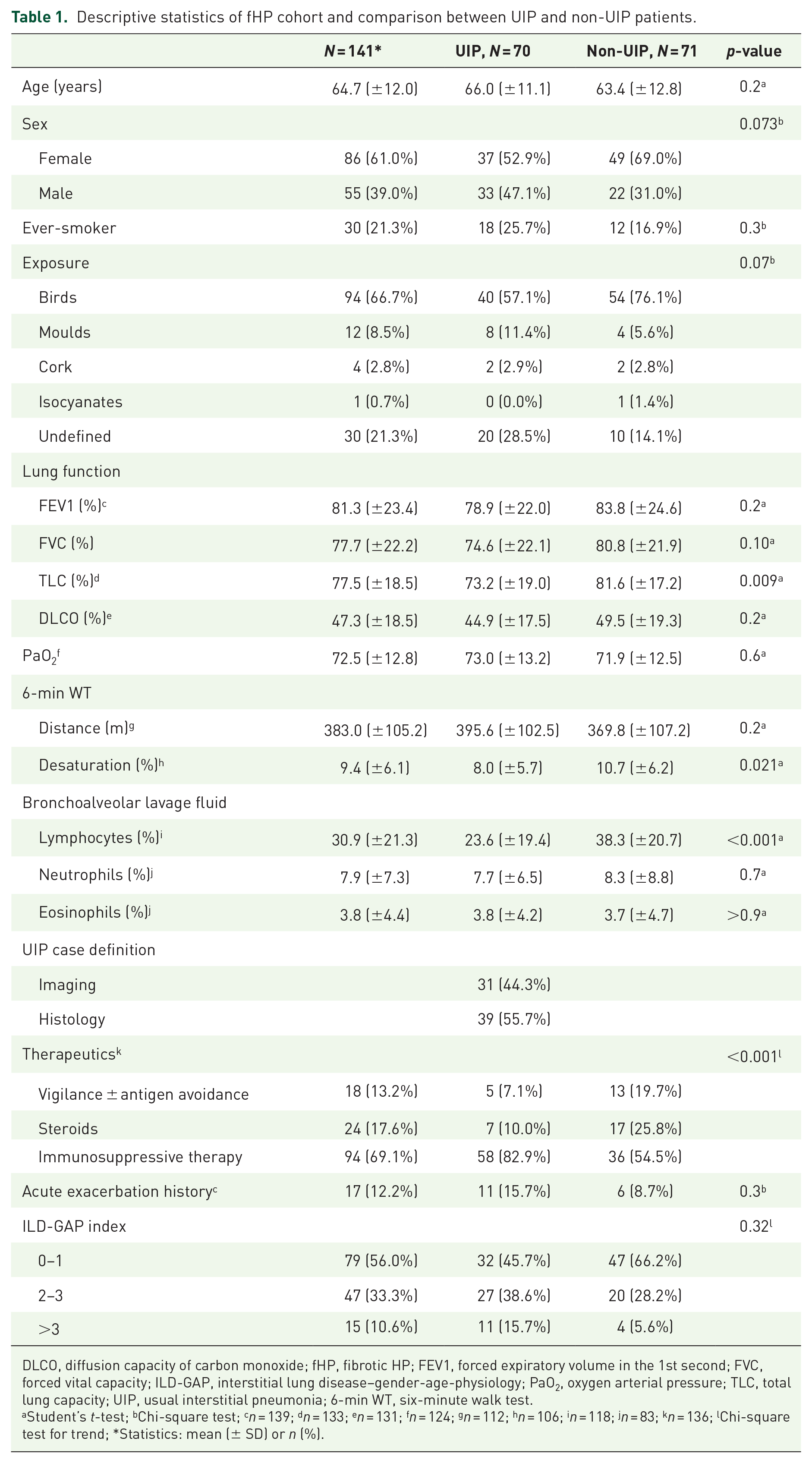
DLCO, diffusion capacity of carbon monoxide; fHP, fibrotic HP; FEV1, forced expiratory volume in the 1st second; FVC, forced vital capacity; ILD-GAP, interstitial lung disease–gender-age-physiology; PaO2, oxygen arterial pressure; TLC, total lung capacity; UIP, usual interstitial pneumonia; 6-min WT, six-minute walk test.
Student’s t-test; bChi-square test; cn = 139; dn = 133; en = 131; fn = 124; gn = 112; hn = 106; in = 118; jn = 83; kn = 136; lChi-square test for trend; *Statistics: mean (± SD) or n (%).
UIP versus non-UIP patients
Due to the high relevance of the UIP pattern in fibrotic ILD regarding prognosis, this pattern was considered and found in 70 (49.6%) patients. The UIP diagnosis was based in imaging in 31 patients (44.3%) and in 39 patients (55.7%) a biopsy sample was needed. Table 1 outlines the differences between UIP and non-UIP patients. We found that UIP had a statistically significant lower total lung capacity (73.2% ± 19% versus 81.6% ± 17.2%, p = 0.009) and lower BAL lymphocyte counts (23.6% ± 19.4% versus 38.3% ± 20.7%, p < 0.001). In 6-min WT, both groups had similar walking distances; however, non-UIP patients had slightly higher, although significant, oxygen desaturation values. Considering therapeutics, UIP patients had a significantly higher percentage of patients under immunosuppressants (Table 1). Regarding survival, the population of non-UIP patients had significantly better survival than UIP patients (Figure 1), with a median follow-up time of 52 months (IQR = 28, 98) compared with 32 months (IQR = 19, 60) in the UIP group (p = 0.048).

Survival curves for UIP and non-UIP patients.
The ILD-GAP model performance in fHP cohort/disease severity and mortality
In this fHP cohort, the ILD-GAP index is a good predictor of mortality (Figures 2 and 3). The results from univariate Cox regression analyses are presented in Table 2. PaO2 and 6-min WT were not statistically significant risk factors for mortality. However, we found statistically significant associations for other lung function parameters. A final multivariate Cox regression model was built with forward conditional stepwise selection of variables with a p-value lower than 0.1 in the univariate analysis. Hence, in the multivariate Cox regression analyses, the ILD-GAP index is a statistically significant risk factor for mortality after adjusting for acute exacerbation (Table 3). Patients with an ILD-GAP index higher than three double their risk of mortality [hazard ratio (HR) = 6.48, 95% confidence interval (CI) = (3.03–13.9)] when compared with the patients with an index between 2 and 3 [HR = 3.04, 95% CI = (1.62–5.71)] having as reference those patients with an index 0–1. From this multivariate model, we can also observe that acute exacerbation is an independent and statistically significant risk factor for mortality in this cohort of patients. When the UIP pattern was added to this model, it did not reach statistical significance.
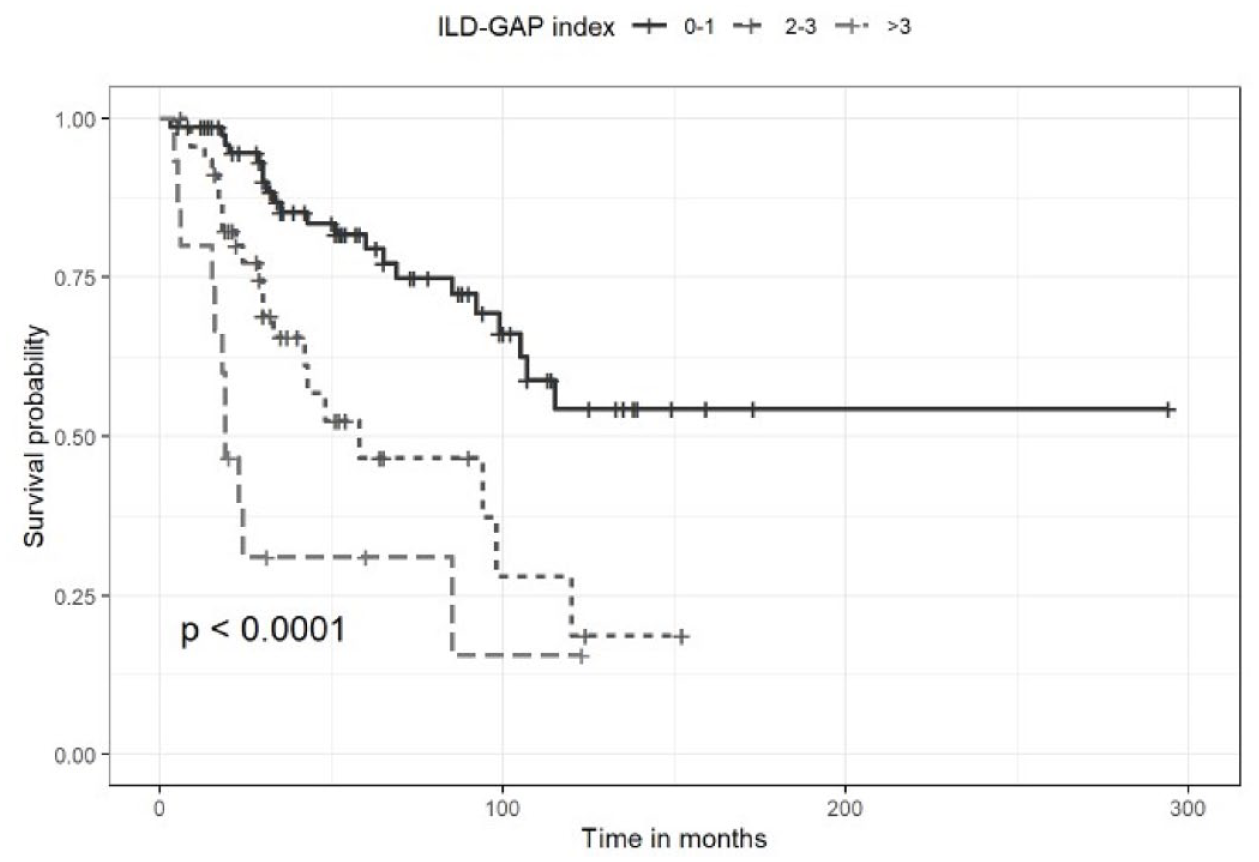
Survival curves for ILD-GAP index – complete follow-up.

Survival curves for ILD-GAP index – 36 months.
Factors associated with mortality in unadjusted univariate Cox proportional regression models.

CI, confidence interval; DLCO, diffusion capacity of carbon monoxide; FEV, forced expiratory volume; FVC, forced vital capacity; HR, hazard ratio; ILD-GAP, interstitial lung disease–gender-age-physiology; Ref, reference group; TLC, total lung capacity; UIP, usual interstitial pneumonia; 6-min WT, six-minute walk test.
Multivariate Cox regression model obtained by forward conditional stepwise selection.

CI, confidence interval; HR, hazard ratio; ILD-GAP, interstitial lung disease–gender-age-physiology; Ref, reference group.
Discussion
ILD-GAP index showed to be a good predictor for mortality in this cohort of fHP patients. In addition, acute exacerbation was also statistically significant risk factor for mortality. Nevertheless, ILD-GAP index was still statistically associated with mortality after adjusting for acute exacerbation. Baseline PaO2 and 6-min WT were not significant risk factors for mortality and, therefore, were not included in our final Cox regression model. However, when looking at UIP patients, their survival is significantly shorter than non-UIP patients, the presence of this pattern did not add mortality risk to the one predicted by the ILD-GAP index.
GAP index and staging system were initially described and validated for IPF before the approval of antifibrotic therapy and represented a useful mortality risk prediction tool, allowing better communication with patients and helping the lung transplant referral. 15 The GAP model applicability in ILD was subsequently extended with ILD-GAP, validated in major chronic ILD subtypes, including chronic HP. 16 Hyldgaard et al. 17 showed that ILD-GAP and Disease Behaviour Classification had good prognostic performance in unclassifiable ILD and were independent of one another in their association with outcome. In rheumatoid arthritis–associated ILD (RA-ILD), GAP model also demonstrated a good discrimination power for mortality risk, and this was not improved by adding rheumatoid factor positivity and UIP pattern on HRCT. 18 Notwithstanding, in myositis-associated ILD, this model showed poor prognostic performance, and the authors explained that the weight of pulmonary function in ILD-GAP might not be adequate for assessing disease severity in myositis. 20 However, these authors focused their analysis on the first 3 years of predicted mortality and did not refer if, in extended follow-up, ILD-GAP index would be a good mortality discriminator.
Regarding UIP pattern shorter survival, as in other chronic HP cohorts, 21 it did not add risk to ILD-GAP in the multivariate analysis. This might be, in part, explained by the sample size, although Morisset et al. 18 found similar results in RA-ILD. Since the UIP pattern in histology was also related to poorer survival in other cohorts,13,22,23 we included both imaging and pathology information in the UIP case definition, which explains the higher percentage of patients classified as UIP comparatively to other cohorts.21,24
Furthermore, an acute exacerbation can have a dreadful prognosis and negatively affect survival in non-IPF fibrotic ILD, 25 and indeed in our cohort, acute exacerbation history was associated with mortality. However, after adjusting for acute exacerbation risk, ILD-GAP still predicts mortality.
The desaturation in 6-min WT has prognostic value in fibrotic ILD,26,27 so we hypothesized that PaO2 levels or desaturation in 6-min WT could add value to ILD-GAP in predicting mortality. Nevertheless, in our cohort, they were not associated with mortality. On the contrary, we found a slight, though significant, desaturation in non-UIP patients; yet it did not seem clinically relevant.
Concerning BAL fluid analysis, lymphocytosis was significantly superior in the non-UIP group, which have been associated with a better prognosis. 21
This study has several limitations, namely its retrospective nature. More detailed data about HRCT, such as the extension of fibrosis, or echocardiogram, could have enriched the analysis.10,24 Another limitation is the lack of comparison between treated and untreated patients and the analysis of treatment as an independent risk factor for mortality. Even though the efficacy of corticosteroids in fHP is not adequately evaluated, its use is widely adopted due to the reports from the acute form of the disease.28–30 In our centre, immunosuppressive treatment, mainly with azathioprine or mycophenolate mofetil, is generally the first approach. However, concurrent steroids are first administered, frequently for a short period of time, in very symptomatic patients. We have shown that azathioprine can improve lung function in fHP;31,32 however, the impact on survival is not studied. In this cohort, there were different treatment durations and several patients treated with more than one drug sequentially, either due to side effects or progression of disease, which precluded the analysis of impact of treatment in survival.
Nonetheless, the data were derived from two ILD centres, combining an academic and a non-academic hospital, thereby increasing their reliability.
Finally, our study suggests that the ILD-GAP index can be used as a mortality risk prediction tool in fHP. ILD-GAP is an extremely easy to perform index, which enhances its applicability in every day clinical practice. Moreover, it is applied at diagnosis and allows identification of patients more likely to have a worse prognosis, which is exceedingly relevant in the era of progressing pulmonary fibrosis with access to anti-fibrotic therapy. 33