
Abstract
Background:
Cystic fibrosis (CF) affects more than 80,000 people worldwide, having a considerable impact on the quality of life of patients and their caregivers, who assist patients with time-consuming treatment regimens. Despite this, a review of the available evidence has not been previously undertaken. This systematic literature review aimed to identify the humanistic and economic burdens of CF on caregivers.
Methods:
A systematic literature review was conducted, in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. Publications reporting outcomes for the caregivers of people with CF, including utility data, health status, and occupational impact, were reviewed. Sources searched were Embase (OvidSP), Medline (PubMed), the Cochrane Database of Systematic Reviews, and the Epistemonikos database, from 2010 to March 2020. A subsequent search with updated terms identified articles up to April 2020. Electronic searches were supplemented by hand searches to capture all relevant literature.
Results:
A total of 889 articles reporting humanistic burden and 310 reporting economic burden were identified. Following full-text screening by two independent reviewers, 72 articles were included in the review, of which 65 and 17 reported data on humanistic and economic burdens, respectively, with 10 reporting on both. The reviewed literature covered several outcomes and identified multiple key findings: greater disease severity is associated with the reporting of greater caregiver burden and lower utility scores of quality of life; reduced patient lung function is associated with increased caregiver depression and anxiety; and caregiving causes significant occupational impact, with pulmonary exacerbations decreasing caregiver productivity by up to a third compared with the patient being in a ‘well’ state.
Conclusion:
Findings from this systematic literature review highlight the substantial humanistic and economic burdens borne by the caregivers of people with CF. Future research would help to further inform on the link between disease severity and caregiver burden.
Introduction
Cystic fibrosis (CF) is a rare disease that affects more than 80,000 people worldwide. 1 Improvements in diagnosis, including widespread newborn screening programs, mean that CF is now typically diagnosed in infancy in Western Europe and the United Kingdom. 2 Despite extensive treatment and advances in care, in 2019, the median age of death for people with CF was 32.4 years in the United States, 3 typically due to respiratory failure. Following diagnosis, caregivers, who are usually a parent or close family member, are required to carry out or assist with daily treatments, such as physiotherapy to clear static mucus from the respiratory tract 4 and the administration of nebulized treatments, along with many other different medications to treat and prevent organ damage. 5 These therapies are intended to alleviate symptoms and reduce the severity of respiratory events, such as exacerbations and infections, 6 but are time-consuming. Children with CF spend an average of 75 min/day receiving treatment, 7 which must be performed by caregivers in addition to other familial and occupational commitments. The role of the caregiver is key in the life of people with CF and, as in many different aspects of the disease, a substantial reduction in caregiver quality of life (QoL) during periods of exacerbation has been previously reported.8,9
The burden of home-based treatments, compounded by the impact on caregivers of patient hospitalizations and other healthcare contacts, results in caregiver burden, which is defined as the perceived experience of physical, psychological, emotional, social, or financial problems due to caring responsibilities. 10 However, the wider humanistic and economic burdens of caregiving in CF are currently not well synthesized. A greater understanding of the impact of caregiving on CF caregivers would assist healthcare providers in better meeting the needs of this group by, for example, targeting psychological support at those who may be at risk of developing anxiety or depression due to the burden of their caregiving responsibilities. This may also act to improve patient outcomes, as caregiver depression has been shown to lead to worse patient adherence to treatment, 11 possibly contributing to disease progression. Quantifying and understanding the burden of caregiving is also important to determine the full benefit to the healthcare system, and value to society, of new healthcare technologies, as both patients and their caregivers benefit if disease severity is reduced. 12
The aim of this study was to synthesize and evaluate the humanistic and economic burden of caregiving on the caregivers of people with CF through a systematic review of the literature. The outcomes of the review are intended to enhance understanding of the burden experienced and to augment the existing body of evidence describing the challenges faced by CF caregivers.
Methods
For the purposes of this systematic literature review, caregiver burden (experienced by the caregivers of people with CF) was defined as the strain borne by an individual who cares for a chronically ill family member. 13 Informal caregivers were identified as individuals who provide nonprofessional care to patients, for which they are not paid. These caregivers are typically relatives, but they may also be foster carers of pediatric or adolescent patients, the spouse of adult patients, or any other person caring for a patient with CF. As caregiver burden arises from, and results in, a wide range of impacts, the review included data on caregiver QoL, health status, social impact of caregiving, work productivity and absences, and direct and indirect financial impacts of caregiving. Data on caregivers’ subjective burden were also captured, pertaining to how a caregiver perceives the burden arising due to their caring responsibilities. 14 Methods were aligned with guidance published by the Centre for Reviews and Dissemination for conducting systematic reviews 15 and the Preferred Reporting Items for Systematic reviews and Meta-Analyses statement. 16
Eligibility and search strategy
Inclusion criteria are described in Table 1. Databases searched included Embase (OvidSP), Medline (PubMed), the Cochrane Database of Systematic Reviews, and the Epistemonikos database. Articles published before 2010 were excluded from the search, as were articles not published in the English language. In addition, the websites of the National Institute for Health and Care Excellence (NICE), the German Federal Joint Committee, and the French Haute Autorité de Santé were hand searched to retrieve any relevant studies not identified by the electronic searches, and to ensure that the search terms were sufficiently broad to capture all articles of interest. Following the search, to capture studies reporting humanistic burden, the decision was made to run a further search to ensure all studies reporting mental health outcomes were captured (for further details, see Supplementary Material section 1).
PICOS elements and inclusion and exclusion criteria for the economic and humanistic burden review.

CF, cystic fibrosis.
For the review, articles reporting data from individuals self-identifying as the primary or secondary informal caregivers of people with CF were included. Two independent reviewers (one of whom authored this article) screened each article using a two-stage approach (title/abstract and full text) to determine its relevance to the study question. Any discrepancies in opinion between the two reviewers were resolved by a third independent reviewer. The number of studies screened, assessed for eligibility, and included in the review at each stage is presented in Figure 1. In total, 72 publications were included in the review following full-text screening. Of these, 65 and 17 reported humanistic and economic data, respectively, with 10 reporting both.9,17 –25 Relevant data from included sources were extracted by the authors into a Microsoft Excel® database, including study characteristics, patient and caregiver demographic details, patient and caregiver QoL data, caregiver employment status, caregiver work and productivity data, caregiver time spent on care tasks, and the financial impact of caregiving.

PRISMA flow diagram of studies reporting data on (a) humanistic caregiver burden and (b) economic caregiver burden.
The methodological quality of included studies was assessed by one experienced reviewer. Studies reporting economic data were assessed using a tool adapted from the NICE Guideline, Manual Appendix H.p9. 26 Studies reporting humanistic data were assessed using guidance provided by the Good Practices for Outcome Research Task Force, established by ISPOR in 2014. 27 All studies were assessed for overall bias using the ROBINS-1 tool 28 (see Supplementary Table S1).
Results
A summary of outcomes captured in the systematic literature review is shown in Figure 2 and Supplementary Table S2. Caregiving results in a number of humanistic and economic impacts on caregivers, which were captured by a broad range of instruments across included studies. Patient-reported outcome measures, listed by outcome, are summarized in Supplementary Table S3.

Main outcomes captured by the systematic literature review, and summary of issues identified (n = number of studies reporting outcome; % = percentage of included studies reporting outcome; key publications highlighted in bold italics). As studies reported > 1 outcome, the total number of outcomes reported is greater than the overall number of studies identified.
Humanistic caregiver burden
For reporting the findings, the evidence on humanistic caregiver burden was further categorized into ‘subjective caregiver burden’, ‘preference-based measures’, ‘caregiver anxiety and depression’, ‘treatment adherence’, and ‘additional outcomes of interest’ (including patient lung function and caregiver well-being, and sleep quality in caregivers).
Subjective caregiver burden and preference-based measures
Ten studies included in the review reported data on subjective caregiver burden.9,17,21,23,24,29 –33 Five studies utilized the Zarit Burden Interview (ZBI), which produces a Zarit Burden Scale (ZBS) score,17,24,30,31,33 of which three were reporting results from the BURQOL-RD European project. The Caregiver Burden General Strain Index (CB-GSI) eight items, 21 The Child Health Questionnaire-Parent Form 28 (CHQ-PF28), 9 an informal questionnaire, 23 the treatment burden subscale of the Cystic Fibrosis Questionnaire-Revised, 32 and an undisclosed measurement tool were each used in one study. 29 The instruments used differ significantly from one another in terms of both their length and sensitivity. For instance, the ZBI utilizes 22 questions, scoring each on a 5-point scale from 0 to 4, resulting in an overall score of 0–88, 10 with scores of 21–40 defined as indicating mild-to-moderate caregiver burden and higher scores indicating a greater burden.24,34 The CB-GSI utilized only eight items, with a 4-point scale per item, which is then converted into a mean burden score, with higher scores representing a worse subjective burden. 21 The use of differing instruments across studies suggests a lack of consensus on the preferred tool for measuring caregiver burden, a finding supported by a previous systematic review of caregiver burden in schizophrenia. 35 Two additional studies utilized the CF Self-Efficacy Questionnaire of The Challenges of Living with Cystic Fibrosis-Questionnaire to assess the self-efficacy of caregivers;22,36 a summary of these data is provided in Supplementary Table S4.
Mean scores from the ZBI, the most commonly used tool to measure caregiver burden, are presented in Figure 3. Overall, studies found a mild-to-moderate subjective caregiver burden associated with CF. In the BURQOL-RD project, which investigated the well-being of people with CF and their caregivers in France, Germany, Italy, Spain, and the United Kingdom, a mild-to-moderate burden was reported by the caregivers of pediatric and adult patients with CF involved (ZBS: 21.7–31.2). 24 When analyzed separately, caregivers of pediatric patients were found to have a significantly higher ZBS score (p = 0.0013). This is likely linked to the significantly greater reported number of informal care hours per week required by young patients compared with adult patients (p = 0.0001). 24 However, it should be noted that considerably more caregivers of pediatric patients, compared with adult patients, were included in this study (ZBS score data available for 210 and 26 caregivers of adult and pediatric patients, respectively). One study compared the ZBS scores of CF caregivers with those of patients with primary ciliary dyskinesia and found that CF caregivers reported a greater burden score. 33
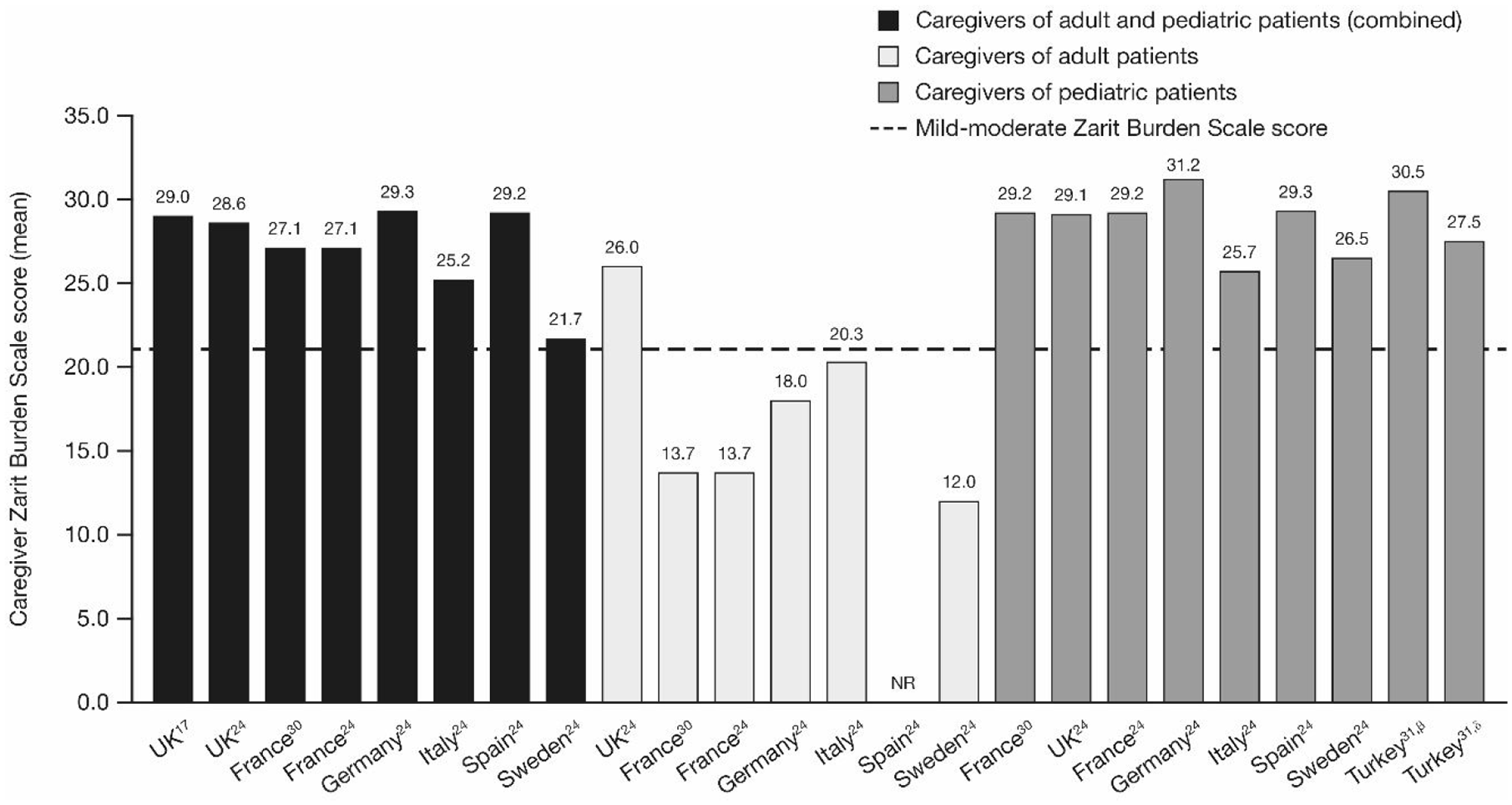
Caregiver Zarit Burden Scale score (mean) stratified by country and patient age-group (β, mothers; δ, fathers; mild–moderate perceived burden threshold from Hébert et al.). 34 Figures for caregivers of adult patients and pediatric patients are subsets of the adult and pediatric patients (combined) data; figures for adult and pediatric patients (combined) are reported as published in their respective sources, not calculated by review authors.
Caregiver burden was shown to be worse in periods of patient hospitalization for disease exacerbation, with caregivers reporting statistically significantly lower CHQ-PF28 parental impact-time scores during hospitalization versus afterwards (49.2 versus 61.0; p = 0.004). 9
Nine studies utilized preference-based measures to determine the QoL of the caregivers of people with CF.17,19,24,25,30,37 –39 Of these, one used the Ulm Quality of Life Inventory for parents of chronically ill children, 37 which consists of questions on five dimensions of QoL, scored on a 5-point scale with high scores indicating a better QoL. 37 One used the World Health Organization Quality-of-Life Assessment–Abbreviated, 40 which consists of 26 questions, and is scored from 0 to 100, with 100 representing the best QoL. Three used the EQ-5D-5 L17,24,30 and one the EQ-5D-3 L, 25 both of which generate a utility score from the participants’ scoring of five dimensions of health on a scale anchored at 0 (representing a state as bad as being dead) and 1 (representing full health), and a visual analog scale (VAS) score against which participants rate their health from 0 to 100, with 100 signifying the best imaginable health. EuroQol-5D Three studies used the Care Related Quality of Life Caregiving (CarerQol-7D) instrument,19,38,39 which consists of seven items each relating to a specific aspect of caregiving and a VAS on which caregivers indicate their well-being in terms of happiness from 0 to 10, with greater scores indicating greater happiness. Unlike the EQ-5D, the CarerQol-7D instrument assesses care-related QoL specifically. 41 The Caregiver Quality Of Life Cystic Fibrosis scale was developed specifically for use in this group; however, it has only been employed in two studies to date, 19 neither of which were included in this systematic literature review as they did not include relevant outcome data.
A summary figure of caregiver utility and VAS scores presented by instrument is shown in Supplementary Figure S1.
Chevreul et al. 24 reported utility and VAS data for caregivers of both adult and pediatric groups from the BURQOL-RD project. Caregiver utilities for caregivers of adults varied significantly by country, from 0.915 in Italy to 0.472 in Sweden. Significant variation was also found in the VAS scores of caregivers to adults, from 92.5 to 30.0 for Italy and Sweden, respectively. 24 This variation is linked to the Barthel index of patients, with caregivers of more dependent patients (as determined by a Barthel index score of ⩽ 90/100 or a modified Barthel index score of ⩽ 14/20) reporting significantly lower utility and VAS scores than caregivers of less dependent patients (p = 0.0023 and p = 0.0063, respectively). 24 Caregiver utilities and VAS scores were not found to differ significantly between caregivers of adult and pediatric patients (0.742 versus 0.765, p = 0.7904; and 76.67 versus 79.35, p = 0.97, respectively).
BURQOL-RD data from the French cohort were stratified according to disease duration. The mean utility score of caregivers of people with a disease duration of ⩾ 30 years was found to be 0.356, significantly less than any other cohort of caregivers (p = 0.0498) and indicating a significantly worse QoL for this group. Caregivers of people with a disease duration of < 10 years had a mean score of 0.738, whereas those of people with a disease duration of 10–19 and 20–29 years reported mean scores of 0.819 and 0.839, respectively. 30
The three studies that used the CarerQol-7D all reported data from the Irish Comparative Outcomes Study in pediatric patients with CF.19,38,39 In the initial combined analysis, mothers were found to have significantly lower utility scores than fathers (81.4 versus 87.4, respectively; p = 0.004) 38 and VAS scores were also significantly lower in mothers than in fathers (7.2 versus 7.79; p = 0.03). 38 However, the difference between mothers and fathers in median VAS score was not found to be statistically significant in a later publication of the complete results of the study (7.0 versus 8.0; p = 0.097). 19
Caregivers of pediatric patients colonized by Pseudomonas aeruginosa, a bacterial infection associated with worse disease progression, 42 were found to have significantly lower utility scores than caregivers of P. aeruginosa-free patients (80.3 versus 86.0; p = 0.001), 19 indicating a negative relationship between disease severity and caregiver QoL.
Caregiver anxiety and depression, and treatment adherence
Thirty-two studies assessed caregiver depression and anxiety, using a variety of tools.
Results for the Patient Health Questionnaire (PHQ) 8/9, Generalized Anxiety Disorder scale 7 items (GAD-7), Center for Epidemiologic Studies Depression scale (CES-D), Hospital Anxiety and Depression Scale-Anxiety (HADS-A), and Hospital Anxiety and Depression Scale-Depression (HADS-D) are presented graphically in Supplementary Figure S2. Additional data from other studies reporting on caregiver anxiety and depression are presented in Supplementary Table S5. One study utilized the Beck Depression Scale. 43 Three studies reported rates of depression without specifying the instrument used,44 –46 two questioned caregivers about subjective feelings of depression,47,48 and one pooled the results of three instruments together. 49 An overview of data from key studies is given subsequently.
Incidence of elevated depressive symptoms in caregivers based on PHQ score was reported by 13 studies,50 –62 and ranged between 12% 55 and 60%. 60 Of these, 11 studies,50 –54,56,57,59 –61,63 reported incidences of depressive symptoms that were substantially greater than those of the general population in Germany 64 (16–60% versus 9.2%, respectively). Further information on study results can be seen in Supplementary Table S5. Confounding factors may explain the lower scores reported by two studies. Naranjo et al. 55 investigated the caregivers of a cohort of patients with a mean percentage predicted forced expiratory volume in 1 s (ppFEV1) of 83%, 77% of which had no hospital stays within the previous 6 months, indicating relatively low disease severity and stable disease. Fisher et al. 51 found that 41% of caregivers declined mental health screening and, hence, the reported data may not be fully representative.
GAD-7 scores were reported by 14 studies50 –55,57 –59,61,62,65,66 and ranged in incidence from 4% 55 to 66%. 60 Naranjo et al. 55 reported an incidence of elevated GAD-7 scores in German caregivers of people with CF comparable with the German population norms (5%) 67 and the remaining 11 studies reported incidences of high GAD-7 scores of between 14% 51 and 66%. 60 A GAD-7 score of ⩾5 is typically considered to be the cut-off for clinically significant anxiety; 68 however, Naranjo et al. 55 applied a cut-off score of ⩾10. This cut-off may explain the lower incidence of high GAD-7 scores in Naranjo et al. 55 Raised CES-D scores were reported by eight studies11,65,69 –74 and varied in incidence from 26% 70 to 54%. 70 All of these incidences were substantially greater than the 8.8% frequency of raised CES-D scores reported by a systematic review of population CES-D scores in English- or Spanish-speaking populations performed by Vilagut et al. 75
Elevated HADS-A scores were reported by four studies70,72,76,77 and ranged in incidence from 35% 76 to 62%. 70 For comparison, Hinz and Brähler 78 reported an incidence of raised scores of 21% in the German general population in 2011. Quittner 65 found that 48% and 36% of mothers and fathers who were CF caregivers had raised scores, respectively. High HADS-D scores were reported by four studies,69,70,73,79 ranging in incidence from 28.3% 73 to 37.7%. 69 For comparison, Hinz and Brähler 78 reported an occurrence of elevated HADS-D scores of 23% in the German general population in 2011. Modi et al. 76 reported the lowest incidence of raised HADS-D scores at 10%; however, the same study also found that 35% of caregivers had HADS-A scores indicating significant anxiety and suggested that as anxiety typically proceeds depression, it may be that depressive symptoms in the patients and caregivers studied had yet to develop. 76
In addition, Suthoff et al.9,80 (2018 and 2019) reported significantly lower Short-Form Survey 12 items mental health scores during patient hospitalization than when the patient had returned to a relatively well state (p = 0.005 and 39.8 versus 42.5; p < 0.001, respectively). Five studies investigated treatment adherence in relation to caregiver anxiety and depression. Two studies found that caregiver anxiety and depression resulted in worse patient adherence to prescribed treatments11,81 and two studies reported that caregiver depression may result in improved adherence to treatment among some caregivers.82,83 One study found that increased caregiver depression and anxiety symptoms are associated with significantly higher patient standardized body mass index (p < 0.05), 57 which may also indicate greater compliance with treatments such as enzyme supplementation. 84
Additional outcomes of interest
Patient lung function and caregiver well-being. Five studies reported data on the association between patient lung function and caregiver well-being.31,55,76,85,86 Fanous et al. 85 noted that Hispanic caregivers reported greater anxiety than non-Hispanic caregivers, and that this was associated with worse patient lung function (Mean GAD-7: 6.88 versus 3.54; p = 0.05). Keniş Coşkun et al. 31 reported a correlation between lower patient forced expiratory volume in 1 s (FEV1) and greater subjective caregiver burden in their caregivers. Modi et al. 76 and Naranjo et al. 55 both reported an association between worse patient lung function and more frequent depressive symptoms in caregivers. Two additional studies reported related outcomes.87,88
Sleep quality. Six studies reported data on caregiver sleep quality.21,77,87,89 –91 These data showed that caregivers of people with CF experience suboptimal sleep duration and poor sleep quality, which in turn lead to a worsening of perceived caregiver burden. A summary of the sleep quality data reported by included studies can be found in Supplementary Table S6.
Additional data on lung function55,76,85,88 and its association with caregiver well-being and on the well-being of healthy siblings 92 are presented in Supplementary Tables S7 and S8, respectively.
Economic caregiver burden and occupational impact
Seventeen studies reported data relevant to the economic burden of caring for a person with CF.9,17 –25,93 –99 Costs to caregivers varied significantly across countries, which in part reflects differences in average hourly wage between countries.
The direct, non-healthcare costs of caregiver time reported in the included studies is shown in Figure 4. The BURQOL-RD European study investigated hours spent on caregiving tasks per week and associated costs. 24 Caregivers of pediatric patients spent differing amounts of time on care tasks in different countries; for example, French caregivers spent a mean of 37.6 hours per week on caregiving tasks, whereas Bulgarian caregivers spent 109.3 hours. When valued using the proxy good method (which calculates the cost of replacing hours of informal care with paid help), 24 this time was valued at €6,704 in France and €15,686 in Bulgaria. The highest cost was reported for Swedish caregivers of adult patients at €31,049. 24 While the number of hours spent caring for adults highest on average in Sweden (71 hours per week), the large difference in costs of caring compared with other countries is largely driven by differences in average wage costs. In addition, it should also be noted that the Swedish figure is based on data from only one caregiver. 24

Estimated cost of time spent on care-related tasks by caregivers valued by proxy good method (€; mean) stratified by patient age group. Figures for caregivers of adult patients and pediatric patients are subsets of the adult and pediatric patients (combined) data; figure for adult and pediatric patients (combined) is reported as published in the source, not calculated by review authors.
The BURQOL-RD study reported that, overall, caregivers of adults with CF had significantly higher direct care costs than those of pediatric patients with CF (p < 0.0001), but that carers of pediatric patients had significantly higher informal care costs (p < 0.0001). 24 The data showed that a higher number of caregiving hours was associated with higher costs, with caregivers of pediatric patients spending significantly more time on caregiving tasks. This is likely due to greater patient dependency on caregivers for assistance with both elementary tasks, such as feeding and bathing, and treatment-related activities.
Six studies reported data on the occupational impact of caregiving.18,19,22,25,96,99 When reported, the occupational data showed that caregiving responsibilities resulted in substantial impacts on caregivers’ occupational lives, with caregivers reporting reduced employment overall, reductions in working hours, and substantial losses in productivity during periods of patient hospitalization. Key data on employment, productivity, and absenteeism are reported below, and additional results are shown in Table 2.18,19,25,99
Key economic outcomes from included studies (caregiver productivity, employment, and absenteeism data).

CF, cystic fibrosis.
In the study by Johnson et al., 96 pulmonary exacerbation events were shown to be associated with greater absenteeism from the workplace. Caregivers of people with CF treated as an inpatient over the 12-month study period claimed an average of 100 absenteeism hours, whereas caregivers of people treated only as an outpatient claimed 77 hours on average. 96 Suthoff et al. 9 found that caregiver absenteeism increased by 30.1% (p < 0.001), productivity fell by 32.8% (p < 0.001), and presenteeism fell by 22.2% (p = 0.003) in the time between patient hospitalization with an exacerbation and the patient returning to a ‘well’ state. Neri et al. 21 reported that caregivers with a very mild caregiver burden had a mean of 0.82 days of reduced working hours due to CF-related childcare in the preceding 30 days, whereas those who reported a very severe caregiver burden (indicating a worse severity of their child’s CF) had a mean of 5.54 days of reduced hours.
Additional economic outcomes were out-of-pocket expenses (reported by two studies9,94), food insecurity (reported by two studies93,98), and social barriers to care (reported by one study 20 ). Key data from these studies are presented below; additional data can be found in Supplementary Table S9.
Suthoff et al. 9 reported a mean out-of-pocket cost to caregivers of pediatric patients of US$2,126 per year. Such costs can be an issue for the families of people with CF: 31% of caregivers surveyed in a 2019 study by Krivchenia et al. 20 cited inadequate income as a barrier to accessing healthcare. Wojtaszcyzk et al. 99 found that full-time employment of adults with CF was associated with lower caregiver burden, regardless of patients’ FEV1, suggesting that while the financial strain of caregiving continues into adulthood, it may be partially ameliorated by the additional income and other benefits associated with patient employment.
Discussion
Informal caregivers of people with chronic conditions, including CF, provide a significant service to society, valued at £132 billion per year in the United Kingdom alone when compared with the cost of providing alternative, professional care. 100 Caregivers perform this role in spite of the significant personal and professional limitations that arise due to their caring responsibilities, such as a reduction in free time due to caregiving tasks and loss of income due to occupational adjustments made to accommodate caregiving. These impacts, combined with other associated issues arising from caregiving such as reported caregiver strain, increased prevalence of affective disorders, and lower sleep quality, result in significant costs to society as a whole, including a loss in caregiver workplace productivity and the cost of supporting individuals suffering from conditions that arose due to their caregiving role. 101 A recent study valued these resultant costs at £24–37 billion per year to the UK economy. 102
The literature identified in this systematic literature review shows that caregiving to people with CF has a wide-ranging impact on caregivers’ QoL, particularly for caregivers of pediatric patients. Caregivers of pediatric patients reported substantially greater perceived burden than those caring for adults, 24 and overall utility scores were found to be lower in caregivers of pediatric patients with CF (disease duration 0–9 years) than of adolescents (disease duration 10–19 years) or adults (disease duration 20–29 years24,30). This reflects the substantial treatment burden associated with time-consuming prophylactic treatments such as airway clearance physiotherapy. A greater number of caregiving hours was associated with greater perceived burden 24 and parents of younger people with CF are generally required to perform or supervise these treatments more than caregivers of adolescents or adults, who typically assume more responsibility for their own treatment. In caregivers of patients with a disease duration of ⩾ 30 years, however, the mean utility scores were lower than in any other cohort of caregivers. 30 Caregivers may adapt to the demands of caregiving until the later stages of the disease when patients are again more dependent on their caregivers’ support and more informal hours of caregiving are required, resulting in the low utility reported in the patients with the longest disease duration.
While the evidence identified by the systematic literature review demonstrates there was variation between countries in the magnitude of the effect of caregiving of people with CF, an impact was demonstrated on health-related QoL in all countries. The utility scores associated with QoL of CF caregivers were shown to be lower than those measured in the general population; for instance, the mean utility score for caregivers of pediatric patients with CF in Germany 24 was 5.8% less than German population norms, 103 and mean utility scores for caregivers of pediatric patients with CF in the United Kingdom were reported to be between 8.1% 17 and 9.7% 30 lower than UK norms. 17 This detriment in caregiver utility and VAS scores appears to be mediated by patient disease severity, with lower scores reported by the caregivers of more dependent patients and of patients with longer disease, 24 who typically have a greater disease severity due to the progressive nature of CF. 104 Other markers of greater disease severity, including infection with P. aeruginosa bacteria, also result in a significant drop in caregiver utility values, likely related to the need for a more intense treatment regimen. 19 In addition, acute events such as hospitalizations resulted in increased caregiver perception of burden. 9 Children with siblings having CF also reported worse well-being scores when their sibling had a history of P. aeruginosa infection or hospitalization. 92
The high incidence of anxiety and depression reported by the identified studies was significant, with up to 66% of caregivers reporting elevated symptoms. 60 This is likely due to an amalgamation of issues experienced by this group: the emotional impact of caring for an individual with a progressive, life-limiting illness; financial concerns caused by the additional out-of-pocket expenses and occupational limitations; and the time impact of performing associated care tasks. For context, the incidence of these symptoms in this caregiver cohort is comparable with the 63.5% and 34% incidences of elevated anxiety and depression symptoms, respectively, reported by caregivers of patients with chronic obstructive pulmonary disease (COPD). 105 Worsening of CF indicated by reductions in ppFEV1 has been shown to result in increased symptoms of anxiety and depression in caregivers,55,61,76 as have reductions in patient body mass index. 61 This relationship between disease severity and caregiver well-being is also seen in COPD, with worsening disease severity resulting in more severe anxiety and depression among caregivers. 106 Hospitalization of people with CF due to disease exacerbations has also been shown to have a significant impact on caregiver mental health, with maternal mental illness linked to inpatient stays.9,18 Novel treatments, such as CF transmembrane conductance regulator modulators, could provide a means of breaking this cycle by delaying disease progression and reducing the frequency of CF-related hospitalizations.
The available data suggest that caregiver anxiety and depression and disease severity may interact in a bi-directional manner: disease progression results in higher caregiver anxiety and depression, and more depressed and anxious parents adhere less to prescribed treatments, leading to worse disease severity in the patient. Children of anxious caregivers were shown to be significantly less adherent to dornase alfa treatment than those of nonanxious caregivers, which resulted in reduced weight gain by patients over the study period.11,81 It is plausible that the time demands of adhering to these treatments can lead to caregiver ‘burnout’ and increased anxiety and depression, reducing treatment adherence. However, this may not be the case for all parents, as in one study maternal depressive symptoms were associated with better adherence to airway clearance treatment in adolescents, 83 indicating that other factors may also be impacting on treatment adherence.
Caregiving also results in caregiver productivity loss, causing a significant increase in absenteeism from the workplace. 9 CF has a particularly acute occupational impact during periods of disease exacerbation, leading to a 32.8% loss in caregiver productivity, 9 in part, due to the additional leave that caregivers need to take from work during exacerbation events. 96 In addition to taking more leave, caregiving results in caregivers changing their job role or working schedule to better accommodate their caregiving responsibilities. 21 This loss in productive time is impacted on by a caregiver’s perception of their patient’s disease severity, with caregivers citing a very severe caregiving burden reporting significantly more days of reduced working hours than those with a very mild burden. 21 Hence, interventions to address the specific needs of this group of caregivers could lead to substantial gains in productivity.
Strengths and limitations
The broad scope of this systematic literature review allowed the inclusion of 72 studies, which reported outcomes covering many aspects of caregiver burden. A total of 32 studies reported data on caregiver depression and anxiety; an evaluation and summary of these data is valuable, and will improve the understanding of the mental health impacts of caregiving for clinicians and decision makers.
Limitations of the review arise from the type of studies available, with a lack of longitudinal studies and a dependence on observational studies. The paucity of longitudinal studies in this area has previously been highlighted by Angelis et al. 17 This is a significant limitation, as the chronic nature of CF means that caregivers are likely to adapt to their role over time, and observational studies are likely to miss the short-term effects of events like disease exacerbations and initial diagnosis on caregiver well-being. In addition, 49 of the studies included in this systematic literature review were conference abstracts, which report limited information on study populations and measures utilized, restricting the conclusions that can be drawn from the data. Only 21 of the patient-reported outcome measures included in the review were explicitly reported as having been validated in at least one study. However, many of the included measures, such as the ZBS, EQ-5D, and the World Health Organization Quality of Life: Brief Version (WHOQOL-BREF), are widely researched and used. Therefore, this is likely, at least in part, to be an issue of reporting and does not preclude that many of the included instruments are validated measures. The lack of data on general population scores for measures such as the EQ-5D-5 L makes it challenging to identify the specific impact of caregiving using this measure. For instance, the BURQOL-RD study investigated caregiver well-being in Bulgaria using the EQ-5D, however, as no reference data were available for the Bulgarian population, the investigators used the UK value set. 24
Future directions
This systematic literature review highlights the lack of longitudinal studies of caregiver burden in CF. More cross-sectional and longitudinal studies would better elucidate the connection between disease severity and caregiver QoL.
Traditionally, the value of potential new treatments has been assessed based almost exclusively on their direct benefits to patients; however, the full benefit of a therapy cannot be understood unless the impact on other parties, including the caregivers, is also considered. Further research into the QoL of caregivers of people with chronic diseases would help better quantify the impact of these disorders beyond the patient, and allow decision-making bodies to more accurately determine the overall merit of novel therapeutic agents.
This review also demonstrates the lack of population utility values and VAS scores available for certain populations. The collection of these data from the general populations of further countries would be beneficial in determining caregiver burden across a number of chronic conditions, including CF.
Conclusion
This systematic literature review brings into focus the consequences of caregiving to people with CF, with caregivers bearing a reduced health-related QoL and significant risk of anxiety and depression due to their role. These can lead to a cycle of decreased patient adherence to treatment regimens, which results in increased disease exacerbations and disease progression that further increase patient dependency on caregivers, in turn leading to diminished caregiver QoL. Economic impacts on families arise from reductions in working hours to accommodate caregiving responsibilities, reduced career progression, and greater absenteeism from the workplace. These impacts, coupled with the increased out-of-pocket expenditure associated with caring for an individual with a chronic illness, result in financial burden for families and a significant cost to society as a whole due to lost productivity. This review has highlighted the significant burden of CF on caregivers and their families; however, important data gaps have been identified requiring further research on the impact of novel treatments, such as CF transmembrane conductance regulator modulators, on the caregiver burden.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221086416 – Supplemental material for Caregiver burden in cystic fibrosis: a systematic literature review
Supplemental material, sj-docx-1-tar-10.1177_17534666221086416 for Caregiver burden in cystic fibrosis: a systematic literature review by Conor Daly, Philip Ruane, Karl O’Reilly, Louise Longworth and Gabriela Vega-Hernandez in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666221086416 – Supplemental material for Caregiver burden in cystic fibrosis: a systematic literature review
Supplemental material, sj-docx-2-tar-10.1177_17534666221086416 for Caregiver burden in cystic fibrosis: a systematic literature review by Conor Daly, Philip Ruane, Karl O’Reilly, Louise Longworth and Gabriela Vega-Hernandez in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-1-tar-10.1177_17534666221086416 – Supplemental material for Caregiver burden in cystic fibrosis: a systematic literature review
Supplemental material, sj-pdf-1-tar-10.1177_17534666221086416 for Caregiver burden in cystic fibrosis: a systematic literature review by Conor Daly, Philip Ruane, Karl O’Reilly, Louise Longworth and Gabriela Vega-Hernandez in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Editorial coordination and support were provided by Francesca Francois, PharmD, MPH, who is an employee of Vertex Pharmaceuticals Incorporated and may own stock or stock options in that company. Project management support was provided by Matilda Toivakka, PhD, and editing support was provided by Adam Paton, BA, of Complete HealthVizion, McCann Health Medical Communications, funded by Vertex Pharmaceuticals Incorporated.
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CD, GV-H, and KO’R are employees of Vertex Pharmaceuticals (Europe) Limited and may hold stock or stock options in the company. PR and LL are employed by PHMR, an independent research company that provides consulting and other research services to pharmaceutical, medical device, and related organizations. In their salaried positions, they work with a variety of companies and are precluded from receiving payment or honoraria directly from these organizations for services rendered. PHMR received payment from Vertex Pharmaceuticals Incorporated for the conduct of this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Vertex Pharmaceuticals Incorporated.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.