
Abstract
Background:
The factors that trigger spontaneous pneumothorax have not been sufficiently evaluated. The purpose of this study is to analyze the relationship between the development of spontaneous pneumothorax and meteorological parameters, including air pollutants.
Methods:
This is a retrospective study using the medical records of 379 patients who were admitted for spontaneous pneumothorax (SP) over a period of 4 years. Meteorological and air pollution data were obtained from the National Meteorological Office and the Ministry of Environment. We employed a case-crossover design to evaluate the short-term association between SP and meteorological factors including air pollutants. Conditional logistic regression was used to analyze bi-directional matched data.
Results:
Increase of relative humidity (RH) and of carbon monoxide (CO) were associated with the risk of pneumothorax, with odds ratio (OR) for RH = 1.18 (1.02–1.36), CO = 1.23 (1.02–1.48). Moreover, as air pressure (AP) decreased, risk of pneumothorax increased, with OR = 1.30 (1.05–1.59) but others did not. In the stratified analysis, the effect of RH was positive in ex-smokers (OR = 3.31) and non-smokers (OR = 1.32), but negative in current smokers (OR = 0.72). The effect of AP was significant in younger patients (OR = 1.33), males (OR = 1.40), and non-smokers (OR = 1.36). CO was related only with non-smokers (OR = 1.35)
Conclusion:
The triggering factors for spontaneous pneumothorax were relative humidity, carbon monoxide, and air pressure. The effect of the trigger was prominent in patients who were younger (<45 years), non- or ex-smokers, and male.
The reviews of this paper are available via the supplemental material section.
Background
Spontaneous pneumothorax (SP) is an irritating disease with sudden onset and frequent recurrence. Therefore, SP can decrease health related quality of life. 1 Various factors are known to be related to the development or recurrence of pneumothorax. Previous reports regarded smoking as a strong risk factor for spontaneous pneumothorax.2,3 In addition, emphysematous change of the lung, pulmonary fibrosis, male gender, and smoking have been regarded as risk factors for recurrence.4–7 Because most of these are pre-existing factors, however, patients cannot make any efforts to prevent occurrence or recurrence, except to quit smoking. Moreover, non-smoking patients or those without pulmonary disease have no effective methods to avoid pneumothorax. Therefore, it is important to discover avoidable factors that could provoke pneumothorax.
Clustering of spontaneous pneumothorax in specific meteorological conditions has been reported in some studies.8,9 Therefore, certain environmental factors, including air pressure, humidity, and temperature, were investigated to evaluate a possible close relationship with the development of spontaneous pneumothorax.8,10,11 Air pollutants have also been suggested to be possible triggering factors of pneumothorax. 9 However, studies that simultaneously analyze smoking, the most powerful causative factor of pneumothorax, and the above-mentioned environmental factors are few.
Therefore, the purpose of this study was to investigate the relationship between the development of SP and meteorological parameters, including air pollutants, and to stratify them according to smoking status (current-, ex-, and non-smokers) to determine the specific effect of smoking on pneumothorax development.
Methods
Study population
A total of 440 SP or pneumomediastinum patients were admitted at Chungbuk National University Hospital from February 2013 to February 2017. Chungbuk National University Hospital is the only university-based hospital in the city of Cheongju, a middle-sized city with a population of approximately 800,000 people located in the center of the Korean peninsula. The size of the city is 940.33 km2, and the population density is 905.2 person/km2. Participants’ demographic factors (such as age, gender, and address), potential risk factors (such as smoking status and cumulative smoking amount), and underlying disease status were collected through medical records review. All patients were diagnosed with pneumothorax through chest X-ray or computed tomography (CT) scan. Patients who were diagnosed with pneumomediastinum (n = 19) and those who had been treated for underlying pulmonary diseases such as chronic obstructive pulmonary disease (n = 26), asthma (n = 8), tuberculosis (n = 7), and pneumoconiosis (n = 1) were excluded. Finally, a total of 379 SP patients were enrolled in the study (Figure 1). This study was approved by the Institutional Review Board of Chungbuk National University Hospital, Korea (IRB No. 2017-03-006-001).

Flow chart of study population. Spontaneous pneumomediastinum was excluded in the study and patients with respiratory disease were not included in the study. Finally, 379 patients of spontaneous pneumothorax without respiratory disease were determined as study sample.
Meteorological data and air pollution data
Meteorological data such as temperature, relative humidity (RH), and air pressure (AP) between 1 February 2013 and 28 February 2017 were obtained from the National Meteorological Office in Korea. Air pollution data for ozone (O3), carbon monoxide (CO), nitric oxide (NO2), sulfur dioxide (SO2), and particulate matter 10 (PM10) over the same period were obtained from the Ministry of Environment in Korea. The daily mean and maximum values were determined for each meteorological factor and air pollutant.
Statistical analysis
We employed a case-crossover design to evaluate the short-term association between SP incidence and meteorological factors, including air pollutant levels. The case-crossover design is very similar to the traditional matched-pair case–control design and features the patient themself becoming his or her own control. 12 We defined case day as the day of SP symptom onset and selected bi-directional matched control days for the case day. In other words, the control days were 14 days before and after the case day (lag day 0). Days 1 (lag day 1) to 7 (lag day 7) prior to the onset of SP symptom were also considered as the case day to evaluate the lag effect of meteorological factors and air pollutants on SP. Conditional logistic regression was used to analyze the bi-directional matched data. Odds ratios (ORs) by one standard deviation decrease (for AP) or increase (for the other meteorological factors and air pollutants) in daily mean or maximum levels are presented with their 95% confidence intervals (CIs). To assess the influence of age, sex, and smoking status, a subgroup analysis was performed. The Benjamini–Hochberg procedure was performed for multiple test comparison correction, and false discovery rate-adjusted p values were suggested. All statistical analyses were conducted using SPSS version 23.0 (IBM, Armonk, NY, USA).
Results
The average age of the 379 SP patients was 31 years. About 40% of the SP patients were under 20 years of age. Of the 379 SP patients, 317 patients (83.6%) were male and 260 patients (68.6%) were never-smokers. The incidence of SP was evenly distributed throughout the four seasons (Table 1). The distributions of daily mean or maximum levels of meteorological factors and air pollutants in Cheongju during the study period are shown in Table 2. The average daily temperature, RH, and AP during the study period were 13.3ºC, 61.2%, and 1009.8 hPa, respectively. The daily means for SO2, O3, NO2, CO, and PM10 were 3.8 ppb, 26.1 ppb, 19.6 ppb, 0.5 ppm, and 49.3 μg/m3, respectively. There were significant correlations among the meteorological factors and air pollutants, excluding the correlation between O3 and PM10 (Table 3).
General characteristics of study subjects.

Distribution of meteorological factors and air pollutants levels in Cheong-ju (1 February 2013–28 February 2017).
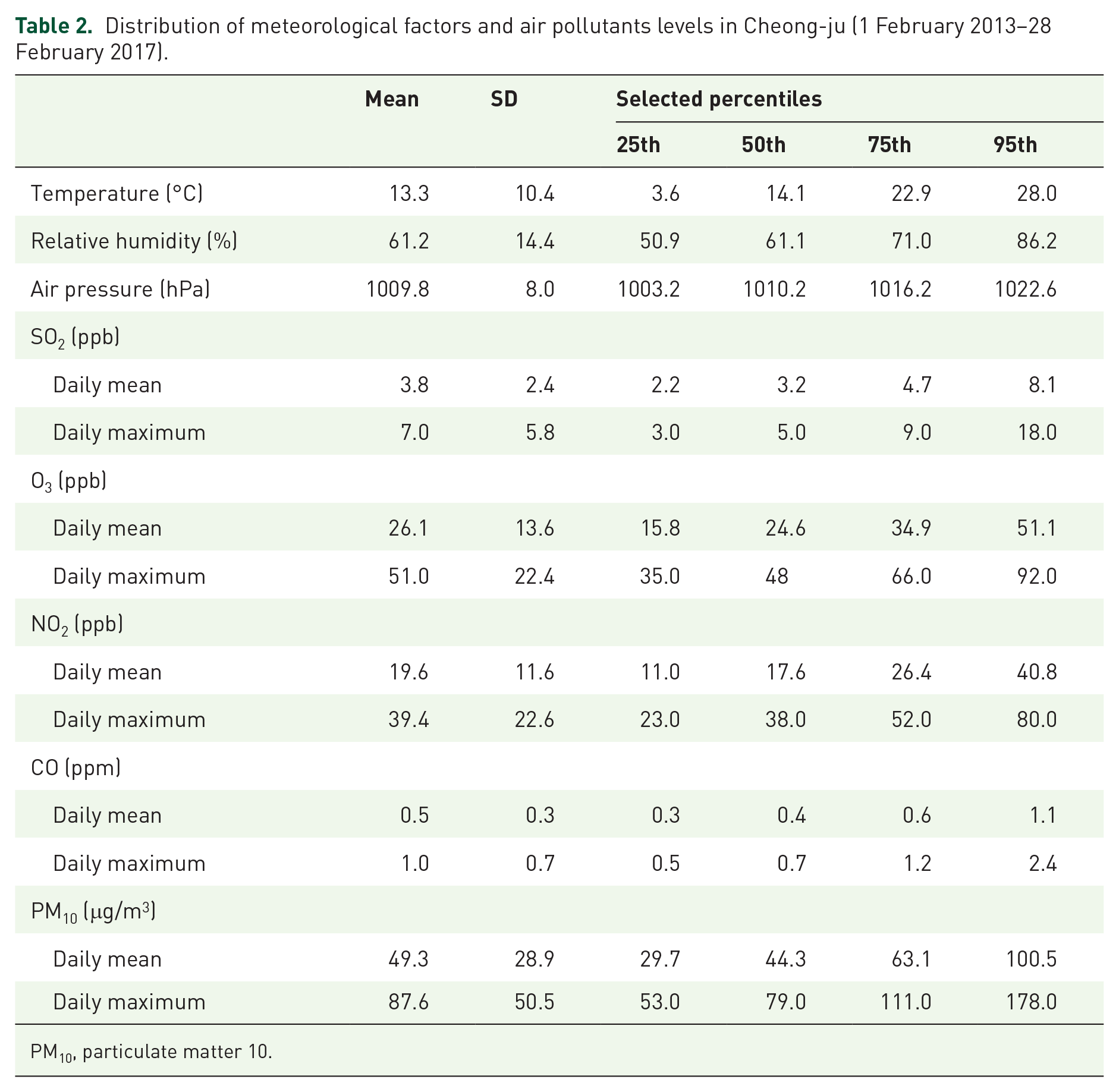
PM10, particulate matter 10.
Spearman rank correlation coefficients among meteorological factors and air pollutant levels.

p < 0.01.
AP, air pressure; PM10, particulate matter 10; RH, relative humidity.
Table 4 presents the association between meteorological factors and air pollutant levels on different lag days and SP incidence. One standard deviation (SD) increase in daily mean RH and CO on lag day 0 (the day of pneumothorax development) was significantly associated with an increased risk of pneumothorax [OR (95% CI) for RH = 1.18 (1.02–1.36) and OR (95% CI) for CO = 1.23 (1.02–1.48)]. We also found a positive association for SD decrease in AP on lag day 0 (OR = 1.30, 95% CI = 1.05–1.59). However, the significant association of these three indicators disappeared after correcting for multiple comparisons. Temperature, SO2, O3, nitrogen dioxide, and particulate matter were not associated with pneumothorax incidence. In the analysis using the daily maximum value of air pollutants, significant association between CO on lag day 0 and the occurrence of SP were observed and remained noteworthy after correcting for multiple comparisons (OR = 1.31, 95% CI = 1.08–1.59) (Table 5). After controlling for meteorological variables such as RH and AP, the daily mean and maximum of CO on lag day 0 showed a consistently positive association with the risk of SP (Figure 2).
Odds ratios and 95% confidence intervals for association between the incidence of pneumothorax and daily mean of meteorological factors and air pollutant levels.

p < 0.05; odds ratios were calculated for a one standard deviation decrease (for air pressure) or increase (for the others) in
AP, air pressure; PM10, particulate matter 10; RH, relative humidity
Odds ratios and 95% confidence intervals for association between the incidence of pneumothorax and daily maximum of air pollutants levels.

p < 0.05.
p < 0.01; odds ratios were calculated for a one standard deviation increase in daily maximum of air pollutant levels on different lag days.
AP, air pressure; PM10, particulate matter 10; RH, relative humidity
The bold indicates significant values statistically.

Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) of the incidence of pneumothorax per one standard deviation increase in daily mean (A) or maximum (B) of carbon monoxide level in different lags. ORs adjusted for relative humidity and air pressure. Error bars represent 95% CIs.
In subgroup analyses according to age, sex, and smoking, RH and AP were significantly associated with risk of pneumothorax only in patients under 45 years of age. AP was significantly associated with the risk of pneumothorax in men but not in women. The effect of RH was strongest in ex-smokers (OR = 3.31, 95% CI = 1.23–8.90), whereas CO was significantly associated with a risk of pneumothorax only in non-smokers (OR = 1.35, 95% CI = 1.08–1.70) (Table 6).
Association between the incidence of pneumothorax and daily mean of relative humidity, air pressure and carbon monoxide levels by age group, sex, and smoking status.

Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for a one standard deviation decrease (for air pressure) or increase (for the others) in daily mean of meteorological factors and air pollutants levels in lag 0 days.
Discussion
This study is unique because both environmental factors and smoking status were simultaneously analyzed as possible causative factors of SP. RH, AP, and CO could influence the development of spontaneous pneumothorax, and the effect differed according to smoking status. Therefore, different guidelines that vary according to smoking status are required to maintain health-related quality of life (HRQOL) in SP patients. For example, an ex-smoker may consider avoiding exposure to high humidity conditions, such as just before rain. In the case of a non-smoker, reducing access to outside air may help prevent pneumothorax if cloudiness and air pollution are expected.
This study revealed that decreased AP may be related with the development of SP. Usually, bullae in the lungs of patients with SP are isolated from the surrounding lung tissue by the check valve mechanism, so the volume of air in the bullae will increase if the AP decreases according to Boyle–Marriot’s law (pressure × volume = constant). This could explain why changes in AP could provoke pneumothorax.8,10,13,14 RH has also been indicated as a triggering factor of pneumothorax in other studies.8,15 In this study, decrease in RH on the day of pneumothorax was related with SP development. Unlike humidity, increase in CO was ascertained to be associated with pneumothorax in this study, and other studies have suggested that air pollutants could influence spontaneous pneumothorax by inducing hyper-reactivity cough.9,16,17 However, these results were valid only for non- or ex-smokers, not for current smokers.
For smokers, AP and CO were not related with the development of pneumothorax. Rather, an increase in RH was negatively correlated with the occurrence of pneumothorax, and the exact mechanism by which this occurs is unknown. However, tobacco is the most potent causative factor of SP, and since the effects of tobacco are so strong,2,18 this suggests that tobacco considerably alters the effects of other factors on the development of SP. Further studies are required to determine whether the environment that promotes pneumothorax induces the opposite effect in smokers, unlike the synergistic effect when smoking is combined with drugs that promote pneumothorax, such as cannabis. 19
This study has some limitations. First, there may be selection bias due to the retrospective nature of the study. In addition, patients with SP could have visited hospitals other than this hospital. However, it could be assumed that most pneumothorax patients would visit this hospital, because this is the only university-based hospital in the city. In addition, patients with prolonged air leakage of more than a week or who are estimated to require an operation were usually transferred to this hospital from other hospitals in the city. Second, it was impossible to investigate the exact time and place when pneumothorax developed, so it was also impossible to know the exact meteorological or air pollution data in which patients existed. However, the city is not big enough to represent different meteorological or air pollution statuses. Moreover, we obtained the environmental data by collecting data from an observatory station nearest to the patient’s home, and the point of occurrence was based on the first appearance of symptoms, not the time of visit to the hospital. Therefore, the environmental data used in this research is considered to be the most similar to the actual location and time of pneumothorax patients. Finally, since this study was conducted retrospectively, the influence of uncontrolled confounding factors (i.e. genetic predisposition, CT chest evidence of bullae, and the difference of spirometry) cannot be excluded. Larger prospective studies will be needed to verify the findings of our study.
In conclusion, the triggering factors of SP were RH, CO, and AP. The trigger was prominent in younger patients (<45 years), non- or ex-smokers (not in current smokers), and males. Guidelines that consider meteorological factors and air pollution are required to achieve a HRQOL in patients susceptible to SP.
Supplemental Material
sj-pdf-1-tar-10.1177_1753466620977408 – Supplemental material for The clinical effect of smoking and environmental factors in spontaneous pneumothorax: a case-crossover study in an Inland province
Supplemental material, sj-pdf-1-tar-10.1177_1753466620977408 for The clinical effect of smoking and environmental factors in spontaneous pneumothorax: a case-crossover study in an Inland province by Dohun Kim, Sang-Yong Eom, Chang-Seob Shin, Yong-Dae Kim, Si-Wook Kim and Jong-Myeon Hong in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_1753466620977408 – Supplemental material for The clinical effect of smoking and environmental factors in spontaneous pneumothorax: a case-crossover study in an Inland province
Supplemental material, sj-pdf-2-tar-10.1177_1753466620977408 for The clinical effect of smoking and environmental factors in spontaneous pneumothorax: a case-crossover study in an Inland province by Dohun Kim, Sang-Yong Eom, Chang-Seob Shin, Yong-Dae Kim, Si-Wook Kim and Jong-Myeon Hong in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_1753466620977408 – Supplemental material for The clinical effect of smoking and environmental factors in spontaneous pneumothorax: a case-crossover study in an Inland province
Supplemental material, sj-pdf-3-tar-10.1177_1753466620977408 for The clinical effect of smoking and environmental factors in spontaneous pneumothorax: a case-crossover study in an Inland province by Dohun Kim, Sang-Yong Eom, Chang-Seob Shin, Yong-Dae Kim, Si-Wook Kim and Jong-Myeon Hong in Therapeutic Advances in Respiratory Disease
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics statement
This study was approved by the Institutional Review Board of Chungbuk National University Hospital, Korea (IRB No. 2017-03-006-001).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (2017R1C1B5015969).
Informed consent
The requirement for written informed consent was waived because all patient information was anonymized and de-identified during data recording.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.