
Abstract
A 66-year-old woman had two severe episodes of massive hemoptysis without any premonitory symptoms, with approximately 400–500 ml blood each time. Bronchoscopic exam revealed a smooth and pulsatile protrusion that was approximately 8–10 mm in diameter found at the beginning of the right middle lobe bronchus in the bronchial lumen. The protrusion arose from the surface with absolutely normal mucosa. Selective bronchial arteriography showed that elongated, tortuous, and dilated branches of the bronchial artery in the region of the middle lobe bronchus. Further bronchial arterial embolization (BAE) is recommended, although the patient currently has no active bleeding. Bronchial Dieulafoy’s disease (BDD) is a rare and life-threatening disease. Selective bronchial arteriography is a diagnostic tool to detect and locate abnormal arteries. There is no unified guideline or expert consensus on the treatment of BDD. Selective BAE or surgical resection is usually used as a first-line treatment to control hemoptysis.
The reviews of this paper are available via the supplemental material section.
Keywords
Introduction
Dieulafoy’s disease is characterized by abnormally tortuous large-caliber arteries in the submucosa that are susceptible to bleeding. This vascular malformation usually occurs in the digestive tract, and involvement of the respiratory system is rare. The pathogenesis of this disease is unclear, and most scholars believe that it is a congenital disease. 1 The main clinical manifestations of bronchial Dieulafoy’s disease (BDD) are recurrent or fatal hemoptysis. In the case of acute massive hemorrhage, arterial embolization and surgical intervention can be optimal treatment strategies.
Case presentation
A 66-year-old woman was admitted to our hospital with chest tightness and cough. There was no history of smoking. Over the past decade, she had two severe episodes of massive hemoptysis without any premonitory symptoms, with approximately 400–500 ml blood each time. After admission, the patient’s vital signs were normal with the exception of oxygen saturation at 86%. Physical exam revealed no wheezing or crackles. Laboratory tests were unremarkable except for hemoglobin concentration 109 g/l (normal 115–150) and D2 polymer 0.69 μg/ml (normal 0–0.5). A chest high-resolution computed tomography (HRCT) scan showed fine reticular and multiple strip-like densification shadows and a small number of nodules in both lungs. Partial atelectasis and narrowing of the bronchus in the upper left lung was observed. There was no evidence of bronchiectasis (Figure 1A). Because of the hypoxemia, a computed tomography pulmonary artery imaging (CTPA) was performed and revealed that pulmonary artery stenosis in the right lower pulmonary artery was caused by external pressure, and no pulmonary embolism was found (Figure 1B). Due to the history of two serious episodes of hemoptysis and computed tomography (CT) findings of bronchial stenosis and pulmonary atelectasis, a bronchoscopy was performed. Bronchoscopic exam revealed a smooth and pulsatile protrusion that was approximately 8–10 mm in diameter found at the beginning of the right middle lobe bronchus in the bronchial lumen. The protrusion arose from the surface with absolutely normal mucosa, without evidence of active bleeding (Figure 1C). Because of suspected vascular abnormalities of the bronchus, the bronchoscopist did not perform a biopsy. Selective bronchial arteriography was consequently performed, and showed elongated, tortuous, and dilated branches of the bronchial artery in the region of the middle lobe bronchus (Figure 1D). Further bronchial arterial embolization (BAE) was recommended, but the patient was not willing to receive further treatment considering that there was no active bleeding.
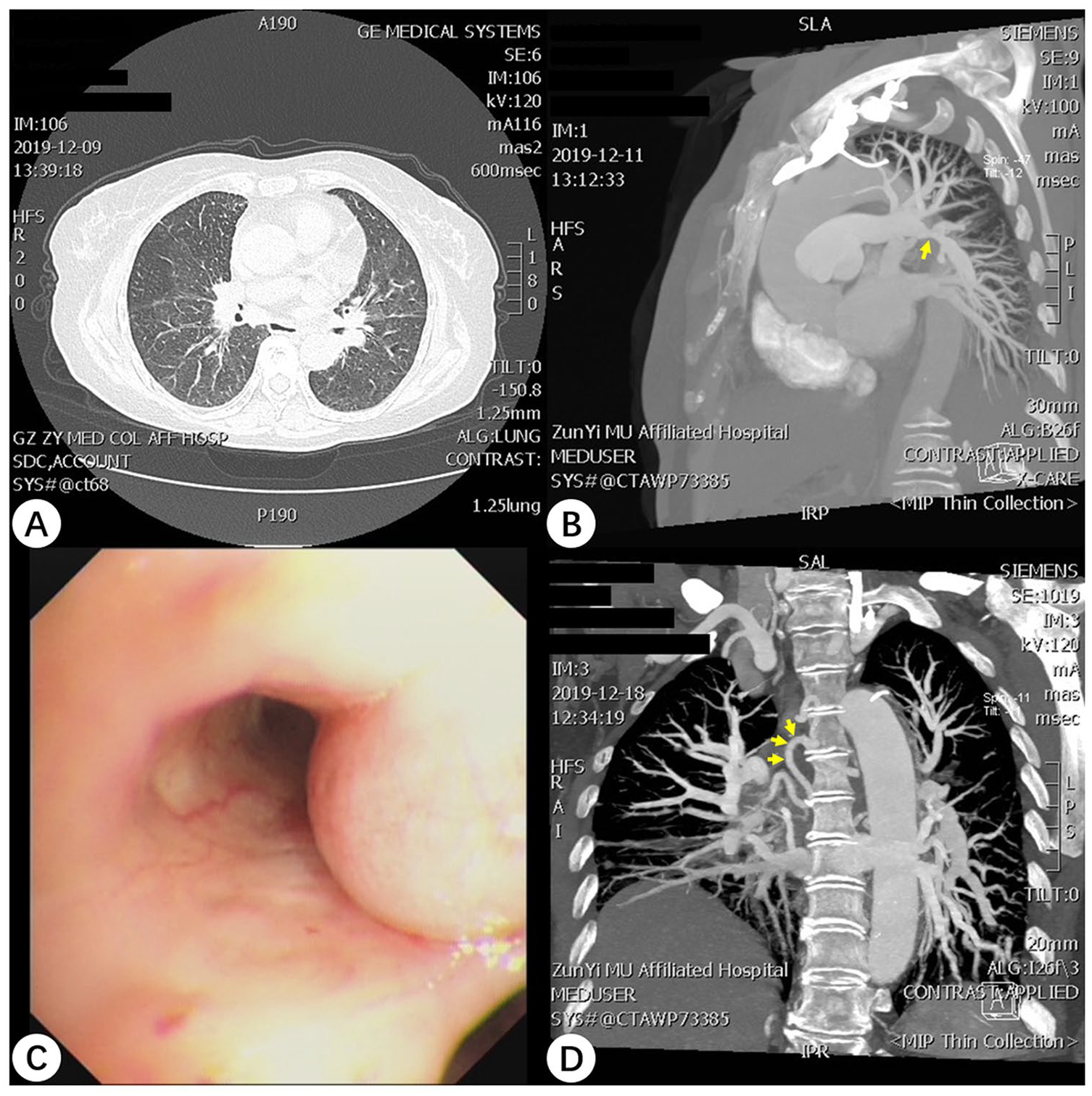
(A) HRCT scan showed interstitial lesions, multiple fibrosis and a small number of nodules in both lungs. Partial atelectasis and narrowing of the bronchus in the upper left lung were observed. No signs of bronchiectasis were found. (B) CTPA showed that the pulmonary artery stenosis in the right lower pulmonary artery was caused by external pressure, and no pulmonary embolism was found. (C) Bronchoscopy of the right lung shows smooth and pulsatile nodular lesions located in the region of the right middle lobe bronchus. The lesion arose from the surface with absolutely normal mucosa, without evidence of active bleeding. (D) CT angiography shows a right bronchial artery arising from the thoracic aorta, from which a branch supplied the pulmonary circulation, and the bronchial arteries on both sides were dilated and tortuous.
Discussion
Dieulafoy’s disease is characterized by rupture and hemorrhage of the submucosal malformed artery. This condition was initially described by the French physician Dieulafoy in 1898 and mainly occurs in the gastrointestinal tract. The bronchial variant of Dieulafoy’s disease was first reported in 1995, and it has been considered to be a rare disease.2 –4 To further understand BBD, we conducted a comprehensive search for studies on BDD in the PubMed, Web of Science and Google Scholar databases. Since the first report of BDD in 1995, a total of 73 cases of BDD have been reported domestically and internationally after excluding duplicate cases.
Pathogenesis
The pathogenesis of BDD is unclear. Most scholars believe that the disease is a congenital dysplasia. However, related case reports indicate that a large proportion of the patients had a history of smoking and other respiratory disorders, including bronchitis, bronchiectasis, asthma, chronic obstructive pulmonary disease (COPD) and tuberculosis, suggesting that the disease may be closely related to long-term smoking and chronic airway inflammation. The female-to-male ratio is approximately 1:2, and the incidence is slightly higher in middle-aged patients, indicating that sex and age are associated with the disease process.1,5
Clinical characteristics
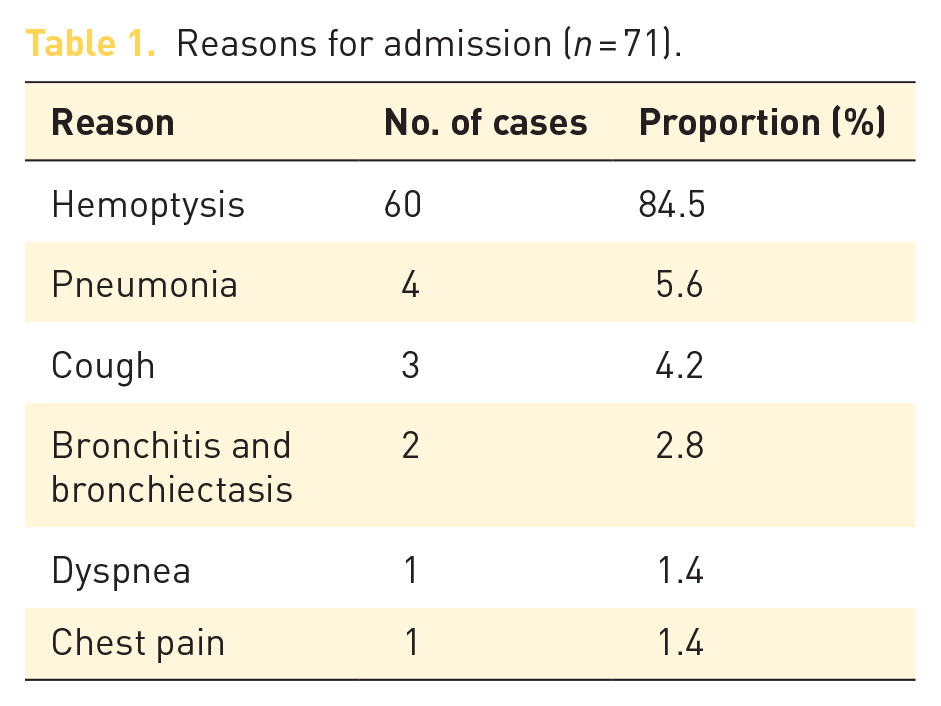
More than 70 patients were hospitalized with different respiratory symptoms and were found to have BBD during their stay. (Table 1) The typical manifestations of BDD are sudden massive hemoptysis or recurrent hemoptysis. Compared with hemoptysis, the other symptoms were relatively rare.6,7 In addition, some patients were treated for other respiratory diseases and had no previous respiratory symptoms, suggesting that BDD can be asymptomatic or cause spontaneous massive hemoptysis, similar to the patient in this case report. In addition, the abnormal lesions were most often located in the right bronchus. The ratio of lesions in the right bronchus to those in the left bronchus is approximately 2.5–1, with a few lesions located in the carina and intermediate bronchus. Therefore, we should be on high alert for unexplained right bronchial hemorrhage. 8 Unnecessary biopsy and brushing should also be avoided during bronchoscopy.
Reasons for admission (n = 71).
Diagnosis and differential diagnosis
Bronchoscopy can be used as a routine examination for this disease. Under bronchoscopy, this lesion often presents as lumen obstructed by the apophysis of normal mucosa, and some of the apophysis is covered by a white necrotic material or blood clots.5,9 The direct diameter of the diseased region is approximately 0.5–1.5 cm. Selective bronchial arteriography is a very useful diagnostic tool to detect and locate abnormal arteries. 10 CT angiography was consequently performed, and it clearly showed elongated, tortuous and dilated branches of the bronchial artery in the region of the right middle lobe bronchus. In addition, endobronchial ultrasound (EBUS) bronchoscopes with integrated probes at the distal ends usually have a Doppler mode and can be used to differentiate vascular masses from endobronchial masses, and Doppler examinations of the mucosal lesion usually showed arterial flow below the surface. 11 Since the main symptom of BDD is hemoptysis, we need to distinguish this condition from other respiratory diseases characterized by hemoptysis, such as bronchiectasis, tuberculosis, pulmonary embolism, and lung cancer. 12 As we reported in this case, the patient had two previous episodes of massive hemoptysis and was misdiagnosed with bronchiectasis in other hospitals. A high-resolution CT examination was performed after admission to our hospital, but no radiological manifestations of bronchiectasis were found. Based on laboratory tests that revealed elevated D2 polymer and associated hypoxemia, pulmonary thromboembolism could not be excluded, so CTPA was further performed, and the results showed no pulmonary embolism. Therefore, HRCT, CTPA, EBUS and enhanced CT are very useful differential examinations in the diagnosis of BDD.
Treatment of BDD
There is no unified guideline or expert consensus on the treatment of BDD to reference. 13 At present, individualized programs are formulated mainly according to the patient’s condition, and the commonly used methods include conservative treatment, BAE and surgical resection (Table 2). In addition, recent reports have shown that argon plasma coagulation by bronchoscopy has also achieved good results. 14 This patient chose to forgo further treatment because there was no active bleeding. However, based on the review of 73 cases, the majority of patients with active bleeding were treated with BAE or surgical treatment, and the results of treatment were satisfactory. In most cases, selective BAE was a safe and effective method to control hemoptysis. This procedure provides an alternative to lobectomy for patients who wish to maintain good pulmonary function or who do not wish to undergo surgery, and has shown good results.2,15 Nevertheless, some patients who underwent BAE had recurrent hemoptysis and finally opted for lobectomy to achieve a curative effect. Therefore, lobectomy may be the preferred treatment for patients with repeated massive hemoptysis or if vascular embolization is unsatisfactory.
Treatment and outcomes (n = 55).

Conclusion
In summary, BDD is a rare vascular anomaly and is extremely rare in the bronchial tree. Our reported case and those reviewed support that patients presenting with recurrent and unexplained hemoptysis should be considered for BDD. BDD is located mostly in the right bronchus, and abnormal bronchial arteries are the main source of hemorrhage. Under bronchoscopy, when the lesion is found to protrude into the bronchial lumen and the mucosal surface of the lesion is smooth, it is necessary to be aware of the possibility of BDD and avoid invasive examinations, such as a blind bronchoscopy with biopsy. Selective bronchial arteriography and bronchial endoscopic ultrasonography are feasible to confirm the diagnosis. Once the disease is diagnosed, and, if the patient has active bleeding, BAE should be performed as soon as possible. In uncontrolled cases or following BAE failure, standard anatomical lung resection is a lifesaving method that can eliminate recurrent hemoptysis.
Supplemental Material
Author_Response_1 – Supplemental material for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease
Supplemental material, Author_Response_1 for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease by Shi-xia Liao, Peng-peng Sun, Bang-guo Li, Shuang-fei He, Mao-mao Liu and Yao Ou-Yang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease
Supplemental material, Reviewer_1_v.1 for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease by Shi-xia Liao, Peng-peng Sun, Bang-guo Li, Shuang-fei He, Mao-mao Liu and Yao Ou-Yang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease
Supplemental material, Reviewer_2_v.1 for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease by Shi-xia Liao, Peng-peng Sun, Bang-guo Li, Shuang-fei He, Mao-mao Liu and Yao Ou-Yang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_3_v.1 – Supplemental material for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease
Supplemental material, Reviewer_3_v.1 for A rare and fatal respiratory disease: bronchial Dieulafoy’s disease by Shi-xia Liao, Peng-peng Sun, Bang-guo Li, Shuang-fei He, Mao-mao Liu and Yao Ou-Yang in Therapeutic Advances in Respiratory Disease
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.