
Abstract
Background:
Non-small cell lung cancer (NSCLC) accounts for approximately 80% of diagnosed lung cancer patients. RAD52 has been reported to be associated with the development of squamous cell lung carcinoma. In this study, we assessed the relationships of RAD52 genetic polymorphisms and NSCLC risk among the Chinese population at high altitude.
Methods:
Eight single nucleotide polymorphisms (SNPs) of RAD52 were genotyped in the Agena MassARRAY platform among 506 NSCLC patients and 510 healthy controls. We examined the association of RAD52 polymorphisms with NSCLC risk using odds ratios (ORs) and 95% confidence intervals (CIs) via multiple genetic models.
Results:
The rs10774474 A allele was related to a decreased risk of NSCLC in a high altitude population of China (OR = 0.82, 95% CI = 0.69–0.98, p = 0.032), whereas mutant alleles of rs1051672, rs7310449, rs1051669, rs6413436, rs4766377 and rs10849605 significantly increased NSCLC risk. Haplotype analysis showed that four haplotypes of RAD52 polymorphisms conferred an enhanced susceptibility to NSCLC (Ars1051672Grs7310449Trs1051669Ars6413436: OR = 1.29, p = 0.021; Grs1051672Ars7310449Crs1051669Grs6413436: OR = 1.21, p = 0.027; Grs4766377Crs12822733Trs10774474Crs10849605: OR = 1.26, p = 0.032; Ars4766377Crs12822733Ars10774474Trs10849605: OR = 1.21, p = 0.032).
Conclusions:
Our findings suggested the remarkable association of RAD52 polymorphisms with NSCLC risk among the Chinese population in a high altitude area.
The reviews of this paper are available via the supplemental material section.
Introduction
Lung cancer has a high incidence and mortality in the global population, with 2.1 million new cases and 1.8 million deaths in 2018. 1 In China, the incidence and mortality of lung cancer was increasing in the past decades, which imposes a great burden on individuals and society. 2 Histological classification distinguishes non-small cell lung cancer (NSCLC) from small cell lung cancer (SCLC), and NSCLC is mainly composed of adenocarcinoma and squamous cell cancer. 3 It has been reported that NSCLC accounts for approximately 80% of cases of lung cancer with a low 5-year survival rate. 4 The pathogenesis of NSCLC has not been fully elucidated. Although tobacco smoke exposure is a crucial etiological factor for lung cancer, 5 increasing numbers of studies have emphasized the important role of inherited genetics factors in tumor etiology.6–8 Genome-wide association studies (GWASs) in Europeans have provided three polymorphic variations at 5p15.33, 6p21.33 and 15q25.1 that could influence the susceptibility to lung cancer.9–13 In addition, three susceptibility regions at 3q28, 13q12.12 and 22q12.2 have been identified to be correlated to lung cancer based on GWAS research in Asian populations.14,15 Two rare variants on chromosome 13q (BRCA2) and 22q (CHEK2) have been found to be associated with squamous lung cancer as well. 16
As a well-known DNA repair gene, RAD52 (RAD52 homolog, DNA repair protein) is responsible for DNA double-strand break repair and homologous recombination. 17 Shi et al. detected a susceptible marker at 12p13.33 (RAD52, rs6489769) affecting the risk of squamous cell lung carcinoma in European smokers. 3 Timofeeva et al. found histology-specific effects of 12p13.33 locus (RAD52, rs10849605) on squamous cell lung carcinoma and SCLC in Caucasians. 18 However, a study focused on a Han Chinese population did not observe any significant correlations of rs10849605 with squamous cell lung cancer or SCLC. 18 In addition, Song et al. examined the association of RAD52 polymorphisms and SCLC susceptibility in a Chinese group, and they found that rs7963551 was significantly associated with SCLC risk. 17
Although RAD52 gene variants were linked to lung cancer susceptibility, most studies were conducted in European populations. And the involvement of RAD52 single nucleotide polymorphisms (SNPs) in the development of NSCLC among the Chinese plateau population is rarely reported. An area with elevations over 1500 meters is considered as high altitude. Exposing to high altitude and hypoxia conditions, some genetic variations were assumed to be associated with NSCLC. Considering the importance of 12p13.33 RAD52 locus in lung cancer, we investigated the correlations between RAD52 genetic polymorphisms and NSCLC risk in a Chinese population from a high altitude area. Cisplatin-based doublet chemotherapy is the feasible therapy for lung cancer, we also evaluated the effect of RAD52 polymorphisms on patients’ response to cisplatin combination chemotherapy.
Materials and methods
Study participants
A total of 506 NSCLC patients (mean age: 59.80 ± 9.08 years) and 510 healthy controls (mean age: 59.80 ± 10.63 years) were recruited in our study. All patients came from the Qinghai Province Cancer Hospital and were pathologically diagnosed with NSCLC. The controls were enrolled from the physical examination center of the Qinghai Province Cancer Hospital. All of the participants were confirmed to live in the high altitude area of China. We collected the information on cases and controls, such as carcinoembryonic antigen (CEA), alpha fetoprotein (AFP) and carbohydrate antigen 50 (CA50). Tumor location, histology subtypes and lymph node metastasis status, treatment and adverse effects of cases were also recorded. Nausea and vomiting were obvious adverse responses to the therapy. Individuals without these responses were classified in the unresponsive group. Informed consents were collected from all participants before this study. Our study was approved by the Ethical Committee of the Qinghai Province Cancer Hospital and conformed to the Declaration of Helsinki.
SNP genotyping
Eight SNPs (rs1051672, rs7310449, rs1051669, rs6413436, rs4766377, rs12822733, rs10774474 and rs10849605) of the RAD52 gene were selected for genotyping. The genomics DNA was extracted from whole blood with the GoldMag-Mini Whole Blood Genomic DNA Purification Kit (GoldMag Co. Ltd., Xi’an City, China). Concentration of the purified DNA was detected by Nanodrop 2000 (Thermo Fisher Scientific, USA). The on-line software (https://agenacx.com/online-tools/) was used to design genotyping primers (Supplementary Table 1). The Agena MassARRAY platform (Agena Bioscience, SanDiego, CA, USA) and Agena Bioscience Typer 4.0 were applied for SNP genotyping and data analysis, respectively.
Statistical analysis
And exact test was carried out to confirm the compliance of SNP allele frequency with Hardy–Weinberg equilibrium (HWE). 19 The genotype and allele distributions were compared between the case and control groups by chi-square test. Associations of variations with individual NSCLC susceptibility, clinical characteristics and cisplatin combination chemotherapy response were examined using a logistic regression model. PLINK 1.07 software was used to calculate odds ratios (ORs) with 95% confidence intervals (95% CIs) by logistic regression analysis. Haploview v.4.2 was used for linkage disequilibrium analysis and haplotype construction.20,21
Results
We present the characteristics of 506 patients with NSCLC and 510 controls from a Chinese high altitude area in Table 1. There was no significant difference in the distributions of age and gender between cases and controls (p > 0.05). The total number of individuals of stages I–II and stages III–IV groups were 93 and 286, respectively. We found significant differences in the quantity of crucial clinical markers (CEA, AFP, CA50) between cases and controls (p < 0.001). Some patients were treated by chemotherapy based on cisplatin, and we detected their responses to the treatment and toxic side effects. Among them, 42 NSCLC patients showed an obvious positive response, whereas 100 NSCLC patients did not. In terms of toxic side effects, there were 37 cases with severe effects and 152 patients with no effect.
The basic information on cases and controls.

AFP, alpha fetoprotein; BMI, body mass index; CA50, carbohydrate antigen 50; CEA, carcinoembryonic antigen.
p < 0.05 indicates statistical significance.
Basic information and allele frequencies of SNPs in RAD52 between NSCLC cases and controls are shown in Table 2. HWE p values were greater than 0.05 for all of the variants, which means that they were all in accordance with HWE and the study population is in genetic equilibrium. Except rs12822733, the other seven SNPs had significant differences in allele frequency between cases and controls. Compared with rs10774474 T allele carriers, individuals carrying the A allele had a lower risk of NSCLC (OR = 0.82, 95% CI = 0.69–0.98, p = 0.032), while the mutant allele of other SNPs (rs1051672, rs7310449, rs1051669, rs6413436, rs4766377 and rs10849605) increased NSCLC risk. The rs1051672 A allele was significantly associated with an increased risk of NSCLC (OR = 1.29, 95% CI = 1.04–1.60, p = 0.021). The rs7310449 G allele carriers had a 1.23-fold elevated risk of developing NSCLC (OR = 1.23, 95% CI = 1.03–1.46, p = 0.021). The rs1051669 T allele (OR = 1.30, 95% CI = 1.05–1.62, p = 0.016), the rs6413436 A allele (OR = 1.20, 95% CI = 1.01–1.43, p = 0.042), the rs4766377 G allele (OR = 1.30, 95% CI = 1.05–1.62, p = 0.017), and the rs10849605 C allele (OR = 1.23, 95% CI = 1.01–1.48, p = 0.035) showed remarkable correlations of NSCLC susceptibility in a Chinese population from a high altitude area.
Basic information on candidate SNPs in this study.

95% CI, 95% confidential interval; A/B, minor/major alleles on the control sample frequencies; MAF, minor allele frequency; HWE, Hardy–Weinberg equilibrium; OR, odds ratio; SNP, single nucleotide polymorphism.
HWE-p was used to assess whether the study population is in genetic equilibrium, p value was to show the allele difference between cases and controls.
p < 0.05 indicates statistical significance.
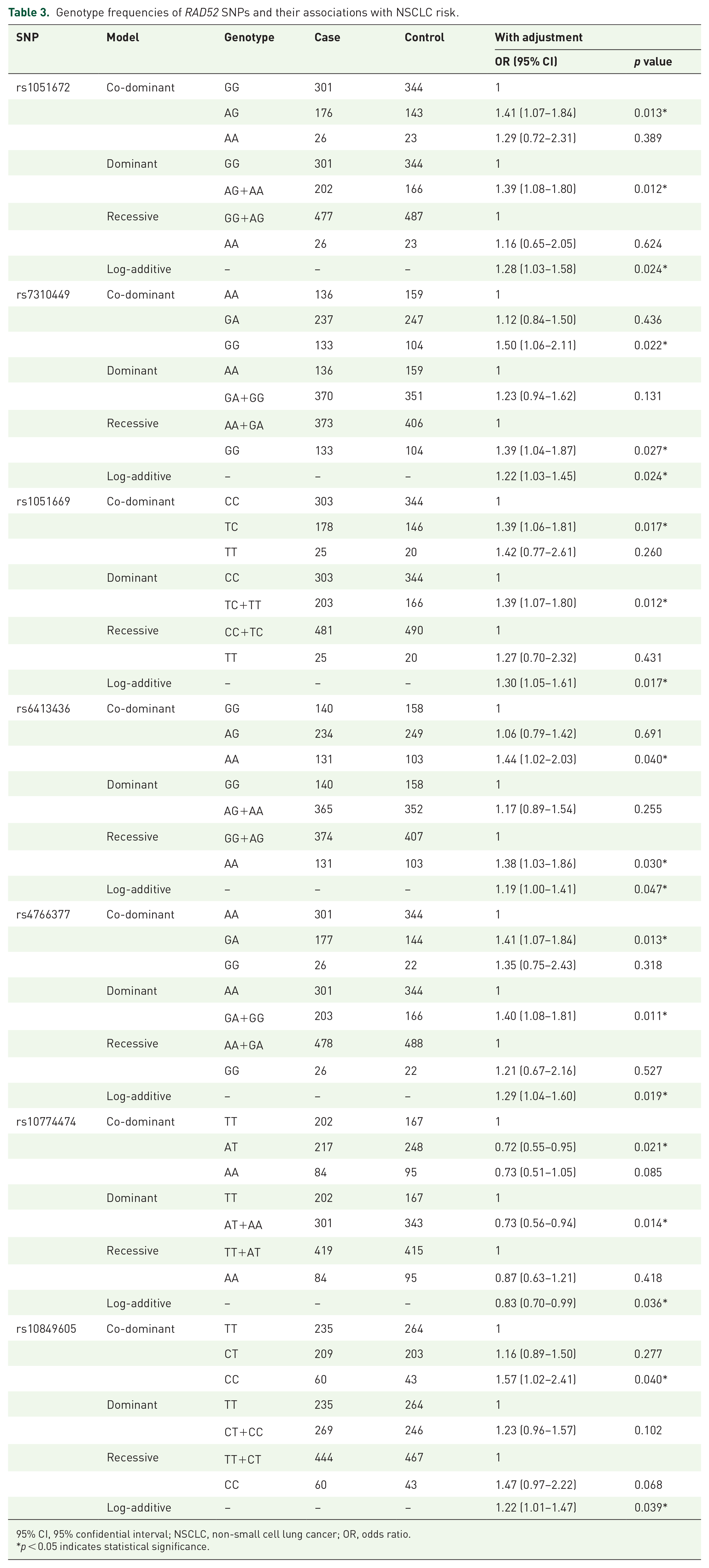
The genotype distribution of cases and controls with the NSCLC risk were compared under different models (Table 3). The frequencies of variant genotypes AT and AA were significantly higher compared with the rs10774474 TT genotype, and the TT genotype was related to a decreased risk of NSCLC under the co-dominant model (OR = 0.72, 95% CI = 0.55–0.95, p = 0.021), dominant model (OR = 0.73, 95% CI = 0.56–0.94, p = 0.014) and log-additive model (OR = 0.83, 95% CI = 0.70–0.99, p = 0.036). The variable genotypes of rs1051672, rs7310449, rs1051669, rs6413436, rs4766377 and rs10849605 all increased NSCLC risk under different genetic models. The rs1051672 AG genotype carriers had a 1.41-fold elevated risk of developing NSCLC when compared with GG genotype carriers under the co-dominant model (OR = 1.41, 95% CI = 1.07–1.84, p = 0.013). Rs1051672 was also associated with an increased NSCLC risk under dominant and log-additive models. Rs7310449 was associated with an increased risk of NSCLC under the co-dominant (OR = 1.50, 95% CI = 1.06–2.11, p = 0.022), recessive (OR = 1.39, 95% CI = 1.04–1.87, p = 0.027) and log-additive (OR = 1.22, 95% CI = 1.03–1.45, p = 0.024) models. Compared with rs1051669 CC genotype carriers, the TC genotype carriers had a 1.39-fold elevated risk of developing NSCLC under the co-dominant model (OR = 1.39, 95% CI = 1.06–1.81, p = 0.017), and rs1051669 was associated with an increased NSCLC risk under dominant and log-additive models. Rs6413436 was associated with an increased risk of NSCLC under multiple models (co-dominant: OR = 1.44, 95% CI = 1.02–2.03, p = 0.040; recessive: OR = 1.38, 95% CI = 1.03–1.86, p = 0.030; log-additive: OR = 1.19, 95% CI = 1.00–1.41, p = 0.047). Compared with rs4766377 AA genotype carriers, the carriers with the GA genotype had a 1.41-fold elevated NSCLC risk under the co-dominant model (OR = 1.41, 95% CI = 1.07–1.84, p = 0.013). Rs4766377 was associated with an increased NSCLC risk under dominant and log-additive models as well. Under the co-dominant model, the CC genotype of rs10849605 was associated with an increased risk of NSCLC (OR = 1.57, 95% CI = 1.02–2.41, p = 0.040), and rs10849605 was linked to an increased NSCLC risk under the log-additive model.
Genotype frequencies of RAD52 SNPs and their associations with NSCLC risk.
95% CI, 95% confidential interval; NSCLC, non-small cell lung cancer; OR, odds ratio.
p < 0.05 indicates statistical significance.
We performed stratification analysis to explore the relationships between RAD52 SNPs and NSCLC risk in the subgroup of age, gender, body mass index (BMI), drinking status, tumor type and lymph node metastasis (Table 4). Stratification analysis of age showed that rs1051672, rs1051669 and rs4766377 significantly increased NSCLC risk in individuals equal to or younger than 59 years whereas rs10774474 significantly decreased NSCLC risk. In addition, rs12822733 significantly increased NSCLC risk among individuals older than 59 years. Rs1051672, rs1051669, rs4766377 and rs10849605 were associated with an increased NSCLC risk among men. In women, rs7310449 and rs64131436 were associated with an increased NSCLC risk, and rs10774474 was associated with a decreased risk of NSCLC. Rs10774474 was correlated to a decreased NSCLC risk in the subgroup of BMI ⩽ 24. Rs1051672, rs1051669, rs4766377 and rs10849605 significantly increased NSCLC risk, while rs10774474 significantly decreased the NSCLC susceptibility in individuals with BMI > 24. In drinking status stratification analysis, rs1051672 and rs4766377 were associated with increased NSCLC risk in drinkers. When stratified by tumor histology type, rs1051672, rs1051669 and rs4766377 were associated with an increased squamous carcinoma risk, whereas rs12822733 and rs10774474 presented the associations with a decreased squamous carcinoma risk. Rs12822733 was related to an increased risk of adenocarcinoma, rs10774474 was associated with a decreased adenocarcinoma risk. In the lymph node metastasis stratification analysis, rs10774474 was associated with metastasis status.
The association between SNPs of RAD52 and demographic and clinical features of NSCLC.

OR and 95% CI of significant association is presented in bold.
95% CI, 95% confidential interval; BMI, body mass index; LN, lymph node; NSCLC, non-small cell lung cancer; OR, odds ratio.
In Table 5, we present the relationship between NSCLC clinical markers and RAD52 SNPs. We observed significant differences among rs12822733 genotypes in serum ferritin (SF; p = 0.020). The individuals carrying the rs12822733 GG genotype had the highest SF level, followed by GC genotype carriers, and CC genotype carriers had lowest expression. For tumor necrosis factor (TNF) expression analysis, the variations of rs1051672, rs1051669 and rs4766377 could significantly influence TNF expression, with the lowest expression quantity of the AA genotype, TT genotype and GG genotype, respectively. We also analyzed the association between the other six tumor associated markers with RAD52 SNPs, which included CEA, CA50, AFP, neuron-specific enolase (NSE), cytokeratin-19-fragment (CF211) and pro-gastrin-releasing peptide (ProGRP), there was no association between these indicators and RAD52 SNPs (Supplementary Table 2).
The association between SNPs of RAD52 and clinical index of NSCLC.

95% CI, 95% confidential interval; NSCLC, non-small cell lung cancer; SF, serum ferritin; TNF, tumor necrosis factor.
p < 0.05 indicates statistical significance.
Some patients were treated by chemotherapy based on cisplatin; we detected the association of RAD52 gene polymorphisms with chemotherapy effects and toxin side effects. There was no association between the eight SNPs and chemotherapy based on cisplatin; the results are shown in Supplementary Table 3.
The association between RAD52 haplotypes and NSCLC risk were analyzed. Figure 1 showed two linkage disequilibrium (LD) blocks in RAD52. Table 6 showed the association between different haplotypes and NSCLC risk. The haplotypes AGTA and GACG conducted by rs1051672, rs7310449, rs1051669 and rs6413436 significantly increased the NSCLC risk (OR = 1.29, 95% CI = 1.04–1.60, p = 0.021; OR = 1.21, 95% CI = 1.02–1.44, p = 0.027). The haplotypes GCTC and ACAT conducted by rs4766377, rs12822733, rs10774474 and rs10849605 were also associated with an increased risk of NSCLC (OR = 1.26, 95% CI = 1.02–1.57, p = 0.032; OR = 1.21, 95% CI = 1.02–1.44, p = 0.032).

D′ linkage map for the eight SNPs in RAD52.
RAD52 haplotype frequencies and the association with NSCLC risk.

95% CI, 95% confidential interval; NSCLC, non-small cell lung cancer; OR, odds ratio.
p < 0.05 indicates statistical significance.
Discussion
We conducted an association study in the RAD52 gene and NSCLC risk among the Chinese population living at a high altitude; rs10774474 was significantly associated with a decreased NSCLC risk, rs1051672, rs7310449, rs1051669, rs6413436, rs4766377 and rs10849605 significantly increased NSCLC risk. Four haplotype blocks were associated with an increased risk of NSCLC (Ars1051672Grs7310449Trs1051669Ars6413436, Grs1051672Ars7310449Crs1051669Grs6413436, Grs4766377Crs12822733Trs10774474Crs10849605, Ars4766377Crs12822733Ars10774474Trs10849605). The expression quantity of tumor-associated markers (SF and TNF) were significantly different in cases and controls. Our results suggest that RAD52 genetic polymorphisms might influence the NSCLC risk in a high altitude area of China.
The RAD52 gene plays a role in DNA strand exchange. 22 Previous studies reported that RAD52 variants were associated with a risk of glioma, 23 breast cancer 24 and colorectal cancer 25 in the Chinese Han population. They suggested that the effects of the RAD52 gene on multiple diseases may be related to DNA strand exchange. Song et al. found that RAD52 rs7963551 contributes to susceptibility to SCLC in the Chinese population. 17 In this study, we evaluated the association between eight SNPs and NSCLC susceptibility in Chinese from a high altitude area, and we found seven RAD52 polymorphisms had a significant association with NSCLC risk. Our finding enriched the association study between RAD52 and lung cancer.
In humans, RAD52 was involved in the HR pathway and plays a key role in regulating HR-related genomic instability. 26 NSCLC is particularly associated with smoking; the variation in RAD52 may potentially decrease the ability to repair carcinogen-induced damage and influences the risk of lung cancer. In addition, the depletion of RAD52 changed the cell cycle distribution by decreasing G0/G1 and increasing G2/M, the SNPs in RAD52 may influence RAD52 and then influence tumor cells division. It revealed the molecular mechanism of RAD52, which may be involved in NSCLC.
In the stratification analysis of tumor histology subtype, we found that rs12822733 had an association with decreased squamous carcinoma risk and increased adenocarcinoma risk, but not with NSCLC, so we speculate that it may be that tumor heterogeneity hampered the detection of the association signal when all lung cancers were analyzed.
A previous study found that RAD52 variants could predict platinum resistance and the prognosis of cervical cancer. 27 In this study, there was no significant association between the SNPs and chemotherapy based on cisplatin; it may be attributed to the different role of RAD52 variants to platinum resistance in different cancers.
Several limitations may exist in this study. First, selection bias is inevitable, because all individuals were recruited from the hospital, validation of our findings in a population-based prospective study is important. Second, the analysis of the BRCA2 status of these patients was limited. Finally, the relationships of RAD52 haplotypes with NSCLC risk in a Chinese high altitude area is still not enough to explain the molecular mechanism of RAD52 with the onset and development of NSCLC, further studies are needed to validate and expand our results.
Conclusion
In conclusion, we found that RAD52 polymorphisms were associated with the risk of NSCLC in the Chinese high altitude population. Future studies are mainly focused on these directions, one is to demonstrate the association between RAD52 and NSCLC risk in larger sample sizes and different populations, the other is to investigate the exact mechanisms of RAD52 influence on NSCLC risk.
Supplemental Material
Author_Response_1 – Supplemental material for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area
Supplemental material, Author_Response_1 for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area by Miao Li, Rong Chen, Baoyan Ji, Chunmei Fan, Guanying Wang, Chenli Yue and Guoquan Jin in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area
Supplemental material, Reviewer_1_v.1 for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area by Miao Li, Rong Chen, Baoyan Ji, Chunmei Fan, Guanying Wang, Chenli Yue and Guoquan Jin in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area
Supplemental material, Reviewer_2_v.1 for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area by Miao Li, Rong Chen, Baoyan Ji, Chunmei Fan, Guanying Wang, Chenli Yue and Guoquan Jin in Therapeutic Advances in Respiratory Disease
Supplemental Material
Supplementary_Tables – Supplemental material for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area
Supplemental material, Supplementary_Tables for RAD52 variants influence NSCLC risk in the Chinese population in a high altitude area by Miao Li, Rong Chen, Baoyan Ji, Chunmei Fan, Guanying Wang, Chenli Yue and Guoquan Jin in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors sincerely thank all participatants in this study.
Author contribution(s)
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflict of interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The informed consents were collected from all participants before this study. Our study was approved by the Ethical Committee of the Qinghai Province Cancer Hospital and conformed to the Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Qinghai science and technology department fund (2017-ZJ-707).
Supplementary material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.