
Abstract
Background:
An increasing number of patients require prolonged mechanical ventilation (PMV) to survive recovery from critical care. It should be emphasized that PMV is a neglected disease in chest medicine. We investigated 6 years of clinical outcomes and long-term survival rates of patients who required PMV.
Methods:
We analyzed retrospectively data from patients in respiratory care center (RCC) to investigate the main causes of respiratory failure leading patients to require PMV. We also studied the factors that influence the ventilator weaned rate, factors that influence the long-term ventilator dependence of patients who require PMV, as well as patients’ hospital mortality and long-term survival rates.
Results:
A total of 574 patients were admitted to RCC during the 6 years. Of these, 428 patients (74.6%) were older than 65 years. A total of 391 patients (68.1%) were successfully weaned from the ventilator while 83 patients (14.4%) were unsuccessfully weaned. A total of 95 patients (16.6%) died during RCC hospitalization. The most common cause of acute respiratory failure leading to patients requiring PMV was pneumonia. The factor that affected whether patients were successfully weaned from the ventilator was the cause of the respiratory failure that lead patients to require PMV. Our hospital mortality rate was 32.4%; the 1-year survival rate was 24.3%. There was a strong correlation between higher patient age and higher hospital mortality rate and poor 1-year survival rate. Patients with no comorbidity demonstrated good 1-year survival rates. Patients with four comorbidities and patients with end-stage renal disease requiring hemodialysis comorbidity showed poor 1-year survival rates.
Conclusions:
The factor that affected whether patients were successfully weaned from the ventilator was the cause of the respiratory failure that lead patients to require PMV. Older patients, patients with renal failure requiring hemodialysis, and those with numerous comorbidities demonstrated poor long-term survival.
The reviews of this paper are available via the supplemental material section.
Introduction
Following advancements in critical care technology the number of patients surviving the critical stage and requiring prolonged mechanical ventilation (PMV) increases. This medical phenomenon causes not only increased consumption of medical resources but also casts a long-lasting burden on patients’ families.
In 2004, National Association for Medical Direction of Respiratory Care (NAMDRC) held a conference associated with the care and management of patients requiring PMV. Patients on PMV are defined as those who use a mechanical ventilator for at least 6 h daily for at least 21 consecutive days. 1 In 2007, Mobaireek referred to non-cystic fibrosis bronchiectasis as an ‘orphan disease’. 2 Since then there have been annual international conferences on bronchiectasis and bronchiectasis guidelines to reference. However, no international conferences on PMV have been held by chest medicine experts since 2004. In this article, we emphasize how PMV is a neglected disease in chest medicine, and chest medicine experts must attach importance to patients requiring PMV and not let PMV become another orphan disease.
Patients requiring PMV have occupied beds in intensive care units (ICUs) in Taiwan before 2000; however, many patients cannot be admitted to the ICU because there are not enough available beds. They have to be transferred in a critical condition to another hospital. 3 In the USA, patients requiring PMV account for less than 10% of all patients requiring mechanical ventilation, but these patients occupy up to 40% of ICU bed days.4,5 In the UK, patients requiring PMV use 29.1% of all general ICU bed days and spend longer in hospital after discharge from the ICU than patients not requiring PMV. Establishing a weaning unit would potentially reduce acute ICU bed occupancy by 8–10% and could reduce overall treatment costs. 6 In 1999, a hospital in Taiwan set up a subacute ICU for patients requiring PMV. These patients would not therefore occupy an ICU bed, meaning more critical patients could be admitted to the ICU. 7 The ‘Trial Plan for National Public Health Insurance Ventilator Dependent Patients Comprehensive Care System’ has been promoted in Taiwan since July 2000. There are four phases, i.e. ICU, respiratory care center (RCC), respiratory care ward (RCW), and home care, for patients requiring PMV care. RCC is a subacute stage for patients receiving ventilator support for more than 21 days. 8 Patients requiring PMV is well documented in the literature,9–24 however, there are no detailed reports on the clinical picture, outcomes, and long-term survival of these patients.
What are the main causes of respiratory failure leading patients to PMV? What factors affect ventilator weaning? What factors cause long-term ventilator dependence? What factors cause patients who required PMV to die? What is the long-term survival of patients who required PMV? In this article, we report a comprehensive clinical experience of patients who required PMV and attempt to answer the above questions.
Methods
We retrospectively studied the medical records of 574 patients who were admitted to the RCC from January 2012 to December 2017. Patients were eligible for RCC admission if they met the Taiwan national health insurance requirements: (a) hemodynamic stability; (b) no vasoactive drug infusion needed; (c) stable oxygen condition (O2 saturation ⩾ 90% or PaO2 ⩾ 60 mmH) with the requirement fraction of inspired oxygen less than 40% and positive end-expiratory pressure less than10 cm H2O; (d) no critical acute hepatic or renal failure; (e) no massive upper gastrointestinal bleeding; (f) no requirement for surgical intervention within the ensuing 2 weeks or no large open surgical wound; (g) no uncontrolled severe infectious diseases; (h) no life-threatening arrhythmia. The collected data included age, gender, comorbidities, causes of respiratory failure, RCC discharge status, the outcome of weaned patients, hospital mortality, and long-term survival.
Ethics approval and consent to participate
The study was not a prospective clinical trial and was a retrospective medical records data collection and analysis. The possibility and severity of injury or discomfort were no higher than in daily life, routine physical examination, or psychological testing. The legal biological database cannot identify a specific individual. It cannot identify a particular individual’s data, files, documents, information, or samples for research. The study was the lowest risk, and the possible risk to the research subject did not exceed the nonparticipating researchers, and exemption from prior consent did not affect the rights of the researcher. Research risk did not exceed minimal risk. Exempt informed consent did not affect the subject rights and wellbeing. Research could not be performed without exempting informed consent. The project was approved by the Buddhist Dalin Tzu Chi general hospital research ethics committee (Approved IRB No.: B10802009).
Definition of outcomes
Discharge of RCC patients included patients who were successfully weaned from ventilators and those unsuccessfully weaned. Patients successfully weaned were defined as patients independent of the ventilator for 5 consecutive days and nights. Patients unsuccessfully weaned included those who died in the RCC, hospice patients in the RCC, and those who were ventilator dependent. The ventilator-dependent patients were transferred to the respiratory care ward for long-term ventilator support. RCC mortality rate was defined as the number of patients who died in the RCC divided by the total number of patients admitted to the RCC. Ward mortality rate was defined as the number of successfully weaned patients who died in the hospital before discharge divided by the total number of successfully weaned patients. Hospital mortality rate was defined as the number of mortality patients (including RCC mortality patients, ward mortality patients, and hospice patients, not including ventilator-dependent patients in the respiratory care ward) divided by the total number of patients admitted to the RCC.
Comorbidities
The numbers of comorbidities were assessed. These included: cardiovascular disease (such as essential hypertension, decompensated heart failure, coronary atherosclerotic disease, acute myocardial infarction), chronic lung disease (such as chronic obstructive pulmonary disease [COPD], asthma, bronchiectasis, interstitial lung disease), chronic kidney disease (not requiring dialysis), end-stage renal disease (requiring dialysis before admission), neurologic disease (such as old stroke, dementia, Parkinsonism), chronic liver disease (such as chronic hepatitis, liver cirrhosis), metabolic disease (such as diabetes mellitus, other endocrine disorders requiring treatment), malignant diseases, and miscellaneous diseases.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation or median (range), whereas categorical variables were expressed as frequencies and percentage. Furthermore, differences in baseline characteristics, causes of respiratory failure, or comorbidities were evaluated using the Student’s t test for continuous variables, and Pearson chi-square tests for categorical variables. Univariate analysis was used to analyze the association of each variable with successful weaning, RCC mortality, ward mortality, and 1-year survival rate. Multivariate stepwise logistic regression models were used to assess factors associated with both successful weaning and 1-year survival in all patients. Different age patients groups related to patients’ outcomes were analyzed by linear-by-linear association. All statistical analyses were conducted using the statistical package SPSS for Windows (Version 17.0), and a p value < 0.05 was considered to show statistical significance.
Results
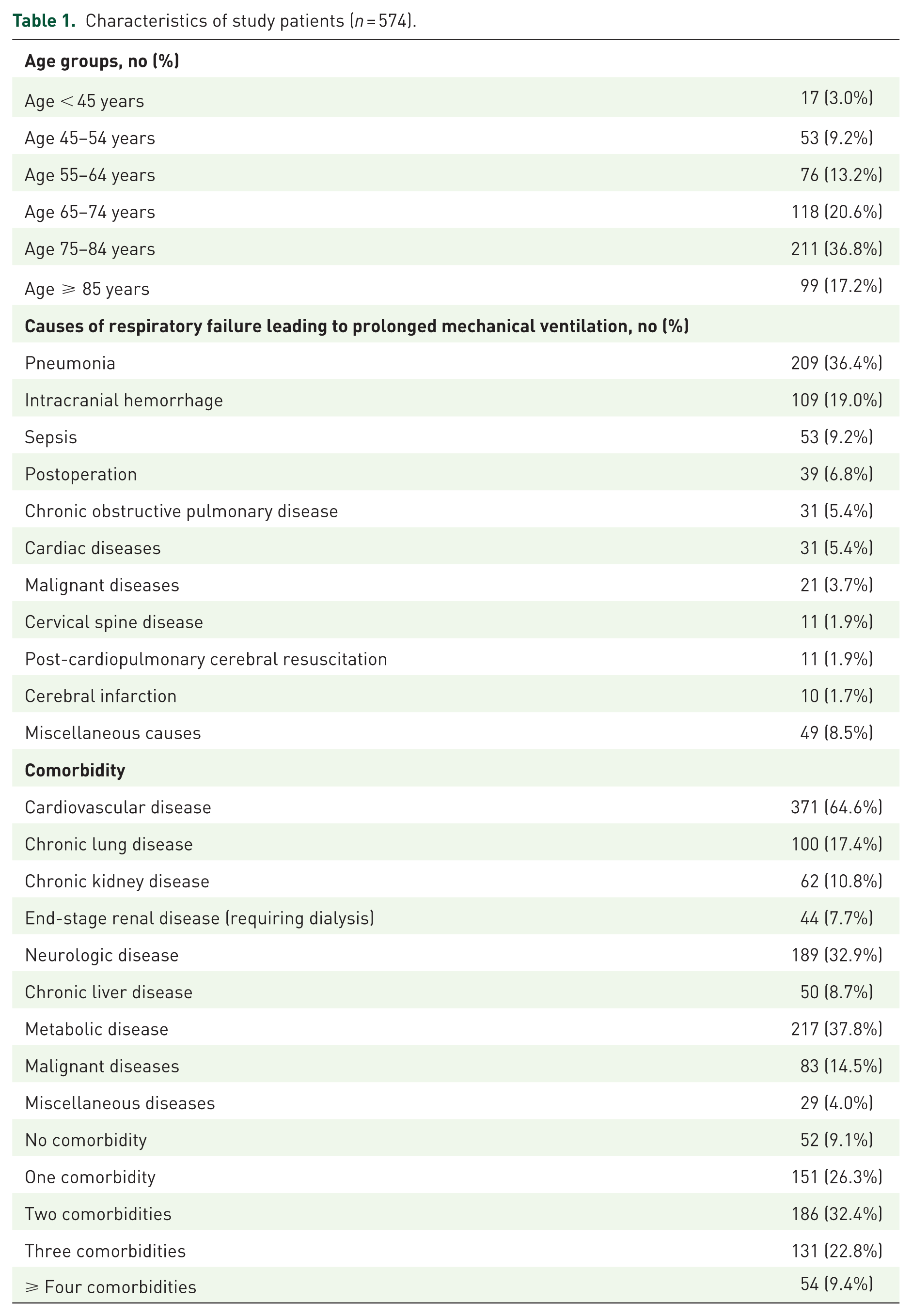
A total of 574 patients were admitted to RCC during the 6 years. Of these, 357 patients (62.2%) were men, and 217 (37.8%) were women. The mean age was 72.4 years. A total of 428 patients (74.6%) were older than 65 years. We classified the 574 patients who required PMV into 11 categories according to the cause of the acute respiratory failure that lead patients to require PMV. The categories were: (a) pneumonia in 209 patients (including patients with chronic lung disease complicated with pneumonia) (36.4%); (b) intracranial hemorrhage (ICH) in 109 patients (19.0%); (c) sepsis (not due to pneumonia) in 53 patients (9.2%); (d) postoperative condition in 39 patients; (e) COPD in 31 patients; (f) cardiac disease (including decompensated heart failure, coronary atherosclerotic disease, acute myocardial infarction, etc.) in 31 patients; (g) underlying malignancies in 21 patients; (h) cervical spine diseases in 11 patients; (i) post Cardio-Pulmonary-Cerebral-Resuscitation (CPCR) hypoxic encephalopathy in 11 patients; (j) cerebral infarction in 10 patients; (k) miscellaneous causes in 49 patients. A total of 151 patients had one comorbidity (26.3%); 186 patients had two comorbidities (32.4%); 131 patients had three comorbidities (22.8%); 54 patients had more than four comorbidities (9.4%). The top three comorbidities were cardiovascular diseases (371 patients, 64.6%), metabolic diseases (217 patients, 37.8%), and neurologic diseases (189 patients, 32.9%) (Table 1). A total of 391 patients (68.1%) were successfully weaned from the ventilator, while 83 patients (14.4%) were unsuccessfully weaned and needed long-term ventilator dependence. A total of 95 patients (16.6%) died during RCC hospitalization. Five patients received hospice therapy.
Characteristics of study patients (n = 574).
Looking at the causes of acute respiratory failure that lead patients to require PMV, the two causes with the most successfully weaned patient groups were cerebral infarction (90%) and intracranial hemorrhage (83.5%). The two causes with the worst RCC mortality were patients with malignant disease (28.6%) and sepsis (26.4%). There were more patients with COPD and cervical spine disease who were ventilator dependent (Table 2).
The causes of respiratory failure related to RCC discharge outcomes.

There were 186 hospital mortality patients, including 95 RCC mortality patients, 5 hospice patients, and 86 ward mortality patients. The hospital mortality rate was 32.4%. The two causes with the highest mortality of RCC mortality patients were pneumonia and sepsis. The two causes with the highest mortality of ward mortality patients were pneumonia and repeated respiratory failure in the ward (Table 3). The 1-year survival rate was 24.3%. We will be able to gather further long-term follow-up data on 403 patients (70.2%) up to 30 October 2018.
The causes of death in hospital mortality.

The factors associated with successfully weaned patients are shown in Table 4. Age groups were not related to successful or unsuccessful weaning in our series. There were good successfully weaned outcomes in patients with ICH. There were poor successfully weaned outcomes in patients with sepsis, COPD, and underlying malignant disease.
Factors associated with successfully weaned patients.

COPD, chronic obstructive pulmonary disease; ICH, intracranial hemorrhage; PMV, prolonged mechanical ventilation.
A comparison of RCC patients with different causes of acute respiratory failure leading to PMV in RCC mortality and ward mortality are shown in Table 5. We found higher mortality outcomes in ward mortality patients than RCC mortality patients. Patients with ICH showed poor ward mortality compared with RCC mortality.
RCC patients with different causes of respiratory failure according to RCC mortality and ward mortality.

Factors associated with the 1-year survival rate in patients who required PMV are shown in Table 6. Our series showed a good 1-year survival rate for patients with no comorbidity. Patients older than 75 years, patients with a comorbidity of end-stage renal disease (ESRD), and patients with more than four comorbidities displayed a poor 1-year survival rate (Table 6).
Factors associated with 1-year survival in patients who required PMV.
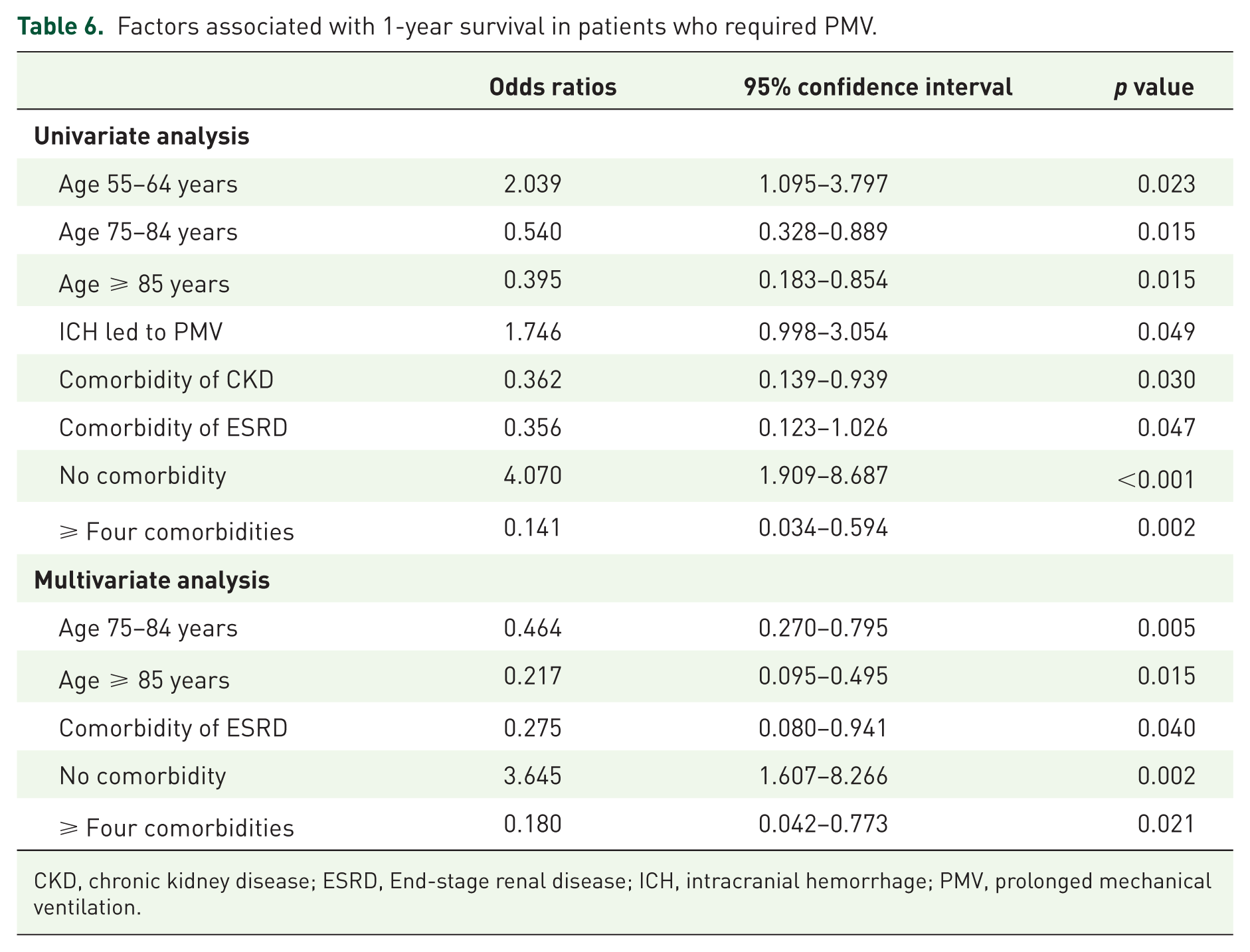
CKD, chronic kidney disease; ESRD, End-stage renal disease; ICH, intracranial hemorrhage; PMV, prolonged mechanical ventilation.
We analyzed different age groups in relation to patient outcomes. There was no relation between increasing patient age and successfully weaned rate, long-term ventilator dependence, and RCC mortality. There was a relationship between increasing patient age and high hospital mortality and poor 1-year survival rate (Table 7).
RCC patients of different age groups related to patients’ outcomes analyzed by linear-by-linear association.

Discussion
The previous study by Lin and colleagues from the Taiwan national health insurance research database had a total of 50,481 RCC patients, 60% men and 40% women, with an average age of 72 years. 20 Another study by Lai and colleagues was based on Taiwan medical center data from 1820 RCC patients, 59.2% men and 40.8% women, with an average age of 69.8 years. 24 Our data were similar to these two Taiwanese reports. In the US reports, the average age of RCC patients was 55.0–71.8 years, which was about 10 years younger than that in the studies from Taiwan. As for gender distribution, men accounted for 50–59%, and women accounted for 41–50%. The percentage of US female patients was slightly higher than in the studies from Taiwan.13–16 The UK published a study of 349 patients who required PMV, 57.6% men and 42.4% women, with an average age of 59.6 years. 6
What are the main causes of respiratory failure leading patients to require PMV?
Although there are many papers on PMV, few articles explore the main causes of respiratory failure leading the patient to require PMV. In our patient population, the top three underlying causes of acute respiratory failure leading patients to require PMV were pneumonia, ICH, and sepsis. In the paper by Lai and colleagues their patient population showed the top underlying causes as pneumonia, neuromuscular disease, and decompensated congestive heart failure. 24 Data from the Taiwan national health insurance research database revealed that the top five causes were acute respiratory failure, pneumonia, ICH, sepsis, and COPD. 21 Scheinhorn and colleagues displayed the top causes as pneumonia, COPD, coronary artery bypass graft, and decompensation congestive heart failure. 14 Lone and Walsh reported that the top three causes in order were pneumonia, sepsis, and trauma. 6 Gathering data from all the literature finds that medical diseases such as pneumonia, COPD, sepsis, and decompensation congestive heart failure, are the most common causes of respiratory failure leading patients to require PMV. Moreover, pneumonia is the most common cause of respiratory failure that leads patients to require PMV. In our group, ICH was the second leading cause of PMV because there were many patients with ICH who transferred to our hospital for an operation.
What factors affect ventilator successfully weaned rates?
Our successfully weaned rate was 68.1%. A study carried out by Lin and colleagues in a medical center in Taiwan had a successfully weaned rate of 52.2%. 23 In another of Taiwan’s reports the RCC patients’ successfully weaned rate was 48.2%. 20 Damuth and colleagues reported a systematic review and meta-analysis which showed that the all acute care hospitals successfully weaned rate was 48.8%. The successfully weaned rate was 58.6% in all weaned units in acute-care hospitals. In all post-acute hospitals the successfully weaned rate was 52.9%. 25 Our RCC was similar to weaned units in acute-care hospitals, and our weaned rate was better than reports in the literature. We displayed a better successfully weaned rate because 19% of patients who required PMV had ICH in our series. Frengley and colleagues showed that the successfully weaned rate decreased with age. 17 Lin and colleagues reported that the failed weaned rate showed no difference based on the patient’s age. 20 Our data revealed that age does not affect the success or failure of weaning from the ventilator. The critical factors that affect ventilator weaned rates are the causes of the respiratory failure that lead patients to require PMV. Patients with ICH had an excellent successfully weaned rate. Patients with sepsis, COPD, and underlying malignant disease had a worse successfully weaned rate.
What factors cause patients to be long-term ventilator dependent?
In our group, 16.6% of patients were ventilator dependent. The two Taiwan reports showed rates of 15.45% and 20.3% for patients needing long-term ventilator dependence, respectively.18,23 Unroe and colleagues reported that 17.4% of their patients were long-term ventilator dependent. 15 Pilcher and colleagues showed that 35% of patients were long-term ventilator dependent, 12 and Scheinhorn and colleagues showed that 20.9% of patients were long-term ventilator dependent. 13 We were the only study to analyze further the subgroups of our patients. Our series showed that patients with ICH needed less long-term ventilator support (odds ratio [OR] = 0.345, p = 0.011), and patients with COPD (OR = 2.817, p = 0.007) and cervical spine disease (OR = 3.380, p = 0.043) needed more long-term ventilator support.
What factors cause patients who required PMV to die?
Our RCC mortality was 16.6%. Two of the Taiwan reports showed RCC mortality as 22.98% and 24%, respectively.18,23 Three reports from the Western world showed RCC mortality as 27%, 25%, and 26.7%, respectively.12,14,15 Our RCC mortality was better than the literature reports, which was due to our high successfully weaned rate. Many patients who required PMV were successfully liberated from the ventilator in the RCC and then transferred to the ward. However, some patients expired in the hospital before being discharged. To our knowledge, no literature discussed the scope of ward mortality in patients who required PMV. We found higher ward mortality than RCC mortality in our series. Patients with ICH showed poor ward mortality compared with RCC mortality. We think three factors lead to the high ward mortality in our successfully weaned patients. First, some patients were successfully weaned in RCC, but the patients’ general health condition and consciousness were worse than before, especially patients with ICH. Patients’ families refused to let patients receive endotracheal tube intubation if the patients again suffered respiratory failure. Patients’ families wanted the patients to receive noninvasive therapy. Second, there was no electrocardiography (ECG) monitor available for ward patients, and we could not monitor patients’ vital signs and oxygen saturation closely. Third, the nurse-to-patient ratio was 3:10 in our RCC and 1:8 in the ward. The patient’s family is more responsible for the patient’s care in the ward. Therefore, more complications, such as food choking, pressure sore occurrence, sputum impaction, etc., occur in the ward than in the RCC.
Damuth and colleagues reported that all hospitals overall hospital mortality was 29.1%. 25 The factors associated with hospital mortality were not discussed. Pilcher and colleagues showed 27% hospital mortality, which increased with age. 12 Lai and colleagues reported that their series of hospital mortality was 17.6% and patients over 80 years old; those requiring hemodialysis had a higher risk of death. 24 There was a relationship between increasing patients’ age and higher hospital mortality in our series. However, our hospital mortality (32.4%) was worse than in the literature reports, and we inferred this high hospital mortality resulted in our high ward mortality.
What is the long-term survival of patients requiring PMV?
Damuth and colleagues reported that in all weaned units in acute-care hospitals the 1-year survival rate was 45.2%. In all post-acute hospitals the 1-year survival rate was 32.1%. 25 The literature showed that among international patients requiring PMV long-term survival is better than in the USA. The national health insurance research database of Taiwan had a 1-year survival rate of 31.9%. 22 Unroe and colleagues and Scheinhorn and colleagues had 1-year survival rates of 56% and 40%, respectively.14,15 Several reports mentioned that the older age of patients requiring PMV was significantly associated with poor survival.14,15,21,26 Frengley and colleagues mentioned that age was not the dominant factor in predicting outcomes. 17 It was also never doubted that patients’ comorbidities were an influencing factor. Based on previous studies, patients with a malignant neoplasm or renal failure requiring hemodialysis had a significant association with poor survival.21,22,26 In addition, patients with numerous comorbidities who required PMV demonstrated poor long-term survival.14,15
Our patients’ group presented an abysmal 1-year survival rate (24.3%). Our series demonstrated that patients with ESRD had a poor 1-year survival rate, which is the same as in the literature. There was a relationship between increasing patients’ age and a poor 1-year survival rate in our RCC patients. Our series showed patients with no comorbidity had excellent 1-year survival rates; on the contrary, patients with more than four comorbidities had a poor 1-year survival rate.
Limitations of our study
Our study was a report of clinical data from patients who required PMV. We did not collect patient’s laboratory data, respiratory parameters, APACHE II score, Glasgow Coma Scale (GCS), etc. This implies that our study could not offer laboratory examinations, respiratory parameters, APACHE II score, and GCS, which are often related to a patient’s outcome and long-term survival rate. Several reports described lower BUN, lower APACHE II score, and higher serum albumin; a higher GCS score was associated with successful weaning. Lower serum albumin, higher APACHE II score, and thrombocytopenia were associated with poor long-term survival rates.23,24,27–29 Dettmer and colleagues’ systematic review showed that vasopressor use and thrombocytopenia were associated with higher mortality. 30 All of these studies were scattered retrospective single-unit studies. Although we made some conclusions about the clinical outcomes and long-term survival rate among patients who required PMV, these results were only concluded from our retrospective single-unit investigations. There is no doubt that further prospective studies on PMV are urgently needed. We expect international chest medicine experts to carry out more clinical prospective studies for patients requiring PMV and provide these patients with better medical care.
Conclusion
The most common causes of respiratory failure leading patients to PMV was pneumonia. The factor that affected whether patients were successfully weaned from the ventilator was the cause of the respiratory failure that lead patients to require PMV. More patients with COPD and cervical spine disease need long-term ventilator dependence. Patient age was not a significant factor for the successfully weaned rate, long-term ventilator dependence, and RCC mortality. Patients with renal failure requiring hemodialysis and numerous comorbidities demonstrated poor 1-year survival. Older age patients have a worse long-term prognosis such as hospital mortality and 1-year survival rate.
Supplemental Material
Author_response_to_reviewer_comments – Supplemental material for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan
Supplemental material, Author_response_to_reviewer_comments for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan by Chienhsiu Huang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan
Supplemental material, Reviewer_1_v.1 for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan by Chienhsiu Huang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.2 – Supplemental material for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan
Supplemental material, Reviewer_1_v.2 for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan by Chienhsiu Huang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan
Supplemental material, Reviewer_2_v.1 for How prolonged mechanical ventilation is a neglected disease in chest medicine: a study of prolonged mechanical ventilation based on 6 years of experience in Taiwan by Chienhsiu Huang in Therapeutic Advances in Respiratory Disease
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author declares no conflict of interest in preparing this article.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.