
Abstract
Background:
Patients diagnosed with chronic obstructive pulmonary disease (COPD) in China are commonly prescribed ipratropium plus theophylline (I+T) therapy. Studies have shown that an inhaled corticosteroid (ICS)/long-acting β2-agonist (LABA) combination is also efficacious in reducing symptoms and exacerbations. This study evaluated the efficacy and tolerability of adding budesonide/formoterol (BUD/FORM) to I+T in Chinese patients with severe COPD.
Methods:
A randomized, parallel-group, open-label, multicenter phase IV study (Clinical Trials.gov identifier: NCT01415518) was conducted in China. Patients received either BUD/FORM (160/4.5 µg; two inhalations twice daily [bid] via Turbuhaler®) + I (20 µg per inhalation, two inhalations four times daily) + T (100 mg bid) or I+T alone for 12 weeks. The primary efficacy variable was change from baseline in predose forced expiratory volume in 1 s (FEV1).
Results:
A total of 584 patients were randomized equally between treatment groups. At the end of the study, the BUD/FORM plus I+T group displayed significant improvements in predose FEV1 versus the I+T group (between-group difference 6.9%; 95% confidence interval [CI]: 4.3, 9.6; p < 0.0001). Forced vital capacity, inspiratory capacity, peak expiratory flow and health-related quality of life (HRQoL) scores were significantly improved (all p < 0.0001) and exacerbation frequency was reduced (43.5% reduction; rate ratio 0.565, 95% CI 0.325, 0.981; p = 0.0425) with BUD/FORM plus I+T versus I+T alone.
Conclusion:
Patients with severe COPD in China treated with BUD/FORM plus I+T showed significant improvements in lung function and HRQoL and a reduction in exacerbations compared with I+T alone. Both treatments were well tolerated and no safety concerns were noted.
The reviews of this paper are available via the supplemental material section.
Introduction
Chronic obstructive pulmonary disease (COPD) is a global health concern and has been predicted to become one of the top three leading causes of death worldwide by 2030.1,2 In China, COPD affects 13.7% of individuals aged >40 years and was responsible for 1.6% of hospitalizations in 2015. The prevalence of COPD in China increased by 67.1% between 2004 and 2015, and current estimates suggest that nearly 100 million people in China have COPD. 3
A common treatment for COPD in China is the dual combination of ipratropium [a short-acting muscarinic antagonist (SAMA)] and theophylline (a methylxanthine), primarily because these agents have reported clinical efficacy in COPD patients,4–7 are affordable (particularly in rural areas), and are readily available. In contrast to common practice in China, however, current COPD treatment recommendations suggest using a long-acting bronchodilator for the management of most patients with stable COPD; patients with persistent exacerbations (more severe disease) may benefit from the addition of a second long-acting bronchodilator or the use of a combination of inhaled corticosteroid (ICS) and long-acting β2-agonist (LABA). 8 Indeed, the ICS/LABA combination of budesonide/formoterol (BUD/FORM) is frequently used as an effective maintenance therapy for patients with moderate to very-severe COPD, especially for those who have a history of COPD exacerbations.9–14
To date, little is known regarding the effects of adding ICS/LABA to maintenance therapy regimens other than long-acting bronchodilators. Since ipratropium plus theophylline (I + T) is a common maintenance regimen for COPD in China, this study was performed to evaluate the efficacy and tolerability of adding BUD/FORM to such therapy compared with the combination of I + T alone in Chinese patients with severe COPD.
Methods
Study design
This 12-week, randomized, parallel-group, open-label, phase IV study (ClinicalTrials.gov identifier: NCT01415518) was conducted in 25 centers (Tier II/III hospitals) in China between August 31, 2011 and December 7, 2012.
Inclusion criteria
Eligible patients were those aged ⩾40 years, with a clinical diagnosis of COPD with symptoms for >2 years, prebronchodilator forced expiratory volume in 1 s (FEV1) ⩽50% of predicted normal, a prebronchodilator FEV1/forced vital capacity (FVC) ratio <0.70, a current/prior smoking history of ⩾10 pack-years, and history of ⩾1 severe COPD exacerbation (i.e., requiring treatment with oral corticosteroids and/or antibiotics) in the 12-month period before randomization.
Patients were excluded from this trial if they had a history of asthma/allergic rhinitis, had experienced a COPD exacerbation mandating hospitalization, or had emergency room treatment, or required treatment with ICS, oral steroids, intravenous corticosteroids or antibiotics within the 4-week period prior to visit two or during the run-in period. Patients with any significant/unstable cardiovascular disorder were excluded, as were patients with clinically significant narrow-angle glaucoma, prostatic hyperplasia, or bladder-neck obstruction.
The trial was performed in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All patients provided written informed consent. The study protocol was approved by the Independent Ethics Committee at the leading site (Beijing Hospital, Ministry of Health), following approval by ethics committees at all other sites.
Study design and treatments
The study design and treatments are described in Figure 1.
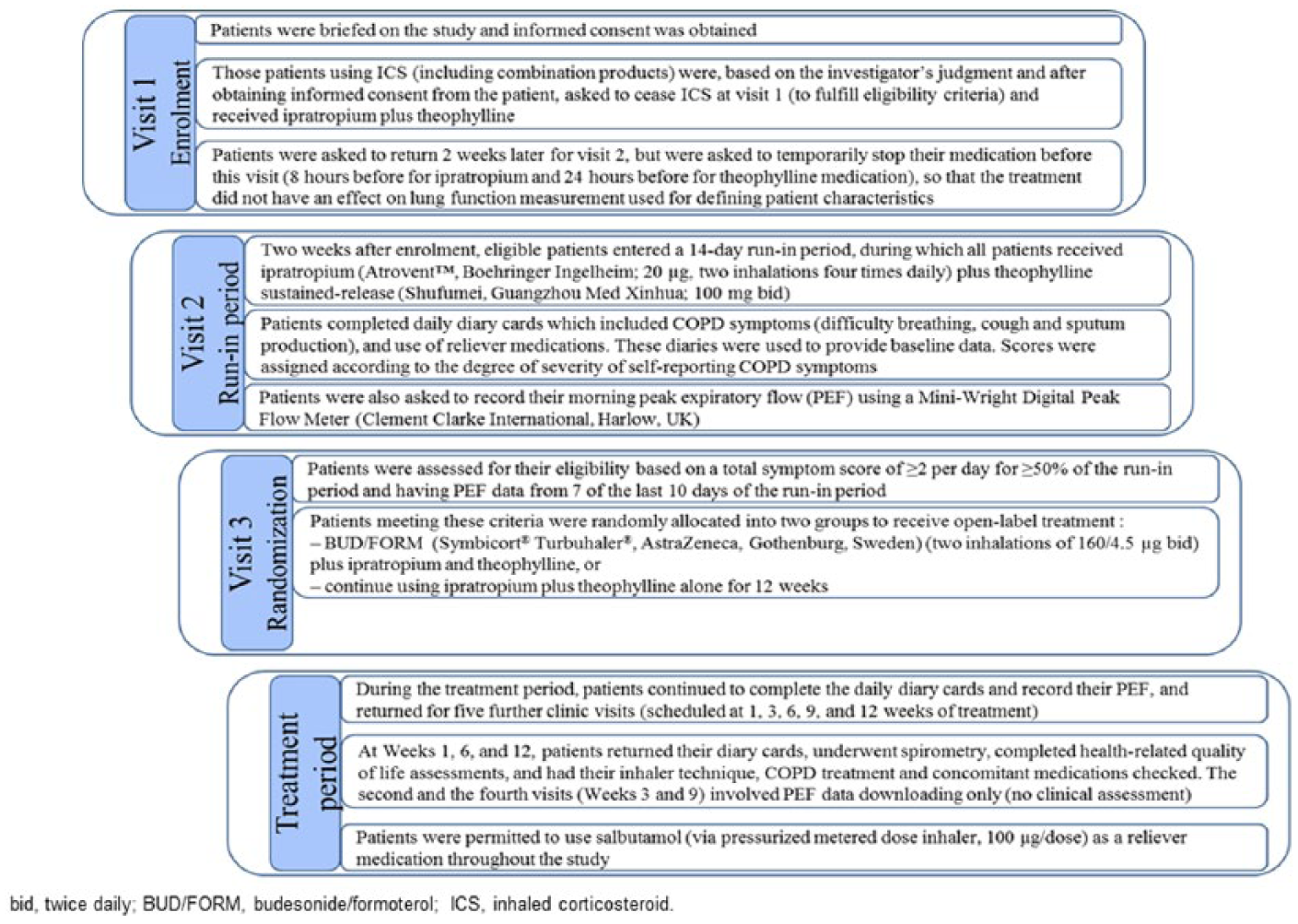
Study design and treatments.
Patients were instructed by study personnel on inhaler technique/how to take medication at the time they were given study medication. Patients were required to practice inhalation technique as many times as necessary until they could demonstrate proper inhaler technique to the supervising Investigator/study nurse. In addition, patients received written information (in local language) on how to correctly use the inhalers, as well as the importance of complying with the study regimen.
Assessments
The primary efficacy variable was the mean change in predose FEV1 from baseline to the treatment period visits (weeks 1, 6, and 12). Secondary efficacy variables included changes in lung function [5- and 60-min postdose FEV1, predose and 5- and 60-min postdose FVC, predose and 60-min postdose inspiratory capacity (IC)], predose and 5-min postdose PEF (measured in the morning only), changes in use of day- and night-time reliever medications, changes in COPD symptoms using the Breathlessness, Cough and Sputum Scale (BCSS), 15 the development of severe COPD exacerbations [requiring systemic steroids (oral ⩾3 days or parenteral) or hospitalization or emergency room treatment due to the deterioration of COPD], the time to first COPD exacerbation, and changes in health-related quality of life [HRQoL; assessed with the St George’s Respiratory Questionnaire for COPD patients (SGRQ-C) total score, where higher scores indicate worse health status]. The Mandarin Chinese version has been validated in a Chinese COPD population. 16 Safety was evaluated by monitoring of adverse events (AEs) and serious AEs (SAEs), and investigators assessed whether AEs were linked to study treatment.
Statistical analyses
All patients who provided postrandomization efficacy data were included in the full analysis set (FAS), which was used for all efficacy analyses. The safety analysis set included all patients who provided postrandomization data and took at least one dose of study medication.
An ANCOVA multiplicative model based on log-transformed response data was used to analyze FEV1, FVC, and IC. The ratios to baseline values and geometric means with their ratios were used for evaluating treatment effects and their differences. An ANCOVA additive model was used to analyze PEF, using day- and night-time reliever medications, SGRQ-C scores, and BSCC scores as changes from baseline values. Poisson regression was adopted to analyze the COPD exacerbation rates, and a Cox proportional hazards model was used to analyze the time to first COPD exacerbation.
Based on previous clinical trials,11,12,17 the standard deviation (SD) of the predose FEV1 was assumed to be 0.175 l on the natural logarithmic scale. A sample size of 259 patients per treatment group would have 90% power to detect a true mean between-group difference of 0.05 on the natural logarithm scale at a two-sided significance level of 0.05. Assuming a potential drop-out rate of 10%, 285 patients per treatment group were planned to be randomized in the study.
Results
Patients
Overall, 774 patients were screened and 584 were randomized to treatment (n = 292 for both BUD/FORM plus I + T, and I + T groups; Figure 2). Both the FAS and safety populations comprised 582 patients.

CONSORT diagram showing patient flow through the study (including reasons for withdrawal).
The demographic and baseline clinical characteristics of the patients were comparable between the two groups (Table 1). A small number of patients (n = 28) were described as having moderate COPD according to the criteria described in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines of 2010, 18 the prevailing version at the time of the study (Table 1).
Patient demographics and baseline characteristics (FAS population) a .

BUD/FORM: budesonide/formoterol; CV: coefficient of variation; FAS: full analysis set; I+T: ipratropium + theophylline; SD: standard deviation.
Two patients were excluded from the BUD/FORM plus I+T group because no efficacy data were recorded after randomization.
Of those patients randomized, 276 patients (94.5%) in the BUD/FORM plus ipratropium and theophylline group and 261 patients (89.4%) in the I + T group completed the study. Patients in the latter group displayed a higher discontinuation rate compared with the BUD/FORM plus ipratropium and theophylline group (10.6% versus 5.5%) and a significantly shorter time to discontinuation (p = 0.015).
Lung function parameters
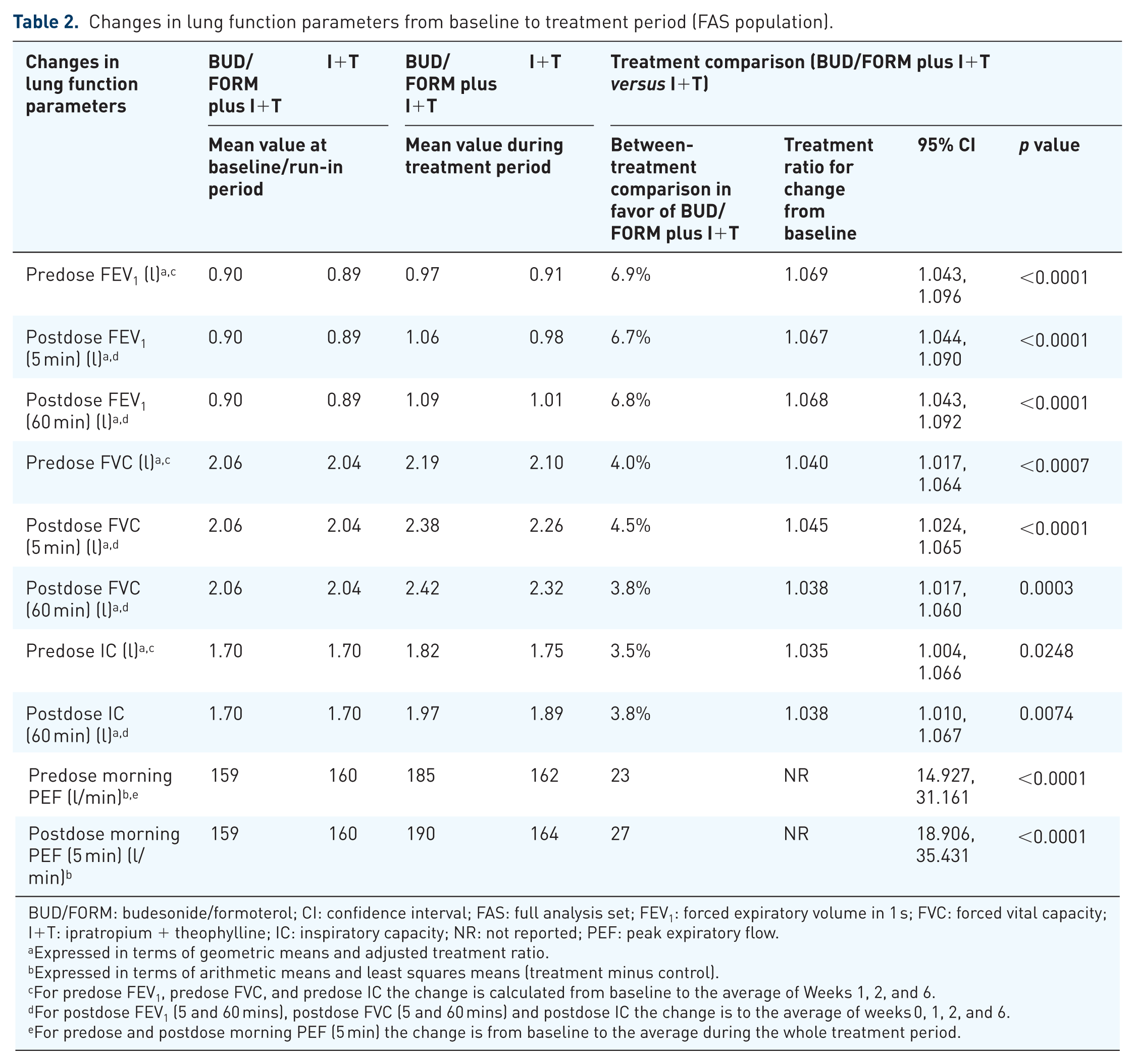
The mean change in predose FEV1 from baseline to the treatment period visits (weeks 1, 6, and 12) was greater in the BUD/FORM plus I + T group than the I + T group (Figure 3). By the end of the study, the mean predose FEV1 increased from baseline by 7.9% in the BUD/FORM plus I + T group compared with 0.9% in the I + T group. The adjusted ratio for between-treatment comparison was 1.069 (95% confidence interval [CI]: 1.043, 1.096; p < 0.0001), corresponding to a 6.9% difference between the groups (Table 2).

Change in absolute predose FEV1 from baseline to mean of treatment period.
Changes in lung function parameters from baseline to treatment period (FAS population).
BUD/FORM: budesonide/formoterol; CI: confidence interval; FAS: full analysis set; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; I+T: ipratropium + theophylline; IC: inspiratory capacity; NR: not reported; PEF: peak expiratory flow.
Expressed in terms of geometric means and adjusted treatment ratio.
Expressed in terms of arithmetic means and least squares means (treatment minus control).
For predose FEV1, predose FVC, and predose IC the change is calculated from baseline to the average of Weeks 1, 2, and 6.
For postdose FEV1 (5 and 60 mins), postdose FVC (5 and 60 mins) and postdose IC the change is to the average of weeks 0, 1, 2, and 6.
For predose and postdose morning PEF (5 min) the change is from baseline to the average during the whole treatment period.
The BUD/FORM plus I + T group demonstrated greater improvements in all secondary efficacy variables related to lung function (postdose FEV1, FVC, IC, and PEF) compared with the I + T group (Table 2). At 5 min postdose, the FEV1 was 6.7% greater (95% CI: 4.4, 9.0; p < 0.0001) in the BUD/FORM plus I + T group than in the I + T group; at 60 min postdose it was 6.8% greater (95% CI: 4.3, 9.2; p < 0.0001). Similar significant between-treatment differences were observed for the changes in FVC, PEF, and IC.
Exacerbations
Exacerbation rates were 43.5% lower in the BUD/FORM plus I + T group (rate 0.069 per patient per 12 weeks; 95% CI: 0.044, 0.106) than the I + T group (rate 0.121 per patient per 12 weeks; 95% CI: 0.087, 0.170), corresponding to a rate ratio of 0.565 (95% CI: 0.325, 0.981; p = 0.0425). The hazard ratio of time to the first COPD exacerbation in each patient (excluding multiple events) for BUD/FORM plus I + T versus I + T was 0.604 (95% CI: 0.339, 1.078; p = 0.0845).
HRQoL
The mean (SD) SGRQ-C total score at baseline was 67.12 (17.22) in the BUD/FORM plus I + T group and 65.18 (16.89) in the I + T group. Both treatment groups demonstrated improvement in SGRQ-C total score from baseline to study end, although the improvement was significantly greater in the BUD/FORM plus I + T group compared with I + T alone (p < 0.0001) (Figure 4). In the BUD/FORM plus I + T group, 62.5% of patients experienced a clinically significant improvement in SGRQ-C score (reduction of ⩾4 units) compared with 49.7% of the I + T group (p = 0.002).

Reduction in SGRQ-C total score from baseline to last available visit.
COPD symptoms and reliever use
BUD/FORM plus I + T was associated with significantly greater improvements in all three symptom components of the BSCC score (p ⩽ 0.0002) (Table 3). The use of daytime reliever medications decreased from baseline in both groups, but the reduction was significantly greater in the BUD/FORM plus I + T group than the I + T group [mean of last week on treatment 0.97 vs 1.21, respectively; between-treatment difference −0.297 (95% CI: −0.522, −0.071); p = 0.0102]. The use of reliever medication at night decreased slightly from baseline in both groups, from a mean of 0.34 doses per night at baseline to 0.26 doses per night during the last week of treatment in the BUD/FORM plus I + T group, and from 0.31 doses per night to 0.30 doses per night in the I + T group. However, the between group difference was not statistically significant [–0.055 (95% CI −0.144, 0.035); p = 0.2281].
Changes in symptom score from baseline to treatment period (FAS population).

ANCOVA, analysis of covariance; BUD/FORM, budesonide/formoterol; BSCC, Breathlessness, Cough and Sputum Scale; CI, confidence interval; I+T, ipratropium + theophylline; LS, least squares; SD, standard deviation.
Tolerability
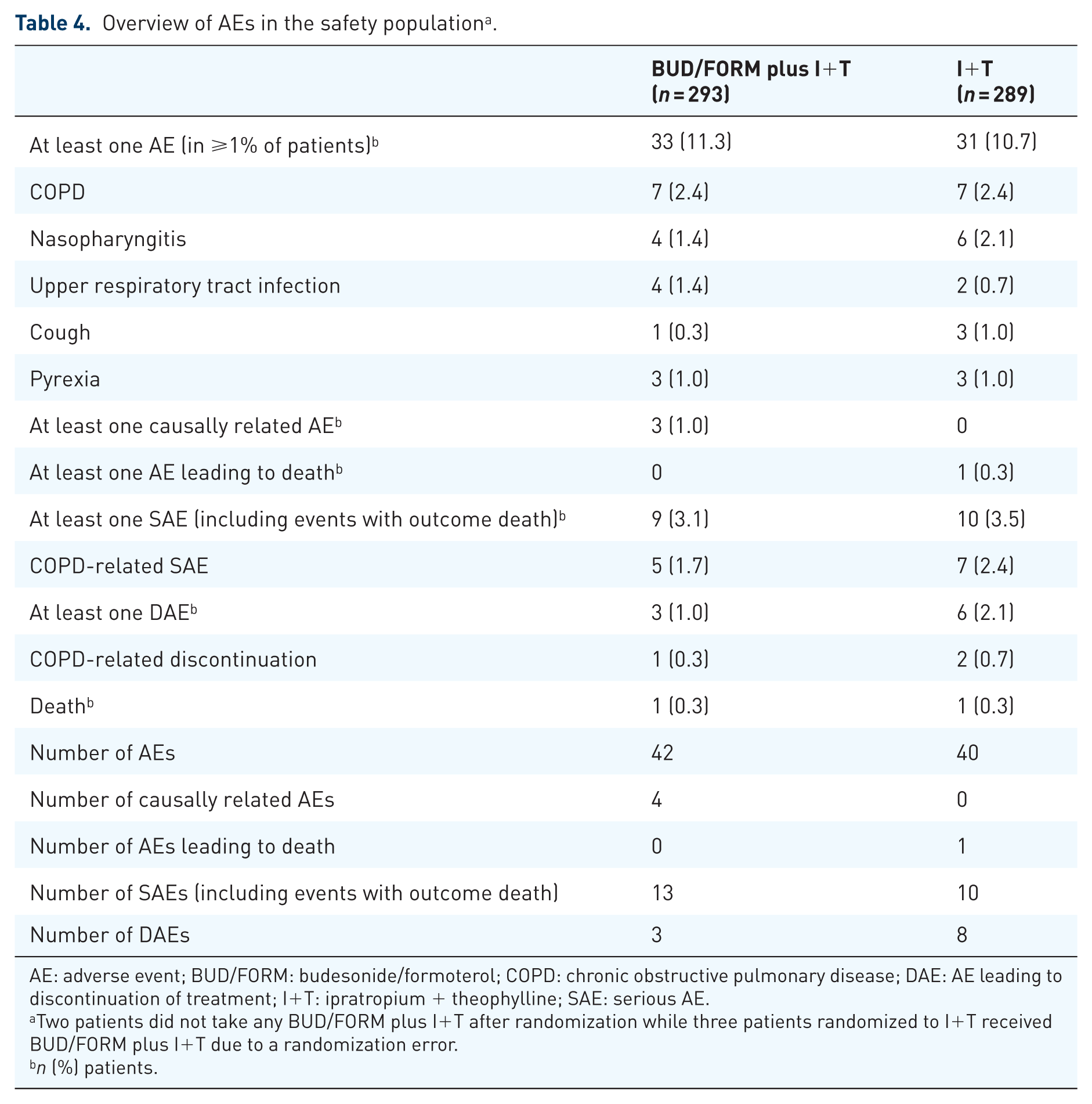
A total of 33 patients (11.3%) in the BUD/FORM plus I + T group experienced more than one AE compared with 31 patients (10.7%) who received I + T alone (Table 4). The most common AEs were respiratory disorders, which included acute exacerbation of COPD (AECOPD), nasopharyngitis, and upper respiratory tract infection. Most adverse events were mild or moderate in severity, and were similarly distributed across the two groups. In the BUD/FORM plus I + T group, 3 patients (1.03%) had treatment-related AEs (palpitations, fungal esophagitis, tuberculosis, and pneumonia), 3 (1.03%) discontinued treatment due to AEs, and 9 (1.3%) experienced at least one SAE, compared with 0 patients (0%), 6 patients (2.1%), and 10 patients (3.5%), respectively, in the I + T group. The most common SAE was AECOPD, which occurred in 1.7% of patients in the BUD/FORM plus I + T group, and 2.4% in the I + T group. Three patients in the BUD/FORM plus I + T group had AEs that investigators judged to be causally related to treatment (pneumonia, tuberculosis, and coronary artery disease in one patient, palpitations in another, and fungal esophagitis in a third), versus none in the I + T group. One patient in each treatment group died during the study; the death in the I + T group was caused by COPD and occurred during treatment, whereas the death in the BUD/FORM plus I + T group was of unknown cause and occurred 8 days after treatment completion. Neither death was considered by investigators to be related to the study treatment.
Overview of AEs in the safety population a .
AE: adverse event; BUD/FORM: budesonide/formoterol; COPD: chronic obstructive pulmonary disease; DAE: AE leading to discontinuation of treatment; I+T: ipratropium + theophylline; SAE: serious AE.
Two patients did not take any BUD/FORM plus I+T after randomization while three patients randomized to I+T received BUD/FORM plus I+T due to a randomization error.
n (%) patients.
Discussion
This 12-week, open-label study showed that treatment with BUD/FORM plus I + T resulted in greater clinical improvement in lung function than I + T treatment alone in patients with severe COPD in China. Significantly greater improvements in trough FEV1 and other lung function parameters were seen in the BUD/FORM plus I + T group compared with the I + T group. The BUD/FORM plus I + T group also demonstrated greater reduction in use of reliever medications, reductions in exacerbation rates, greater improvement in symptom scores, and a greater proportion of patients with clinically significant improvements in HRQoL. Overall, the treatments were well tolerated; the addition of BUD/FORM to I + T did not cause any new safety concerns.
This study is the first to examine the efficacy and safety of ICS/LABA (in the form of BUD/FORM) added to I + T in Chinese patients with severe COPD. The clinically important improvements in HRQoL scores and reduction in exacerbation rates in this study were consistent with those of previous studies comparing ICS/LABA combination treatment with placebo and/or ICS or LABA monotherapy in patients with COPD of similar severity (FEV1 ⩽50% predicted and FEV1/FVC ratio ⩽0.70).12–14 Similar improvements were also observed when ICS/LABA treatment was provided as an add-on therapy for patients receiving tiotropium.17,19
Our study employed prebronchodilator FEV1 as the primary endpoint. Postbronchodilator FEV1 is recommended in guidelines for COPD diagnosis, because this measurement is more sensitive than prebronchodilator FEV1 for estimating the prevalence of COPD, and has slightly better reproducibility. 20 However, the differences between the sensitivity and specificity of pre and postbronchodilator FEV1 are not marked, 20 and prebronchodilator FEV1 is more frequently used to define COPD patients for clinical trial inclusion, presumably because it may be less susceptible to methodological variation, such as in the timing of spirometry after acute bronchodilator administration, the type or dose of the acute bronchodilator, and the patient’s inhaler technique. 21 These factors may explain why a previous study showed an improvement in prebronchodilator FEV1 after 3 months of treatment with inhaled fluticasone, but no statistically significant change in postbronchodilator FEV1. 22 Therefore, while the prebronchodilator FEV1 assessment used in the current study is not consistent with COPD diagnostic guidelines, it is consistent with the criteria used to define COPD patients in most clinical trials,13,14,20 and when combined with the other selection criteria (such as the presence of symptoms and recent exacerbation), it is not likely to have led to the inclusion of patients without COPD.
The GOLD 2018 report recommends the administration of LAMA therapy as the initial treatment choice for patients with high exacerbation risk (i.e., Group C/D), with treatment escalated to a ICS/LABA, LAMA/LABA, or LAMA + LABA + ICS combination for patients who require additional treatment to reduce the risk of exacerbations. 8 A 12-week randomized controlled trial conducted by Welte and colleagues aimed to assess the clinical efficacy and tolerability of a triple-therapy approach by combining LAMA plus BUD/FORM in the management of patients with COPD in Europe. 17 The results indicated that the combination of LAMA plus BUD/FORM rapidly improved lung function, health status, morning symptoms and activities, and decreased severe exacerbations compared with LAMA alone. These results were consistent with another 12-week randomized controlled trial, which utilized the same triple-therapy approach in 587 COPD patients from East Asia (China, Hong Kong, Indonesia, South Korea, and Thailand). 23 Lung function parameters for inclusion in this study were the same as in the present study, i.e., prebronchodilator FEV1 ⩽50% predicted and FEV1/FVC ratio <0.70. 23
The rationale for adding theophylline to an ICS-containing combination lies in its suggested mechanism of action. Low-dose theophylline has been shown to have anti-inflammatory effects that are different to those of corticosteroids, including increased activation and expression of histone deacetylase (HDAC) 2, which helps to reverse corticosteroid resistance and facilitate corticosteroid sensitivity in COPD.24–26 Theophylline has been shown to significantly reduce the levels of inflammatory markers, including HDAC, in sputum of COPD patients during an acute exacerbation. 27 However, this may not be the case in stable COPD. In a small study, patients with severe COPD received theophylline or placebo, in conjunction with ICS plus salmeterol, but there was no significant difference between the groups in the incidence of exacerbations, and no differences in levels of HDAC or inflammatory markers. 28 However, combination treatments with theophylline have been shown to improve symptoms. Theophylline combined with BUD/FORM effectively reduced dyspnea, increased exercise performance, and improved pulmonary function in patients with moderate-to-severe COPD. 29 Another study found that adding theophylline to treatment with an LABA + LAMA improved symptoms in patients with moderate-to-severe COPD, but had no significant effect on objective lung function parameters. 30 Further studies are required to clarify the effect of theophylline when used in addition to ICS-containing combination therapy in patients with COPD.
While LAMA therapy is commonly prescribed in Europe, as recommended in the 2018 GOLD guidelines, it is not widely used in clinical settings in China. Other therapies, such as theophylline and SAMAs, have been commonly prescribed for Chinese patients with COPD due to their rapid-acting nature, low cost, and availability. The 2018 GOLD guidelines note the importance of individualizing treatment for each patient based not only on their response to treatment and their risk of adverse events, but on the availability and affordability of treatment. For patients in China, I + T is a relatively affordable and cost-effective option for COPD. 31 Therefore, the results of this study suggest that ICS/LABA plus SAMA and theophylline could be considered an alternative option for patients with moderate-to-severe COPD.
This was a large, multicenter, randomized study of 12 weeks’ duration. As previous studies investigating the effects of combined ICS/LABA therapy versus ICS or LABA monotherapy have typically been 6–12 months in duration,12–14,32,33 the relatively short time-frame of this study could be viewed as a limitation. However, several randomized controlled studies have now confirmed the value of 3-month studies in assessing the efficacy of ICS/LABA therapy in improving lung function and reducing exacerbations.34,35 A differential discontinuation rate was observed at the 3-month assessment despite a low drop-out rate (i.e., 5.5% in the BUD/FORM plus I + T group versus 10.4% in the I + T group). It should be noted that patients with more severe disease tend to drop out in greater numbers on less effective therapies while patients with milder disease remain. Therefore, the observed between-treatment difference is not as great as it would be. If this study had continued for a longer assessment period, the difference in discontinuation rate could have affected the robustness of the study. Another limitation of this study was the open-label design. Blinding can be difficult to achieve in respiratory studies when the inhalers differ between groups. A double-dummy technique can be used for double-blind studies, but even using a dummy inhaler may not maintain blinding if the taste or sensation of the inhalation differs between active treatment and placebo. 36 We minimized the impact of the open-label design on outcomes by randomizing patients after a run-in period in which baseline was established and by using objective assessments of lung function as the primary efficacy variable (and by blinding the spirometry technicians to the patients’ treatment groups). 36 The absence of both a placebo and BUD/FORM study arm can also be considered a limitation, as inclusion of both would be required to allow investigation of potential synergistic effects between BUD/FORM and I + T treatments. Randomization of the patient cohort into three treatment groups (BUD/FORM, I + T and BUD/FORM plus I + T ) may have permitted more detailed evidence on the comparative efficacy of the different therapies to be collected. Alternatively, two different treatment groups (BUD/FORM vs I + T) could have been compared directly. These alternative study designs could be utilized in any future studies to determine if there is need to switch treatments in patients with COPD in China, particularly given the economic burden of this disease. The 12-week duration of this study could be considered a limitation, as it is the minimum study duration regarded as sufficient to detect a treatment effect on exacerbations and provide reliable results. 37 Lastly, because this study was performed solely in Chinese patients and employed a regimen (I + T) that is largely used only in this region, these results may not be readily generalized to other patient populations.
Conclusion
Among Chinese patients with severe COPD and a history of exacerbations, treatment with BUD/FORM plus ipratropium and theophylline was associated with significant improvements in lung function, predose FEV1 and HRQoL, plus a reduction in exacerbations, compared with ipratropium and theophylline alone. Both treatments were equally well tolerated and no new or unexpected safety findings were observed.
Supplemental Material
Author_response_to_reviewers – Supplemental material for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China
Supplemental material, Author_response_to_reviewers for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China by Kewu Huang, Yanfei Guo, Jian Kang, Li An, Zeguang Zheng, Lijun Ma, Liping Peng, Hongyang Wang, Rong Su, Yohji Itoh and Chen Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China
Supplemental material, Reviewer_1_v.1 for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China by Kewu Huang, Yanfei Guo, Jian Kang, Li An, Zeguang Zheng, Lijun Ma, Liping Peng, Hongyang Wang, Rong Su, Yohji Itoh and Chen Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.2 – Supplemental material for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China
Supplemental material, Reviewer_1_v.2 for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China by Kewu Huang, Yanfei Guo, Jian Kang, Li An, Zeguang Zheng, Lijun Ma, Liping Peng, Hongyang Wang, Rong Su, Yohji Itoh and Chen Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China
Supplemental material, Reviewer_2_v.1 for The efficacy of adding budesonide/formoterol to ipratropium plus theophylline in managing severe chronic obstructive pulmonary disease: an open-label, randomized study in China by Kewu Huang, Yanfei Guo, Jian Kang, Li An, Zeguang Zheng, Lijun Ma, Liping Peng, Hongyang Wang, Rong Su, Yohji Itoh and Chen Wang in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Author contribution
Chen Wang and Kewu Huang participated in the design of the study, carried out the experiments, performed data analyses, and drafted the manuscript; Yanfei Guo and Jian Kang contributed to the study design, carried out the experiments, performed data analyses, and wrote the manuscript; Li An, Zeguang Zheng, Lijun Ma, Liping Peng, and Hongyang Wang contributed to the study design, supervised the entire project, and helped write the manuscript; Rong Su and Yohji Itoh contributed to the study design, supervised the experimental work and statistical analysis, wrote the manuscript, and supervised the entire project. All authors read and approved the final manuscript.
Funding
Funding for this study was provided by AstraZeneca and the Research Special Fund for Public Welfare of Health from Ministry of Health of the People’s Republic of China (201002008).
Conflict of interest statement
Rong Su and Yohji Itoh are current employees of AstraZeneca. Kewu Huang, Yanfei Guo, Jian Kang, Li An, Zeguang Zheng, Lijun Ma, Liping Peng, Hongyang Wang, and Chen Wang declare that they have no competing interests.
Data sharing statement
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.