
Abstract
Background:
Omalizumab may modulate airway remodeling in severe asthma. Using forced expiratory volume in 1 second (FEV1) as a surrogate of airway remodeling, we aimed to investigate if an omalizumab add-on in severe allergic asthma may lead to a persistent reversal of airway obstruction and to evaluate the potential biomarkers of airway obstruction reversibility.
Methods:
Data were collected before (T0) and after omalizumab add-on for 1 year (T1, 32 patients), 2 years (T2, 26 patients) and 4 years (T4, 13 patients). All patients had baseline FEV1 below 80 % predicted (60.5 ± 12.5 %). After omalizumab, 18 patients showed FEV1 normalization (reversible airway obstruction; RAO+) already at T1 (88.7 ± 14.9 %, p < 0.0001) that persisted up to T4 (83.2 ± 7.9, p < 0.01), while 14 patients (RAO−) had FEV1 persistently decreased, from T1 (65.2 ± 8.4%, p < 0.05) up to T4 (61.4 ± 6.2%, not significant). Both groups had significant improvement of symptoms and exacerbations after omalizumab at T1, which persisted up to T4. The comparison between pretreatment characteristics of the two groups showed that RAO+ patients, had higher values of circulating eosinophils, exhaled nitric oxide (FENO), prevalence of rhinitis and nasal polyps, need of oral corticosteroids, shorter asthma duration, higher FEV1 and response to albuterol test. The optimal cut-off points predicting FEV1 normalization after omalizumab add-on were 30.5 ppb for FENO and 305 cells/µl for eosinophils.
Conclusions:
This study suggests that omalizumab add-on contributes to the persistent reversal of airway obstruction in a consistent number of patients with severe allergic asthma, and this beneficial effect is predicted by elevated pretreatment FENO and circulating eosinophils.
Introduction
According to international European Respiratory Society (ERS)/American Thoracic Society (ATS) guidelines, severe asthma is a condition that requires high-dose inhaled corticosteroid (ICS) therapy in addition to a second controller or systemic glucocorticoids to remain ‘controlled’, or it is an asthma that remains ‘uncontrolled’ despite this therapy. 1 For patients with severe allergic asthma who remain uncontrolled or poorly controlled, add-on treatment with the anti-immunoglobulin (Ig)E omalizumab is recommended. 2 Omalizumab is a humanized recombinant monoclonal anti-IgE antibody, which binds to the high-affinity IgE receptor on mast cells and basophils, thereby inhibiting their activation by circulating IgE. This results in a milder allergic response, both in the early and late phase. A decrease in serum-free IgE levels and in the number of IgE receptors3,4 are additional effects of omalizumab. Clinical studies have shown that omalizumab results in better asthma control, fewer exacerbations, and fewer emergency department visits. According to Bousquet and colleagues, 5 the clinical response can be judged at weeks 12–16 and the benefit is more likely in patients needing high ICS doses, having worse airway obstruction and at least one asthma emergency treatment in the previous year.
Airway remodeling is an important feature of severe asthma and it is made up of various structural abnormalities, not necessarily coexistent, such as epithelium thickening, increased smooth muscle mass, vascular proliferation and subepithelial fibrosis.1,6,7 Experimental observations indicate that IgE-dependent activation of high-affinity IgE (FcεRI) receptors is involved in the maintenance of airway allergic inflammation and in airway smooth muscle cell remodeling deposing extracellular matrix. 8 Omalizumab, through its property of downregulating FcεRI expression not only on mast cells, but also on basophils and dendritic cells, has the potential to decrease airway remodeling. Roth and colleagues, 9 demonstrated in vitro that omalizumab decreases airway smooth muscle proliferation, and deposition of fibronectin and collagen type-I. Recent evidences by Riccio and colleagues, 10 and Mauri and colleagues, 11 suggest that omalizumab may interfere with cellular and molecular mechanisms underlying airway remodeling. A relevant finding by Maggi and colleagues 12 is that long-term omalizumab treatment suppresses cells involved in type 2 inflammation and, besides downregulating FcεRI expression, is also able to remove IgE from its receptor. However, the influence of omalizumab on structural alterations of the airway remains to be defined in vivo. Actually, the assessment of airway remodeling requires the analysis of tissue from bronchial biopsy. Recently Berair and colleagues, 13 published a relevant observation combining biopsy-derived features of bronchial inflammation and remodeling with both spirometry and airway morphometry assessed by quantitative computed tomography (CT). These authors found that post-bronchodilator forced expiratory volume in 1 second (FEV1) has a significant inverse correlation with airway smooth muscle thickness and vascularity either assessed by biopsy or by CT.
In a small group of patients, Hoshino and colleagues 14 found that short-term treatment with omalizumab was associated with reduced airway wall thickness, assessed by CT, and with decreased airway inflammation, assessed by sputum eosinophils. Moreover, they found that the changes in wall thickness after omalizumab were correlated with the changes in FEV1 % and in sputum eosinophils.
These findings encourage the use of lung function test as a surrogate measure for remodeling, although some rather old observations report negative results.15,16
Aim
The aim of the present study was to assess in real-life the long-term effects of omalizumab on FEV1, used as surrogate of airway remodeling, and to evaluate whether exhaled nitric oxide (FENO) and circulating eosinophils, the biomarkers previously shown to be predictors of omalizumab response, 17 may also be predictors of airway obstruction reversibility.
Methods
A single-center retrospective observational study was performed on all the consecutive adult patients who had been prescribed omalizumab for severe allergic asthma at the Severe Asthma Clinic at the University Hospital ‘Città della Salute e della Scienza’, Turin (Italy) between January 2013 and January 2017. All the patients were on omalizumab treatment for at least 1 year and had quarterly visits in the year preceding the start of omalizumab treatment, as recommended in severe asthma. 2 The study was conducted in accordance with the amended Declaration of Helsinki, and was approved by Institutional Review Board (Comitato Etico Interaziendale, CEI N. 62/2012). Patients were informed about the aim of the study and gave written consent to the anonymous use of their clinical records.
Study protocol
The primary outcome of the study was the response of airway obstruction to omalizumab, in terms of FEV1 normalization. Severe asthma was diagnosed according to the Global Initiative for Asthma (GINA) strategy. 2 Other outcomes were symptoms, based on asthma control test questionnaire (ACT), number of asthma exacerbations, FENO and circulating eosinophils. In Figure 1, a STROBE flow diagram outlines the design and conduct of the study.
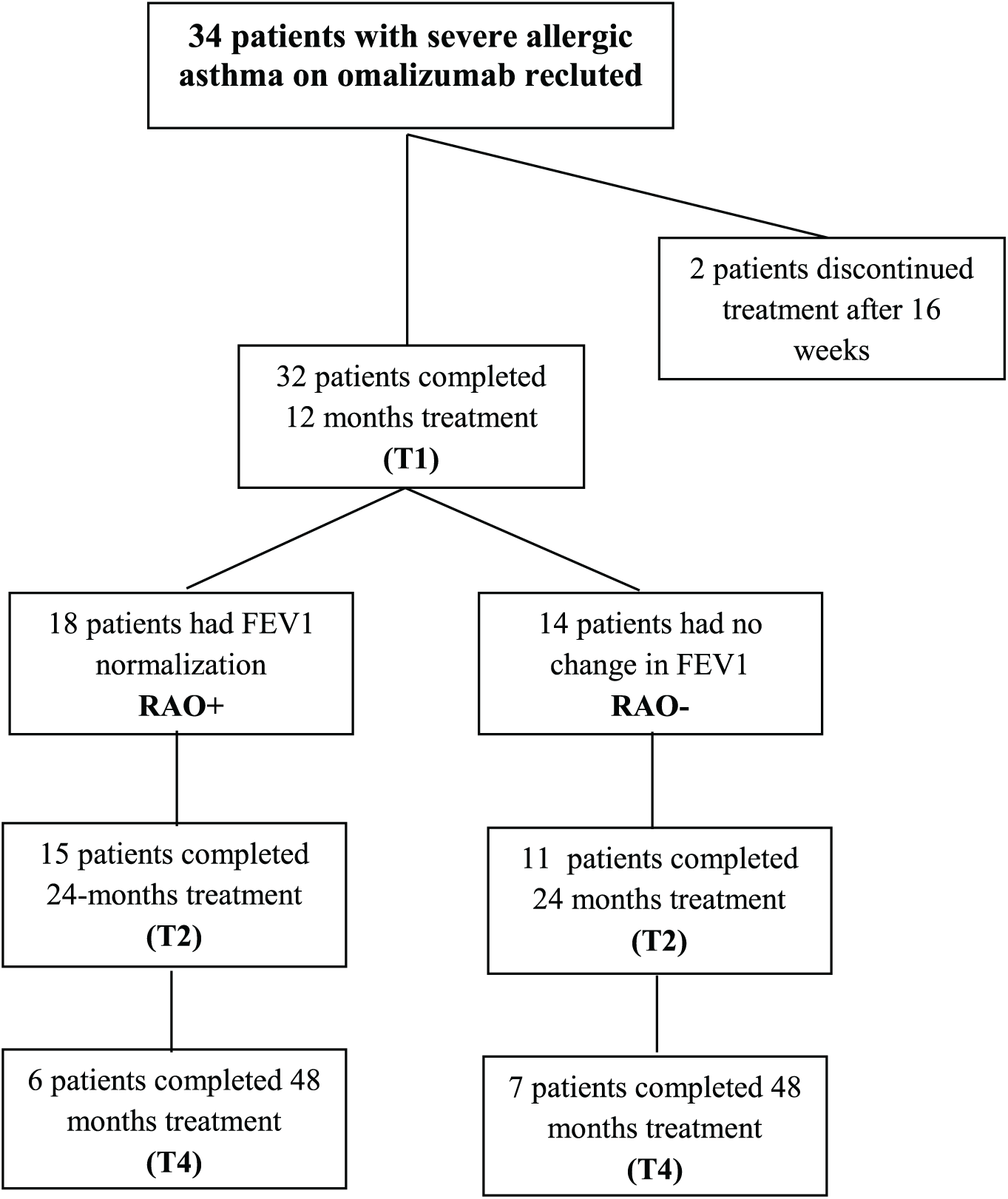
STROBE diagram of patients recruited for the study.
The medical record of each patient was retrospectively collected and reviewed to gain information concerning the year preceding the start of omalizumab add-on (baseline = T0), and after treatment for 1 year (T1, 32 patients), 2 years (T2, 26 patients) and 4 years (T4, 13 patients). Overall, two additional patients had voluntarily interrupted treatment after 16 weeks because they did not perceive improvement. Omalizumab was administered at the asthma clinic, subcutaneously, in the dose determined by the omalizumab dosing chart, using baseline IgE (30–1500 IE/ml) and body weight, every 2 or 4 weeks depending on the calculated requirement.
Data collected included demographics, smoking habits, atopy, symptoms by asthma control test (ACT), asthma exacerbations (AEs), medication use, comorbidities, lung function tests, FENO, and blood tests for circulating eosinophils and total serum IgE. Patients were classified as current, ex- and never-smokers, according to self-reported smoking history. Body mass index (BMI) was calculated as the ratio between weight and squared height (kg/m2). Atopy was defined by the presence of at least one positive skin prick test, according to the European Academy of Allergy and Clinical Immunology consensus on allergy testing. 18 Asthma medications included ICSs, long-acting beta-agonists, antimuscarinic agents (LAMAs) and oral leukotriene receptor antagonists (LTRAs). ICS dose was categorized on the basis of clinical comparability to beclomethasone dose, as suggested in the GINA strategy, 2 that is: 1 = no ICS, 2 = low (200–500 µg), 3 = medium (>500–1000 µg), 4 = high (>1000 µg).
AEs were defined according to the ATS/ERS joint statement 19 on the basis of unscheduled physician visits for acute or subacute worsening of respiratory symptoms, associated with airflow obstruction, requiring changes or higher doses of medications, need for oral corticosteroids or antibiotics, or hospitalization.
Comorbidities were recorded on the basis of prior diagnosis and current treatment for: chronic sinusitis with nasal polyps (CHRSwNP) or without (CHRSnNP), confirmed by an otorhinolaryngological evaluation or CT scan, systemic arterial hypertension, ischemic heart disease, heart failure, diabetes, anxiety or depression, chronic kidney disease, cerebrovascular disease, osteoporosis, and obstructive sleep apnea. Symptoms of CHRSwNP were assessed by three items (rated by numbers from 0 = no to 5 = as bad as it can be): nasal obstruction, loss of smell or taste, post-nasal discharge. 20 A score was calculated (range from 0 to 15). The score was reassessed after 1 year of treatment.
Lung function tests were measured using the Baires System (Biomedin, Padua, Italy). The values of slow vital capacity (VC), FEV1, and FEV1/VC% ratio, were used as markers of airway patency. VC and FEV1 were expressed either as absolute values or as the percent of predicted value. 21 Bronchodilator response was diagnosed if FEV1 increased by 12% from baseline or by 200 ml following inhalation of albuterol 400 μg. 2
FENO was measured according to ATS/ERS recommendations, 22 using a NO electrochemical analyzer (Hypair, Medisoft, Sorinnes, Belgium).
ACT, baseline spirometry, and FENO were measured at least every 3 months, so that for each patient, four measurements per year of each variable were available. To analyze the long-term trend of these variables (as markers of symptoms, airway obstruction and inflammation) before and during omalizumab treatment, the median of four values per year of ACT, FEV1, and FENO, were calculated at T0, T1, T2, T4. The use of the median value of four annual measurements overcame the influence of occasional variations caused by an exacerbation. Total IgE, circulating eosinophils and number of AE were assessed once in a year, at the start of omalizumab treatment and at T1–T2–T4.
Statistical analysis
Statistical analyses were performed with SPSS Statistical Package software, version 21 (SPSS, Chicago, IL, USA) and STATA 13.1 (Stata Corporation, College Station, TX, USA). A descriptive analysis of all variables was performed. The normality of variable distribution was assessed by the Kolmogorov–Smirnov test.
The changes of ACT, exacerbations, FEV1, FENO, circulating eosinophils after treatment with omalizumab for 1 year (32 patients), 2 years (25 patients) and 4 years (13 patients) were evaluated by paired Student’s t test. Based on the outcome at the end of the first year of treatment the patients who displayed persistent FEV1 normalization were allocated in the group of reversible airway obstruction (RAO+), and those who showed no significant change in FEV1 in the group of nonreversible airway obstruction (RAO−).
The comparison of pretreatment characteristics of the two groups was performed using the Wilcoxon–Mann–Whitney test.
The effects of several independent variables on airway obstruction reversibility were tested using univariate and multivariate logistic regression models. Due to the small number of patients, only two independent variables could be included in the multivariate model, to avoid overfitting.
An empirical estimation of the cut-off points of FENO and circulating eosinophils for identifying the reversibility of airway obstruction at T1 was established using the Liu’s method, 23 by maximizing the product of the sensitivity and specificity.
The results were considered statistically significant if the p value was below 0.05.
Results
The baseline characteristics of the 32 patients enrolled are reported in Table 1, left column. Most of the patients were women (69%), had polysensitization (69%) and chronic rhinosinusitis (66%); over half of the patients suffered from nasal polyps (53%). FENO was over 30 ppb in 15 patients (47%), circulating eosinophils were over 300 cells/µl in 23 patients (72%). A combined increase in FENO and circulating eosinophils was found in 16 patients. All the patients had airway obstruction with a trough FEV1 below 80% of predicted and 19 patients (59%) had a significant response (⩾ 12% FEV1 increase) to albuterol test. All the patients received high-dose ICSs and 12 (38%) were on chronic therapy with oral corticosteroids.
Pretreatment characteristics of the overall patients and of the subgroups with FEV1 normalization (RAO+) and without FEV1 normalization (RAO

D-FEV1 PB, percent increase in FEV1 after albuterol.
BMI, body mass index; FEV1, forced expiratory volume in 1 second; FENO, exhaled nitric oxide; Ig, immunoglobulin; NS, not significant; RAO, reversible airway obstruction; SD, standard deviation.
The results obtained in the overall patients, before and during treatment with omalizumab, are summarized in Table 2. Omalizumab was well tolerated and only two patients experienced local side effects, consisting in mild injection-site reactions (with no need of treatment discontinuation). After 1 year of treatment (T1), FEV1, FENO, eosinophils, ACT and AEs were all significantly improved. The improvement was maintained at 2 years (T2), with a further significant decrease in the number of AEs, compared with T1. In the 13 patients who completed 4 years of treatment, the improvement in FEV1, ACT, and AEs remained stable, with no significant difference from T2. During treatment, none of the patients needed an emergency room visit or hospitalization for asthma.
Changes from baseline (T0) after 1 (T1), 2 (T2) and 4 (T4) years of omalizumab treatment in the overall patients.

FEV1, forced expiratory volume in 1 second; FENO, exhaled nitric oxide; Ig, immunoglobulin.
The primary endpoint of this study, that is FEV1 normalization as marker of reversible airway obstruction+), occurred in 18 patients at the first year of treatment, while in the remaining 14 patients (RAO−) airway obstruction persisted throughout treatment.
The comparison between the pretreatment characteristics of the two groups, displayed in Table 1, showed that RAO+ patients had higher circulating eosinophils, higher FENO, higher prevalence of rhinitis and nasal polyps, higher need of chronic oral corticosteroids treatment, shorter asthma duration, slightly better FEV1, and better response to albuterol test. A total of 15 RAO+ patients (83%), but only 1 RAO− (7%), had a combined increase in FENO and circulating eosinophils. No significant difference was found between the two groups in the prevalence of arterial hypertension, cardiovascular disease, depression, osteoporosis and gastroesophageal reflux disease.
The results of the univariate and multivariate analyses for evaluating the influence of several independent variables on airway obstruction reversibility are displayed in Table 3. The univariate analysis showed that RAO+ was associated with increased pretreatment FENO, circulating eosinophils, bronchodilator response, shorter asthma duration, history of rhinitis and nasal polyps. Multivariate analysis confirmed the association of RAO+ with FENO and circulating eosinophils.
Results of univariate and multivariate analysis on the predictors of airway obstruction reversibility after omalizumab.

D-FEV1 PB, percent increase in FEV1 after albuterol.
CI, confidence interval; FEV1, forced expiratory volume in 1 second; FENO, exhaled nitric oxide; Ig, immunoglobulin; OR, odds ratio.
The results obtained before and during treatment with omalizumab by reversibility are summarized in supplementary Table S1 for RAO+ and Table S2 for RAO− patients. Both groups showed a significant increase in ACT and a decrease in exacerbation rate after omalizumab, that persisted up to the fourth year of treatment and no significant difference in the mean value of ACT and AE number was found between the two groups at any time. Oral corticosteroids treatment could be withdrawn in 8 of the 16 RAO+ patients (from 89 to 39%, p = 0.023) and in 3 of the 8 RAO− patients (from 57 to 36%, not significant). ICS dosage was decreased from class 4 to class 3 in 15 RAO+ patients (83%, p < 0.001) and in 5 RAO− patients (36%, p = 0.041).
RAO+ patients, together with persistent FEV1 normalization, had also a significant decrease in FENO and circulating eosinophils.
RAO− patients had a FEV1 persistently below the normal range, although transiently increased at T1, and showed no change in FENO and circulating eosinophils.
As regards nasal polyps, during omalizumab treatment 2 RAO+ and 1 RAO− patients underwent Functional Endoscopic Sinus Surgery (FESS) intervention. The CHRSwNP score was significantly improved in the 13 in RAO+ patients (from 13.2 ± 1.7 before to 9.6 ± 2.5 after omalizumab, p < 0.001) and unchanged in the 5 RAO− patients (from 14.2 ± 1.3 before to 11.6 ± 2.7 after omalizumab, p = 0.144).
In Figure 2 are graphically the changes (expressed as percent of pretreatment value) in ACT, AE, FEV1, FENO, and circulating eosinophils at T0, T1 and T2 after treatment with omalizumab in RAO+ (15 patients) and RAO− (10 patients) and in Figure 3 are shown data of patients who completed 4 years treatment (7 patients RAO+ and 6 patients RAO−). In both groups, the improvement of symptoms and number of exacerbations persisted up to four year of treatment, while the improvement of FEV1, together with FENO and eosinophils, occurred and persisted only in RAO+.

Changes in FEV1, ACT, FENO, AE, and circulation EOSs during omalizumab add-on for 1 year (T1) and 2 years (T2) in patients with FEV1 normalization (RAO+) and in those with persistent airway obstruction (RAO−).

Changes in FEV1, ACT, FENO, AE, and circulation EOSs during omalizumab add-on for 1 (T1), 2 (T2) and 4 (T4) years in patients with FEV1 normalization (RAO+) and in those with persistent airway obstruction (RAO−).
The comparison between the two groups of FEV1% predicted median values, according to the two-sample Wilcoxon–Mann–Whitney rank-sum test, gave a z = −2.128 (p = 0.033) at baseline, a z = −4.221 (p = 0.000) at T1, a z = −4.261 (p = 0.000) at T2, and a z = −2.022 (p = 0.027) at T4.
The results of the empirical estimation of FENO and eosinophils cut-off points for RAO, according to Liu analysis 22 are reported in Figure 4. The optimal cut-off points to predict FEV1 normalization after omalizumab treatment were a FENO value of 30.5 ppb and a number of circulating eosinophils of 305 cells/µl.

Summary of ROC curves for FENO and circulating eosinophils cut-points estimation to predict FEV1 normalization after omalizumab add-on. 23
Discussion
The primary aim of this single-center real-life observational study was to assess whether long-term treatment with omalizumab in patients with severe allergic asthma may lead to a persistent reversal of airway obstruction and to evaluate whether inflammatory biomarkers, such as FENO and circulating eosinophils, may predict airway obstruction reversibility. The results of the study indicate that omalizumab effectively reversed airway obstruction in over half of the 32 patients (56%), maintaining this beneficial effect in the long term. This effect was predicted by increase pretreatment values of FENO and circulating eosinophils and seemed to be independent of the relief of symptoms and of the reduction of exacerbations. In fact, the same significant improvement in ACT and AE number observed in RAO+ patients was observed in the 14 patients who showed no significant improvement in airway obstruction after omalizumab, either after 2 or 4 years of treatment. Actually, most RAO+ patients (83%), but only one RAO− (7%) had combined increase in FENO and circulating eosinophils before omalizumab add-on.
Increased FENO and peripheral eosinophils indicate underlining Th2 inflammation. 17 We may suppose that in RAO+ patients, airway obstruction was driven by inflammation and eosinophil infiltration, which dampened after omalizumab treatment. The efficacy of omalizumab in suppressing cells involved in type 2 inflammation is sustained by recent observations.12,17
In contrast, in RAO− patients, the poor reversibility of airway obstruction suggests that remodeling was characterized mainly by subepithelial fibrosis. Nevertheless, in these patients, after omalizumab add-on, symptoms and exacerbations were significantly improved and FEV1 remained stable throughout the follow up. The benefit of omalizumab add-on in severe asthma control is widely demonstrated and consists in decreased rate of exacerbations, of asthma-related access to the emergency room or hospitalizations, and in an improvement of asthma-related symptoms and quality of life, enabling a significant reduction in the dose of ICSs or oral corticosteroids.17,24–30 In our patients, the withdrawal of oral corticosteroids was significant only in the RAO+ group (from 89 to 39% of patients) and not in RAO− (from 57 to 36%), while ICSs were significantly decreased in both groups, from class 4 to class 3 in 83% of RAO+ and in 39% of RAO− patients. Probably, the patients in whom omalizumab was mostly effective in reducing corticosteroids were those with greater inflammation and greater airway obstruction reversibility.
Interestingly, RAO+ patients had a higher prevalence of nasal polyps and showed a significant improvement in nasal polyp symptoms after omalizumab add-on. The benefit of anti-IgE therapy in reducing nasal polyp score in patients with severe comorbid asthma is reported in a recent meta-analysis. 31 Unfortunately, in our study nasal polyp score was assessed by a symptom questionnaire and not by endoscopy.
In establishing FEV1 normalization as the main outcome, our study has brought out more clearly some omalizumab benefits. Actually, even if in the literature the effect of omalizumab in improving FEV1 has been widely investigated, there are no studies specifically exploring whether and to what extent treatment induces FEV1 normalization. In randomized placebo-controlled trials, significant FEV1 improvements have been reported in asthma patients treated with omalizumab.28–30 In a retrospective pooled analysis, Busse and colleagues 32 found a modest, but significant improvement in FEV1 in the omalizumab group compared with the placebo group. In the INNOVATE study, 28 Humbert found that only 44% of patients had at least a 200 ml improvement in FEV1 but the increase was significantly better with omalizumab than with a placebo. Paganin and colleagues 33 found that FEV1 improved at 6 months and remained stable for 2 years only in omalizumab responder patients. Pelaia and colleagues 34 and Yorgancıoğlu and colleagues 35 found a significant improvement in FEV1 after 1 and 5 years of omalizumab treatment.
To our knowledge, this is the first study to examine the recovery of airway obstruction as a response to omalizumab. This beneficial effect occurred in patients with greater degree of inflammation before treatment, as proven by the elevation of FENO and circulating eosinophils, which are recognized biomarkers of asthma severity and inflammation. Based on an empirical estimation of the cut-off points of the two biomarkers predicting FEV1 normalization, we would propose a FENO value equal or over 30.5 ppb and a number of circulating eosinophils equal or over 305 cells/µl as predictors of airway obstruction reversibility after omalizumab add-on.
We aware that our study has several limitations. First, this is a single-center study with a limited number of patients. However, a single center has the advantage of repeatability of the measurements using the same instruments, which is relevant in long-term follow-up observations. Second, being a ‘real-life’ study, it lacks a placebo control group. Third, we did not measure serum periostin, a recognized biomarker of Th2 high eosinophilic asthma. 36 However, at the start of the study, this property of periostin had not yet been recognized.
In conclusion, this study suggests that omalizumab add-on, besides improving symptoms and decreasing disease exacerbations, may lead to a persistent reversal of airway obstruction in a consistent proportion of patients with severe allergic asthma. This beneficial effect is predicted by elevated pretreatment FENO and circulating eosinophils.
Supplemental Material
Supplementary_tables_TAR_841274 – Supplemental material for Predictors of reversible airway obstruction with omalizumab in severe asthma: a real-life study
Supplemental material, Supplementary_tables_TAR_841274 for Predictors of reversible airway obstruction with omalizumab in severe asthma: a real-life study by Paolo Solidoro, Filippo Patrucco, Francesca de Blasio, Luisa Brussino, Michela Bellocchia, Davide Dassetto, Emanuele Pivetta, Annamaria Riccio, Enrico Heffler, Walter Canonica, Giovanni Rolla and Caterina Bucca in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors would like to thank Springer Healthcare Communications for publication fees assistance. This unconditional support was funded by Novartis Farma, Italy.
P. S. and C.B. were involved in the study design, in the data collection, interpretation of data and in drafting the article. F.P., F.dB., M.B., L.B., D.D., E.H. and A.R. were involved in the acquisition and collection of data. E.P. and F.dB performed statistical analysis. W.C., E.H. and G.R. were involved in the critical discussion of data and drafting the article. All the authors have given final approval of the version to be published.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Novartis, that markets omalizumab, has not paid any fee to us for the collection of data and the preparation of the manuscript but supported the publication fee through Springer Healthcare Communications.
Conflict of interest statement
C.B. received lecture fees from AstraZeneca, Guidotti-Malesci, Menarini, Novartis. W.C. received research grants as well as lecture or advisory board fees from A. Menarini, AstraZeneca, Boehringer Ingelheim, Chiesi Farmaceutici, Genentech, Guidotti-Malesci, Glaxo Smith Kline, Mundip-harma, Novartis, Sanofi-Aventis, Teva. G.R. received lecture fees from Allergy Therapeutics.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.