
Abstract
Background:
Endoscopic lung volume reduction coil (LVRC) treatment is a therapeutic option for selected patients with advanced emphysema. The effects and the safety of endoscopic lung volume reduction in patients with very low forced expired volume in one second (FEV1) remain to be determined. This study was conducted to assess the effects and the safety of LVRC treatment in patients with very low FEV1.
Methods:
The study was performed as a retrospective observational study in the Department of Respiratory Medicine at the University Medical Center Hamburg-Eppendorf on patients with very low FEV1, defined as an FEV1 ⩽ 20% of predicted at baseline in whom LVRC treatment was performed between 1 April 2012 and 28 February 2017.
Results:
LVRC treatment was performed in 33 patients with very low FEV1. Of these, 45.5% were female and 54.5% were male. At baseline, mean FEV1 was 0.46 ± 0.12 liters (15 ± 3% of predicted), mean forced vital capacity (FVC) was 1.61 ± 0.62 liters (42 ± 13% of predicted), mean residual volume (RV) was 6.03 ± 0.81 liters (275 ± 51% of predicted) and 6-minute walk distance was 229 ± 102 m. Bilateral LVRC treatment was completed in 21 of these patients (63.6%). Bilateral LVRC treatment led to significant improvements in functional parameters with an increase in mean FEV1 from 0.44 ± 0.11 liters to 0.54 ± 0.12 liters (p = 0.001), equivalent to a relative improvement of 24.5 ± 26.9%, an increase in mean FVC from 1.49 ± 0.54 liters to 1.84 ± 0.49 liters (p = 0.001), a decrease in mean RV from 6.27 ± 0.83 liters to 5.83 ± 1.09 liters (p = 0.004) and an improvement in 6-minute walk distance from 218 ± 91 m to 266 ± 96 m (p = 0.01). There were no cases of respiratory failure requiring mechanical ventilation and no deaths.
Conclusions:
LVRC treatment was effective and safe in patients with very low FEV1.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) constituted of small airway disease and emphysema is a chronic pulmonary condition with high morbidity and mortality. 1 Emphysema is characterized by the destruction of lung parenchyma with consecutive reduction of gas exchange surface, loss of elastic recoil and hyperinflation. Hyperinflation is a key pathophysiological component that is acknowledged to be clinically relevant due to its contribution to dyspnea, exercise intolerance and reduction in quality of life. 2 Both static characteristics and dynamic processes contribute to hyperinflation. Dynamic hyperinflation is encountered with increasing breathing frequency as progressive amounts of air are being trapped within the lungs. The onset of dynamic hyperinflation is dependent on disease severity and will occur at ever lower minute ventilations as disease severity progresses. 3
Therapeutic options for patients with emphysema are limited. An approach targeting hyperinflation is lung volume reduction, which can be considered in selected patients with advanced emphysema. 4 Methods for lung volume reduction include lung volume reduction surgery 5 and interventional bronchoscopic procedures including one-way valves, 6 bronchoscopic thermal vapor ablation 7 and coils. 8 Careful patient selection is mandatory before lung volume reduction to ensure benefit and safety. The original procedure for lung volume reduction, lung volume reduction surgery, has been investigated in the national emphysema treatment (NET) trial. 5 An interim analysis identified the subgroup of patients with very low forced expired volume in one second (FEV1), defined as an FEV1 ⩽ 20% of predicted and either a homogeneous distribution of emphysema on computed tomography or a diffusion capacity ⩽20% of predicted, to be at high risk of death after lung volume reduction surgery and also to be unlikely to benefit from the surgery. 9 Data on endoscopic lung volume reduction in patients with very low FEV1 are scarce. Recently, two retrospective observational studies on lung volume reduction with valves in patients with very low FEV1 have been published. Darwiche and colleagues reported on 20 patients with very low FEV1 and concluded that endoscopic lung volume reduction with endobronchial valves could achieve improvements in lung function and exercise capacity and could be performed safely in this group of patients. 10 Trudzinski and colleagues reported on 20 patients with very low FEV1 and concluded that endoscopic lung volume reduction with endobronchial valves was generally feasible and safe. 11
To our knowledge, there are no published data on endoscopic lung volume reduction coil (LVRC) treatment in patients with very low FEV1. We therefore conducted this observational study on LVRC treatment in patients with very low FEV1 to assess the effects and the safety of LVRC treatment in this group of patients.
Materials and methods
Study design
The study was designed as a retrospective observational study. It was conducted in the Department of Respiratory Medicine at the University Medical Center Hamburg-Eppendorf, Germany. All patients with very low FEV1, defined as an FEV1 ⩽ 20% of predicted, in whom LVRC treatment was performed were included in the study, provided the availability of complete datasets for analysis. The ethics committee of the Hamburg Chamber of Physicians waived the need for ethics approval and for the need to obtain consent for the collection, analysis and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Data collection
All cases of LVRC treatment were retrieved from the electronic endoscopic database (Endobase, version 12.0, Olympus, Tokyo, Japan) by searching within a time frame between 1 April 2012 and 28 February 2017. Patient characteristics, details of the LVRC procedure and data collected during initial assessment and follow-up visits, including the results of the assessments of pulmonary function and exercise capacity, were then collected from the electronic patient database, including the electronic patient record (Soarian Clinicals, version 3.00, Cerner Health Services, USA).
LVRC treatment
The departmental routine in the evaluation, procedural performance and follow up of patients undergoing LVRC treatment was performed as previously described. 12 All patients with advanced emphysema are evaluated considering lung volume reduction surgery, different techniques of endoscopic lung volume reduction and lung transplantation. Lung volume reduction is considered in patients with emphysema phenotype, symptoms despite optimal medical therapy and pulmonary rehabilitation, severe or very severe airflow obstruction as defined by the global initiative for chronic obstructive lung disease (GOLD) definition, hyperinflation at the time of this study with a residual volume (RV) of more than 175% of predicted and the absence of active infection. High-resolution computed tomography scans with multiplanar reconstructions are required for evaluation in all patients prior to lung volume reduction. At the time of this study, densitometry software was not routinely used for analysis in our department. The distribution of emphysema was assessed visually on the basis of the computed tomography images. To select the appropriate technique, the distribution of emphysema, the degree of tissue destruction, the evaluation of interlobar collateral ventilation and comorbidities are taken into account. While the importance of the distribution of emphysema for the selection of the appropriate technique is greatly diminished since the publication of the IMPACT trial showing that treatment with one-way valves is also effective in patients with homogeneous emphysema, 13 at the time of this study homogeneous emphysema, the presence of collateral ventilation in patients with heterogeneous emphysema and sufficient tissue to anchor the coils were among the criteria in favor of LVRC treatment.
LVRC treatment is performed bilaterally in two sequential procedures unless complications or contraindications arise or the patient opts for unilateral treatment only. The aim is to complete the second procedure 1–3 months after the first procedure. The targeted lobe and the sequence are selected according to the distribution of emphysema and the degree of tissue destruction, with the upper lobes being preferentially treated in patients with homogeneous emphysema.12,14,15
Assessment of pulmonary function and exercise capacity
In patients with LVRC treatment, pulmonary function and exercise capacity are assessed in a standardized manner at baseline, between the first and second LVRC treatment and at each follow-up visit. Outpatient follow-up visits are routinely scheduled between the first and second treatment approximately 1 month after the first treatment, and 3 months after the second treatment. Pulmonary function tests including spirometry, body plethysmography and carbon monoxide uptake, as well as blood gas analyses, are performed according to the American Thoracic Society and European Respiratory Society guidelines.16–20 Exercise capacity is assessed using the 6-minute walk test. 21 Improvements in FEV1, RV or 6-minute walk distance were defined to be clinically important if FEV1 increased by ⩾100 ml, 22 RV decreased by ⩾0.35 L 23 or 6-minute walk distance increased by ⩾25 m. 24 Pulmonary function tests and 6-minute walk tests are performed with the patient under optimal pharmacological bronchodilatative therapy.
Adverse events
The electronic patient record was systematically reviewed for adverse events. As routine standard of care, patients after LVRC treatment are questioned about changes in dyspnea and the occurrence of hemoptysis or chest pain on a daily basis during hospitalization and at each outpatient follow-up visit. Any complications encountered during bronchoscopy as well as respiratory failure requiring mechanical ventilation, pneumothoraces, respiratory infections, COPD exacerbations within 3 months of the procedure, pleuritic pain associated with the position of coils and hemoptysis were considered adverse events.
Data analysis
Categorical variables are presented as absolute numbers and percentages. Continuous variables are presented as mean and standard deviation if normally distributed and as median and range if not normally distributed. Comparisons were performed using the t test for metric data. A two-sided p value below 0.05 was considered significant. The software used for statistical analyses was SPSS version 21.0 (SPSS Inc., Chicago, IL, USA).
Results
Case selection
A total of 125 LVRC procedures were performed in 79 patients between 1 April 2012 and 28 February 2017. Among these were 37 patients with very low FEV1. Complete datasets were available for 33 patients, which were included in this study. Bilateral LVRC treatment was completed in 21 of these patients (63.6%). The process of case selection is illustrated in Figure 1. To determine the fate of the four patients excluded from the study due to incomplete datasets, the referring pulmonologists or general practitioners were contacted and asked to provide information on follow up. It could be determined that one patient, who underwent unilateral LVRC treatment in our department, moved away and successfully completed bilateral LVRC treatment in another hospital. Two other patients were being followed up outside our department. In one of these cases, it could be determined that the patient is alive to date 24 months after LVRC treatment. In the other case, only short-term follow-up data could be obtained stating that the patient was doing well and had experienced improvements in dyspnea and lung function after LVRC treatment. In the one remaining case, the contacted physician declined to provide information. It could, however, be determined that this patient was alive for at least 18 months after LVRC treatment. Data sufficient for detailed analysis of functional parameters or adverse events could not be obtained in any of these cases.

Flow diagram illustrating the process of case selection.
Characteristics of patients at baseline
A total of 33 patients were included in the study. Of these, 45.5% were female and 54.5% were male. Mean age was 60 ± 8 years. In addition to optimal pharmacological therapy for their pulmonary disease, which was present in all patients, 51.5% of patients were on long-term oxygen therapy due to chronic hypoxemia and 27.3% were on intermittent non-invasive ventilation. Emphysema was distributed homogeneously in 69.7% and heterogeneously in 30.3% of cases. At baseline, mean FEV1 was 0.46 ± 0.12 liters (15 ± 3% of predicted), mean RV was 6.03 ± 0.81 liters (275 ± 51% of predicted), mean forced vital capacity (FVC) was 1.61 ± 0.62 liters (42 ± 13% of predicted) and mean 6-minute walk distance was 229 ± 102 m. Single-breath diffusion capacity for carbon monoxide (DLCO) at baseline could be determined in only 20 patients. In the other cases, VC was too low to reliably determine DLCO. For the 20 patients in whom DLCO could be determined at baseline, it was 1.67 ± 1.17 mmol/min/kPa (18 ± 13% of predicted). It has been described above that the interim analysis of the NET trial identified patients with an FEV1 ⩽20% of predicted and either a homogeneous distribution of emphysema on computed tomography or a DLCO ⩽20% of predicted to be at high risk of death after lung volume reduction surgery. In our study, as defined in the inclusion criteria, all 33 patients had an FEV1 ⩽20% of predicted. The distribution of emphysema was homogeneous in 23 of these patients. Of the 10 patients with heterogeneous emphysema, DLCO could be determined in seven patients. Three of these patients had a DLCO > 20% of predicted, the other four patients had a DLCO ⩽ 20% of predicted. In the remaining three patients with heterogeneous emphysema, VC was too low to reliably determine DLCO. It may therefore be presumed that their DLCO was also ⩽20% of predicted. Overall, definitely 27 patients (81.8%) and, including those in whom DLCO could not be reliably determined due to low VC, probably 30 patients (90.9%) included in this study met the criteria for high risk identified in the NET trial. Characteristics of patients at baseline are summarized in Table 1.
Characteristics of patients at baseline.
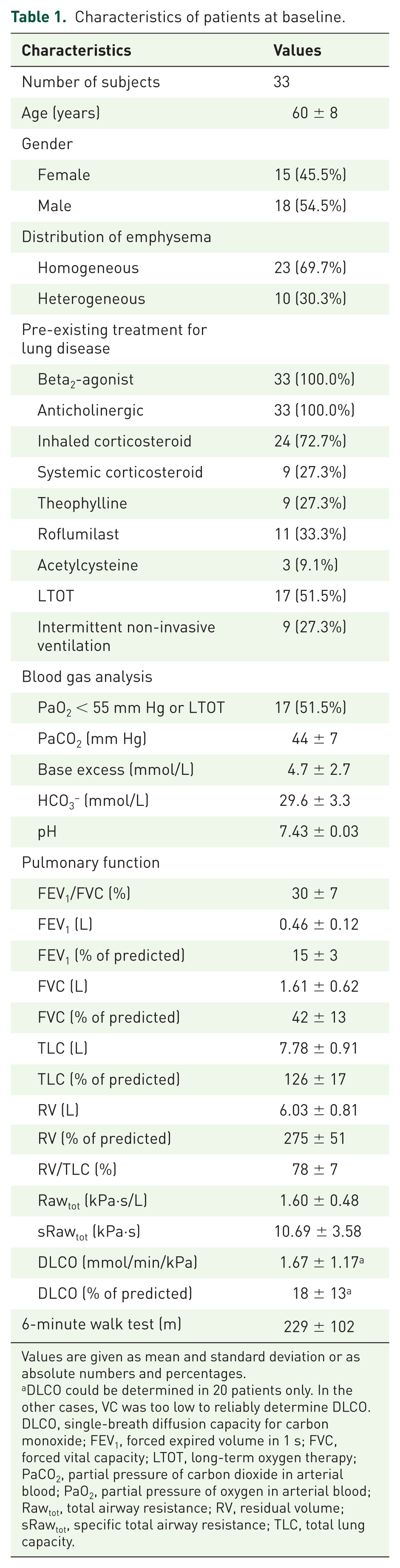
Values are given as mean and standard deviation or as absolute numbers and percentages.
DLCO could be determined in 20 patients only. In the other cases, VC was too low to reliably determine DLCO.
DLCO, single-breath diffusion capacity for carbon monoxide; FEV1, forced expired volume in 1 s; FVC, forced vital capacity; LTOT, long-term oxygen therapy; PaCO2, partial pressure of carbon dioxide in arterial blood; PaO2, partial pressure of oxygen in arterial blood; Rawtot, total airway resistance; RV, residual volume; sRawtot, specific total airway resistance; TLC, total lung capacity.
Characteristics of the LVRC procedure
Bilateral LVRC treatment was completed in two sequential procedures in 21 patients (63.6%). In 12 patients (36.4%), LVRC treatment was performed unilaterally only. Reasons why only unilateral treatment was performed were COPD exacerbations or respiratory infections in nine cases and patient’s request in three cases. Characteristics of the 54 LVRC procedures are shown in Table 2.
Characteristics of the LVRC procedures.

Values are given as absolute numbers and percentages or as median and range.
LVRC, lung volume reduction coil.
Adverse events
Hemoptysis occurred in the first days after 42 of the 54 LVRC procedures (77.8%). In all but two cases, hemoptysis was mild and self-limiting. In the two remaining cases, hemoptysis required readmission to hospital. In one of these cases bronchial artery embolization was required to terminate the bleeding. This specific patient was on antiplatelet medication with acetyl salicylic acid, but not on any other anticoagulants. Platelet count and international normalized ratio were within the normal range. There were no signs of severe pulmonary hypertension. Exacerbations of COPD were observed within 3 months after 25 of the 54 LVRC procedures (46.3%). Of these cases, eight required readmission to hospital. Pneumonia was observed after 3 of the 54 LVRC procedures (5.6%). Of these cases, two required readmission to hospital. In summary, severe adverse events requiring readmission to hospital occurred after 12 of the 54 LVRC procedures (22.2%). All other adverse events resolved spontaneously or with routine medical care. There were no adverse events during bronchoscopy. There were no cases of respiratory failure requiring mechanical ventilation and no deaths. There were no coil-associated opacities. A summary of adverse events is provided in Table 3.
Adverse events within 3 months after the LVRC procedures.

Values are given as absolute numbers and percentages.
COPD, chronic obstructive pulmonary disease; LVRC, lung volume reduction coil.
Outcome
After bilateral LVRC treatment there was a significant increase in mean FEV1 from 0.44 ± 0.11 liters to 0.54 ± 0.12 liters (p = 0.001), equivalent to a relative improvement of 24.5 ± 26.9%; a significant increase in mean FVC from 1.49 ± 0.54 liters to 1.84 ± 0.49 liters (p = 0.001); a significant decrease in mean RV from 6.27 ± 0.83 liters to 5.83 ± 1.09 liters (p = 0.004); and a significant increase in mean 6-minute walk distance from 218 ± 91 m to 266 ± 96 m (p = 0.01) compared to baseline. Improvements defined to be clinically important were seen for FEV1 in 42.9%, for RV in 57.1% and for 6-minute walk distance in 66.7% of patients. Follow-up values in patients completing bilateral treatment were collected at a median of 84 days after the first procedure and at a median of 49 days after the second procedure. In patients treated unilaterally only, there was a significant increase in FEV1 from 0.49 ± 0.13 liters to 0.60 ± 0.16 liters (p = 0.02), equivalent to a relative improvement of 25.7 ± 26.5%. Changes in mean FVC (from 1.83 ± 0.67 liters to 2.13 ± 0.72 liters, p = 0.13), mean RV (from 5.61 ± 0.56 liters to 5.78 ± 0.77 liters, p = 0.26) and mean 6-minute walk distance (from 245 ± 115 m to 223 ± 90 m, p = 0.59) were not significant. Follow-up values in patients treated only unilaterally were collected at a median of 70 days after the procedure. Changes in functional parameters are illustrated in Figure 2.

Functional parameters at baseline and follow up for patients completing bilateral lung volume reduction coil (LVRC) treatment and for patients with unilateral treatment only.
Discussion
In this retrospective observational study, we analyzed 33 patients with very low FEV1, defined as an FEV1 ⩽20% of predicted in whom LVRC treatment was performed. LVRC treatment was found to be effective and safe in this group of patients.
The degree of airflow limitation, although recognized not to be satisfactory as an isolated parameter,25,26 has been correlated with mortality in patients with COPD. 27 Therefore, an FEV1 <25% of predicted has been listed among the criteria for referral to a lung transplant center and an FEV1 <15–20% of predicted has been suggested as an indication for listing for lung transplantation. 28 However, with the use of the lung allocation score, patients with COPD receive lower priority and hence spend more time on the waiting list. 29 Therefore, therapeutic options to alleviate symptoms and improve or maintain nutritional status and exercise capacity while on the waiting list are needed. As a bridge to lung transplantation, lung volume reduction may help ameliorate or preserve the patient’s clinical status and help reach the time of surgery.30,31 The majority of patients with emphysema will, however, not be suitable candidates for lung transplantation. In this setting, while not being applied as a bridge to lung transplantation, lung volume reduction presents a symptom-modifying treatment approach.
LVRC treatment has been shown to improve lung function, exercise capacity and quality of life in patients with emphysema.14,32–34 The REVOLENS trial and the RENEW trial are the largest randomized trials on LVRC treatment published to date, including 100 and 315 patients respectively. The REVOLENS trial included patients with an RV >220% of predicted and showed improvements in lung function and quality of life in the 50 patients randomized to receive LVRC treatment. 15 The RENEW trial eventually included patients with an RV ⩾175% of predicted and showed that improvements in lung function and quality of life were more pronounced in patients with severe hyperinflation defined as an RV ⩾225% of predicted and with a heterogeneous distribution of emphysema. 8 It has to be noted that in the REVOLENS trial mean FEV1 at baseline was 25.7 ± 7.5% of predicted and patients with an FEV1 <15% of predicted were excluded from participation, and in the RENEW trial mean FEV1 at baseline was 25.7 ± 6.3% of predicted, indicating that FEV1 was not very low in the majority of patients included in these trials. In our study, mean FEV1 at baseline was very low, at 15 ± 3% of predicted. After bilateral LVRC treatment in these selected patients with very low FEV1, we observed statistically significant and clinically important improvements in FEV1, RV and 6-minute walk distance.
Very low FEV1 puts the patient at an increased periprocedural risk due to limited functional reserves, especially in the event of complications. Indeed, very low FEV1 in combination with either a homogeneous distribution of emphysema on computed tomography or a very low diffusion capacity has been reported to increase mortality associated with lung volume reduction surgery. 9 LVRC treatment has been shown to have a good safety profile.35,36 The REVOLENS trial reported 17 severe adverse events within 1 month of the procedure (four COPD exacerbations, three pneumothoraces, one case of hemoptysis, one case of thoracic pain, five cases of pneumonia, one cardiovascular event and two others), as well as one death that was however due to peritonitis. 15 The RENEW trial reported major complications after LVRC treatment including pneumonia requiring hospitalization and other potentially life-threatening or fatal events in 34.8% of cases and other serious adverse events including COPD exacerbations, pneumonia and pneumothorax in 27.7%, 20.0% and 9.7% of cases respectively. 8 LVRC in patients with very low FEV1 in our study was shown to have an acceptable safety profile with severe adverse events requiring readmission to hospital occurring after 12 of the 54 procedures (22.2%). There were no cases of respiratory failure requiring mechanical ventilation and no deaths. For endoscopic lung volume reduction with valves in 20 patients with very low FEV1, Darwiche and colleagues reported four cases of pneumothorax (20%) – of which two were treated with video-assisted thoracoscopic surgery and two with drainage – three cases of pneumonia and two exacerbations of COPD. 10 Trudzinski and colleagues reported five cases of pneumothorax (25%) and three exacerbations of COPD (15%), stating that the greatest risk of the procedure was pneumothorax with prolonged chest tube duration. 11 Exacerbations of COPD and pneumonia were equally observed in our study on LVRC treatment. However, bleeding, which was seen after 77.8% of procedures in our study, which was previously reported to occur frequently after LVRC procedures 37 and which led to one procedure-associated death in the RENEW trial, 8 is an inherent risk of LVRC treatment. On the other hand, pneumothorax, which was not seen in any patients in our study, is a major risk of endoscopic lung volume reduction with valves. Nevertheless, it has to be noted that there were no cases of respiratory failure requiring mechanical ventilation and no deaths in the patients with very low FEV1, neither in the two studies on endoscopic lung volume reduction with valves10,11 nor in our study on LVRC treatment.
The study has some methodological limitations. The interpretation of the results is limited by potential biases introduced by the retrospective study design and the small number of patients. However, outcome and safety profile of LVRC treatment in this selected and highly vulnerable subgroup of patients with emphysema and very low FEV1 were comparable with the overall results of previously published studies on LVRC treatment. Hence, further evaluation for LVRC treatment should probably not be withheld from patients otherwise qualified only due to the finding of very low FEV1. Prospective studies including more patients are now needed to further assess the value of LVRC treatment in patients with very low FEV1.
Conclusion
Lung volume reduction coil treatment could be performed safely and effectively in patients with very low FEV1. Within 3 months of follow up, it led to statistically significant and clinically relevant improvements in lung function and exercise capacity. There were no cases of respiratory failure requiring mechanical ventilation and no deaths. Hence, further evaluation for LVRC treatment should probably not be withheld from patients otherwise qualified only due to the finding of very low FEV1.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
MS and HK declare that they serve as advisors for PneumRx and have received honoraria for talks and workshops. None of the authors has any financial interest in the company.